Wondering how to get your newborn to fall asleep on their own? Get real-life tips on how to get your baby to sleep without being held.
My baby couldn’t sleep at all without being held.
It didn’t matter how deeply he seemed to be asleep in my arms, or how long I waited until I thought it was safe to put him down. Nor did it matter how or even where I put him down. He would wake up the minute he wasn’t held, look around, and fuss to get picked up once again.
And so, I ended up getting stuck with a sleeping baby in my arms, immobile for the duration of his sleep. I knew newborn babies liked to be held, but this much? I wished I could put him down, if not for nap time, then at least for the first stretch of sleep at night.
Because nothing is worse than when your newborn won’t sleep in the crib and only in your arms.
Table of Contents
How to get your baby to sleep without being held
Don’t worry, friend—nearly every mom can relate to this struggle.
Maybe your baby insists on being held all the time, leaving your arms tired from the weight. You have to nurse or rock him to sleep, only for him to wake up immediately when you put him down. It doesn’t help that you’re home alone with other kids who need you as well.
Now, we all know the newborn stage isn’t going to be perfect. But, if you’re like me, you’re desperate to see if there’s something you can at least try and do differently to make the situation easier.
But like many first-time moms, I had no clue what I was doing. I spent many sleep-deprived nights researching and reading what worked and didn’t work for other moms, hoping I could find my answers.
I tried several strategies, some that failed miserably, and others that actually worked. My son was still too young for sleep training, much less sleep through the night, but these strategies were helping him sleep longer stretches. Most importantly, I had my arms back, in some form or another.
So, what do you do when your newborn won’t sleep anywhere but your arms? Take a look at these strategies, and hopefully they can work for you as well:
1. Don’t keep your baby awake too long
I figured babies simply sleep when they’re tired, but I couldn’t have been more wrong. In fact, the times when I kept my baby awake for far too long were some of the most challenging times. Being overtired meant he had a difficult time falling asleep.
I later learned that babies can’t stay awake for too long. That once the window is up, then you really need to do whatever it takes to get them to sleep and reset their bodies.
One of the best ways to make sure your baby isn’t awake too long is to pay attention to his baby tired signs. For instance, any more than three yawns are cues that he’s overtired, so put him to sleep once he yawns.
The other way to ensure he’s not overtired is to simply watch the clock. Note when he woke up, and don’t let him be awake after a certain time period.
How long exactly is too long? Well, it depends on your baby’s age. You can grab this free resource where I share the age and sleep guidelines, as well as share more tips about your baby’s awake time. You’ll also get my newsletters, which parents say they LOVE:
“You have no idea how much your emails help me. Not many people are open and real about the newborn phase. All other women around me either don’t want to talk about it or have selective amnesia. Your openness is refreshing. I would announce to my husband when I received another Nina Garcia email and then eagerly read it, sometimes aloud. I appreciate the candidness, honesty, and purpose of your newsletters. -From an appreciative new parent, Jill Weathington”
2. Put your baby down drowsy but awake
We’re all creatures of habits and rituals, getting used to what we’ve always done or experienced. If your baby has always fallen asleep in your arms, then it’s no wonder he cries when he sleeps any other way.
The first place to start breaking those habits and sleep associations is by putting him down drowsy but awake. That way, he’ll get to experience falling asleep away from your arms, in the sleep environment he’ll eventually wake up.
After all, few of us can fall asleep in one place, get moved to another, and not wake up in the process. The same is true for your baby.
He’ll also learn that you don’t have to hold him to fall asleep. Again, he’s gotten so used to one way of falling asleep—in your arms—that any other way feels strange. By consistently putting him down drowsy but awake, he learns that it’s okay to fall asleep that way, too.
Sure, hold him in your arms, but once he starts looking drowsy, set him down where you want him to sleep so he can experience the transition for himself.
Learn what to do when your baby won’t nap unless held.
3. Let your baby sleep in a snug place
Disclosure: This article contains affiliate links, which means I will earn a commission—at no extra cost to you—if you make a purchase.
Babies find comfort in snug places, having spent so much time in the womb. While the crib is the ideal place to set your baby down, many parents have found more luck in other, snugger places. These offer the secure feeling of being “cupped” and held, just like in your arms.
Here are a few ideas:
Infant bouncer
Infant cushion
Baby wrap
Sleep suit
Swaddle
4. Keep the crib mattress warm
To go from your warm, cozy arms to a cold, hard crib can be a difficult transition for your baby.
To make the bed just as inviting, you can try placing a heating pad or a warm water bottle on the crib a few minutes before you plan to set him down. Of course, make sure to check that the bed isn’t too hot. Another option is to turn up the temperature in the room before you set him down so that it’s not too cold.
By keeping his crib warm, easing him out of your arms can still feel cozy.
Learn how to get your baby to nap in the crib instead of your arms.
5. Stroke your baby’s face
Worried that your baby will startle and throw a fit the minute you put him down awake?
Try this simple trick to help him relax: After putting him down awake, stroke his cheek and forehead until his eyes close. Maybe you caress his eyebrows or run your finger from the bridge of his nose to the top of his head. Gently stroke his cheeks, moving from nose to ear.
These simple touches can be all it takes to keep him in a drowsy state until he eventually falls asleep. Sure, he still needs your help to sleep, but at least you’re not holding him the whole time.
6. Keep your hands on your baby after putting him down
One of the sensations of being held is that contact with your body, the warmth on her chest as it presses against yours. But after you put her down, this warmth goes away, leaving her exposed.
To mimic that feeling, try a little trick to make that transition easier:
Put her down just as she’s about to sleep, but keep your cradling arm wrapped around her body and your other hand on her chest. If you can, you might even want to lightly keep your chest touching hers, as if you’re still hugging and holding her lying down.
Then, as she drifts off to sleep, slowly remove and slide your cradling arm from underneath while still keeping your other hand on her tummy. And finally, remove the other hand so she can sleep alone.
Learn 5 things you can do when your newborn wants to be held all night.
7. Use a pacifier if your baby fusses
As you set your baby down drowsy, you might notice fussiness. If he takes to a pacifier, this would be a good time to put one in his mouth to encourage sucking. Don’t wait until he’s crying hysterically—instead, insert the pacifier if you see him starting to squirm or get upset.
Then, keep your hand on him so he still feels you as you hold the pacifier in his mouth. This will remind him that you’re still there, while encouraging him to suck on the pacifier and fall asleep.
After you’ve left, keep the pacifier in his mouth. But if you notice him squirming once more (or you think he’s about to wake up), use the pacifier again:
If the pacifier fell out, re-insert it into his mouth.
If the pacifier is still in his mouth, give it a gentle “tug.” This will encourage him to suck harder and hopefully keep sleeping.
8. Use white noise or music
Keeping the room completely silent will only invite sudden noises to startle your baby awake. Instead, use white noise to muffle those sounds. Not only will they block those sounds, they’ll also remind him of the constant hum he heard when he was in your womb.
You might use an app or buy a white noise machine. Maybe you download and loop a static music file on your phone, or simply turn on a regular fan or heater. The white noise will add a constant hum to encourage continuous sleep after you put him down.
Some parents have also found success with teaching their babies to tie soothing music to sleeping.
Play music while you nurse at night so he associates it with comfort and drowsiness. Then, keep the music on as you put him down and let him sleep. Hopefully, he’ll stay asleep with the music still playing nearby.
Bonus tip: Add darkening curtains to his room to keep the room really dark.
9. Let your baby lie down awake
I mistakenly assumed that the minute my baby’s eyes flew wide open after putting him down, that I’d have to scoop him back up and re-do our bedtime routine. Only later with my twins did I realize that those were opportunities for him to fall asleep on his own.
Don’t feel compelled to pick your baby back up if he goes from sleepy to awake when you put him down. He just might be able to put himself to sleep, especially if you give him a chance to. And given that he’s not crying, you have even less reason to get him out of the crib or bassinet.
Instead, let him lie down, even if he’s awake. He might fuss a little, at which point you can try a pacifier or simply let him try to soothe himself. He just might surprise you—as my twins did—by falling asleep on his own.
Speaking of which…
When can babies fall asleep on their own?
Your pediatrician is your best resource to know exactly when your baby can fall asleep on his own. But in general, babies in the newborn stage—the fourth trimester, as they say—still need help falling asleep.
That said, you can still set good sleep habits even now that encourage him to sleep independently. Make every first attempt an opportunity for him to fall asleep on his own (for instance, by putting him down drowsy but awake each time).
And if he cries hysterically? Then yes, scoop him up and try something else. Maybe this time you’ll put him in the swing, carry him in a wrap, or try an infant cushion. And if he truly isn’t having any of it, then hold him in your arms to help him sleep.
He might still need help falling asleep a lot of times, but at least you’re consistently giving him a chance to do it on his own, too.
Can you spoil a baby by holding him too much?
“Spoiling a baby” is relative.
After all, someone who enjoys holding her baby to sleep every time would certainly not object to doing so. In fact, she might even feel guilty for holding her baby, assuming she’s doing a bad job by doing it so often.
So no, you can’t “spoil” a baby by holding him too much.
Instead, the better question to ask is this: What expectations are you willing to set?
If you’re okay with holding your baby, then by all means, continue doing so. But if you feel an imbalance between his needs and those of yours, your family, your work, and your home, then something needs to change.
It can be as simple as putting him down more throughout the day—when he is awake—so he knows it’s also okay to be away from your arms. And of course, applying the tips you learned here to get him used to sleeping without being held.
Conclusion
So, how do you get your baby to fall asleep on his own? We’ve learned that a lot of it is trial and error, but that it’s totally possible to make your baby sleep on his own.
Make sure you’re not keeping him awake too long, and that you put him down drowsy but awake. Let him sleep in a snug place, or warm his bed before you place him in it. Stroke his face and keep your hands and arms around him as you set him down.
Use a pacifier if he starts to fuss or wakes up earlier than you’d want him to. White noise and music can help muffle startling sounds and soothe him to sleep. And finally, let him lie down even if he’s awake—you just might find him having fallen asleep soon after.
Hopefully you’ve found that you can get your baby to sleep without being held, after all.
Get more tips:
How to Get an Overtired Newborn to Sleep
Newborn Not Sleeping? 9 Tricks to Help Your Baby (Finally!) Sleep
How to Burp a Sleeping Baby
What to Do When Your Overtired Baby Keeps Waking Up
How to Establish a Baby Nighttime Routine
Don’t forget: Join my newsletter and get One Mistake You’re Making with Your Baby’s Awake Time—at no cost to you:
How to Get Baby to Sleep in Crib • Kids Activities Blog
How to get your baby to sleep in the crib was something that many of us have struggled with over the years. If you have ever muttered the words through tired lips “My baby will only sleep in my arms “… you can breath a sigh of relief today. We have some time-tested baby sleep solutions that actually work.
Baby, why don’t you sleep?
Newborn Baby Won’t Sleep in Bassinet or Crib!
When your baby won’t fall asleep without you, it can be hard and then on top of that it might be in completely the wrong place!
I have been there, too, and it DOES stop.
Eventually, they do just fall asleep, without needing you right there to pat them, rock them, nurse them, feed them…
All four of mine are now falling asleep all by themselves and yours will, too.
Eventually they will sleep…
Baby Only Sleeps When Held
It may start by accident. You nurse or bottle feed your baby, just to get a few extra minutes of sleep yourself, and then it becomes a habit.
You bring your baby into your bed so you can get the sleep that your body is craving and you both sleep well, so you do it again. When you try to stop, your baby cries and cries.
What do you do now?
Take the advice from these real moms… who have been where you are right now.
How to Get Your Baby to Sleep without Being Held
The truth is that this happens more often than you might think. Even babies who are considered “good sleepers” have occasional off-days and nights where they only want to sleep in someone’s arms.
1. Continue Sleeping in Arms with a Twist
Remember that this is very normal and natural for your baby to want you. You may be in “survival” mode right not- trying to get sleep where you can.
“Just do what feels right to you, feed to sleep, cosleep, do what you can to get the most sleep and least crying… They are only babies for 365 days which will pass in the blink of an eye. Do what you can to enjoy it while it lasts” ~Rebecca
If you aren’t comfortable co-sleeping, remember that it only takes three days to break a habit.
Three days!
One thing that helped me was to put my baby down in the crib and then time how long he cried. I know this sounds nuts and a little cruel, but what I found was that it was always less than a minute. It seemed like an hour! But when I actually timed it, he cried for less than a minute and then would sleep longer and more soundly than if he was in my arms.
2. Prepare the Crib for Baby to Sleep
Try making the crib warm by placing an electric blanket on his sheets for 10-20 minutes BEFORE you put your baby into his crib. Remove the blanket right before bedtime (you never want to leave it in the crib). It will warm the sheets, which will make sleep come easier. (Think of it like this: you are a warm body, so if he is resting on you and moving to cold sheets, a drastic change in temperature can be startling)
Try putting a crib beside your bed and hold your hand in on your baby’s belly until he/she falls asleep.
Try a co-sleeping bed or crib (many stores sell these)
3.
Positioning Baby for Success
If you want your baby to sleep on his back, hold him on his back when you are snuggling him. It will make the transition easier to the crib or bassinet.
4. How to End Co-Sleeping
If you have been co-sleeping and need to make a change for some reason, here is Sherry’s story that is encouraging and real:
“I couldn’t even get out of bed to brush my teeth and he’d start moving & crying! At four months it was becoming challenging because he would wake up every 30 minutes all night and all day I also have a three-year-old and it was very hard to co-sleep and also get her to bed! My husband and I decided it was time to get him out of our bed at 4 1/2 months… a few rough nights of crying and going in to comfort him to show him that his crib is where he sleeps and he’s been doing wonderful!! He’s now almost six months old and sleeps 11 hours in his crib!!! You have to do what works for you and not worry about it!! I thoroughly enjoyed cosleeping but it was definitely our time to end it. ”~Sherry McQuay
Try placing the baby in their crib while you are awake, to avoid them temptation to co-sleep due to YOUR sleepiness. A good way to do this is by starting at nap time.
5. Baby Will Only Sleep in Swing
I had one of these kids too…that went through a phase where he only wanted to sleep in the swing as it was swinging. It was easier for me to let him fall asleep in the swing than endure the screaming as I took him out to his bed.
For awhile I justified that the swing would stop and he would stay asleep.
But sleeping in a swing is not a very good longterm solution! All I can think of is how I am going to need a larger and larger swing {Giggle}.
First, look at what is going on and if the problem of your child sleeping only in the swing is minor compared to other stressful things that might be happening, then giving it another day or two is fine.
I always said there is a season for everything.
Once you are ready to start weaning baby from sleeping in the swing, then start to distance falling asleep from the swing. Place your baby in the swing until eyelids get heavy. Then start removing him earlier and earlier in that process to eliminate the association of sitting up and swinging with sleep.
It took less than a week to make the transition this way…so hang in there.
6. When Baby Will Only Sleep in the Car
Like the swing, some babies will only sleep in the car…and some only when it is moving! This is more common than you might think and it requires a similar, but more abrupt ending since driving your car every time your child needs sleep is certainly a short term solution!
Find other ways to mimic that motion whether it be pushing the stroller or placing the carseat in a wagon, etc. And then pre-empt the actual falling asleep with a move to the crib or bassinet.
This will work. It just will be a little noisy at first.
7. Try Swaddling If it is an Option
The AAP guidelines for swaddling is to stop swaddling at 2 months or when your baby starts to roll over intentionally. This is a bit controversial since many moms have swaddled for up to 4-5 months as did I. The concern is that your baby would become entangled in the swaddling and not be able to move to breathe. So look at what is happening and what supervision you can give to make your decision.
Swaddling works because the baby feels safe and secure tucked in. Think of how a baby could feel like it is falling when placed on their back after being tightly secured in the womb for such a long time.
8. Start as You Mean to Go
I probably repeated those words a million times when my kids were little. Start as you mean to go.Start as you mean to go. Start as you mean to go.
I read this is a book that I loved (The Baby Whisperer) and it holds true for every situation. Don’t do something that you don’t intend to keep doing.
You are training your children one way or another.
It helped me see how what may seem small and inconsequential on any given day actually builds up over time in baby steps to the bigger picture.
9. Routine! Routine! Routine!
Put him down for naps and bed at the same time each day. You may need to wake them in the morning to try to keep this schedule.
Keep a structured routine, so his body becomes used to sleep at the same time.
10. Tips for Getting Baby to Sleep
Try making a “sh, sh, shhhh… sh, sh, shhhh…” sound as you keep your hand on his chest. This sound reminds them of being in the womb.
If he cries when you try to put him into his crib, pick him up until he is calm and then immediately place him into his crib again.
OMG. This too shall pass, my friend. I remember going through this with each of our four children. I remember it like it was yesterday, but it does get better and easier.
You are tired now, but you will get sleep again.
You can find more solutions and ideas here at Kids Activities Blog where we share real mom solutions every day…
Activities for the other kiddos
What have you found works to get your baby to sleep in the crib? What tips do you have that we missed? Have you found ways to help your child sleep when they get older, like toddler, 1 year old, 18 month old, or even preschooler?
Why Some Babies Want to be Held While Sleeping
NewFolks may earn a commission when you buy through links on our site.
If your newborn wants to be held all night, you need these tips and tricks
By
Vin D’Eletto
Finding peace and quiet, or simply trying to take a shower, while caring for a newborn can be difficult. If your baby only sleeps when held, completing the smallest tasks can feel impossible. What can a parent do when their newborn wants to be held all night? Newborns love being held for many reasons.
Contents
Why babies want to be held while sleeping
Comfortable ways to hold babies while sleeping
How and when to put your baby in their crib
Tips for sleep training your baby
Learn more about why your baby wants to be held, the best way to hold your baby, and when to put them in their crib. Just because your newborn wants to be held all night, doesn’t mean you can’t get any sleep.
Why babies want to be held while sleeping
Monkey Business Images/Shutterstock
The relationship between a parent and their baby is complex and beautiful. While cuddling, your baby can actually hear your heartbeat, and your presence is soothing. Babies also smell your scent when you hold them, making them feel safer.
When your baby is under four months old, they’re still getting used to life outside the womb. The new surroundings can be scary and unfamiliar. It’ll take time for them to become accustomed to this new environment, and when parents hold their babies, they feel warm and safe — just like in the womb.
However, when your baby falls asleep in your arms too often, it can become a habit that’s hard to break. Your baby might associate sleeping with being in your arms and will consequently have trouble sleeping anywhere else, like their own crib.
Comfortable ways to hold babies while sleeping
Holding a baby isn’t challenging, but sometimes it can be difficult to find an agreeable position while they’re sleeping. Here’s a breakdown of a few positions that are often very comfortable for babies to sleep in.
Cradling
Cradling a baby may just be the most common position for holding your baby. It tends to be a natural holding position and is quite simple. Your baby’s head will gently rest in the crook of one arm while your other arm is wrapped around them, securing your baby while they sleep. Cradling makes rocking your little one to sleep easy.
On your shoulder
Another classic baby-holding position is on your shoulder. Let your baby lean their cheek against your shoulder while you support their bottom, as well as their back and neck. This position may make it easier to gently bounce your baby to sleep. Your baby will be able to hear your rhythmic breathing and heartbeat, too, so it’s a relaxing and comforting sleeping position for them.
In a sling
Using a sling is also helpful for sleeping babies. It lets you hold your baby hands-free while giving your baby the comfort of being held. They’ll be able to stay close to you, but you’ll be able to do other things while your baby rests.
Remember, you shouldn’t hold the baby while you’re standing up, just in case they fall. Don’t hold your baby if you’re sick, and only carry one baby at a time if you have multiples.
How and when to put your baby in their crib
Although it entirely depends on when you, as a parent, feel ready to introduce your baby to their crib, a good time to do so is around six months old.
Use the crib for naptime
You can start the transition into their crib by using it during naptime. When it’s time for your baby’s nap, star by placing them in their crib. Introducing your baby to their crib during naptime will help them get used to sleeping in it at night.
Your baby’s behavior will let you know when they are ready to go to sleep. Common sleepy symptoms include becoming fussy, yawning frequently, rubbing their eyes, or looking away. If you notice one or more of these behaviors, they’re probably ready to go to sleep.
Make sure you place your baby in their crib when they’re sleepy but not actually asleep. If they wake up during the night, comfort your baby by patting them, but don’t take them out of their crib because that will negatively affect their routine.
Use technology for support
For added comfort, you can try adding a white noise during your baby’s sleep routine. White noise machines can block out other sounds and disturbances. This can be especially helpful if your baby is sleeping in a crib in your room.
Transitioning your baby to a crib can be more difficult for you than for your babies. Using a baby monitor can help ease your mind if you’re a parent anxious about your baby sleeping in their own crib in a room by themselves. There are even some mobile applications that can turn your tablet or phone into a baby monitor.
It’s completely normal if your baby doesn’t sleep through the night yet. Once your baby is about five months old, they may be able to start sleeping around seven hours per night. As your baby starts to inch into infanthood you may no longer have a baby who wants to be held all night.
Tips for sleep training your baby
Try swaddling
During the first few weeks, your baby is adjusting to the “outside world” after dwelling in a snug, warm environment for the last nine months. Naturally, re-creating that safe space can help if your baby only sleeps when held.
Swaddling is the best option when it comes to soothing your baby to sleep, especially during the first two weeks. In the womb, your baby was accustomed to having limbs tucked in and snug. When you swaddle your baby, you’re placing them in a similar position, particularly with what’s called the “burrito wrap,” which is the most common form of swaddling.
Incorporate white noise
Using white noise during sleep also works well with swaddling. The soft humming and swooshing closely resembles the sounds from the womb. Your baby is reminded of the secure and comfy environment from where they just arrived. Plus, it helps your baby adjust during the more difficult sleep cycles and helps them stay asleep longer. A device like the Letsfit White Noise Machine provides an effective option when your newborn won’t sleep unless held.
Although the process can be frustrating (and exhausting), remember that babies don’t learn to fall asleep on their own in a day. It takes time and repetition. The best thing you can do for yourself and your baby is to remain patient. There are parent support groups that you can seek out for reassurance.
Editors’ Recommendations
5 telltale signs your child is struggling in school (or will be) – and what to do to help
Can you take cold medicine while nursing? What you need to know about what to avoid
6 best Facebook groups for nursing moms
Help! My teenager is vaping! Why this is a high-level parenting emergency
5 reasons reversible strollers are an excellent purchase for new parents who are on the go
Separate sleep with mother threatens the child with mental disorder
Babies who sleep in their crib already in the first month of life suffer from rapid heartbeat – the heart muscle tenses three times more, which in the future can lead to a number of diseases. Nils Bergman, a professor of pediatrics at the University of Cape Town, came to this conclusion by tracing the relationship between the joint sleep of a newborn with his mother and his further physical development. The results of the study were published in Daily Mail .
In addition, the brain of a baby who sleeps separately from the mother before the age of four weeks develops more slowly, says Bergman. The reason for everything is the stress that a newborn experiences, being alone for a long time.
Nils Bergman conducted a study of 16 infants. Some of the children slept on their mother’s chest, and the other – in a separate bed nearby. It turned out that the children in the crib experienced stress, the level of which was three times higher than in children who slept with their mother. In addition, infants who slept separately were less likely to alternate between slow-wave and REM sleep, while the alternation plays a key role in brain development. Thus, Bergman encourages mothers to put their baby on their chest for the first three to four weeks and to sleep in the same bed until 3-4 years of age.
Newly made fathers may not like this news, and they will easily find refutation of Bergman’s conclusions, for example, in the theory of Sigmund Freud’s Oedipus Complex. The famous psychologist argued that in children aged 2-4 years, a sexual attraction to a parent of the opposite sex is formed, and close contact, which includes joint sleep, can increase this attraction. However, psychology, like medicine, does not stand still, and today Russian experts assure that the separate sleep of an infant under the age of four weeks threatens him not only with the development of physiological pathologies, but also with a mental disorder, told the correspondent of “MIR 24” psychologist Larisa Surkova.
“There are serious cases when parents, frightened by grandparents or doctors, at any cost begin to transfer the child not only to a separate bed, but also to a separate room. Today it is a very fashionable trend. Thus, parents separate very young children from themselves. Although the first four weeks of a child’s life are not accidentally called the tenth month of pregnancy, they are very important.
There is a theory of attachment which says that for the first four weeks the baby should be as close to the mother as possible. The mother must literally tie him, carry him in her arms, put him on her chest, in a word, do everything so that he wears, even if the child was born full-term. When parents begin to move their children to another room, because someone told them that they would later have serious pathological problems with their children, through the cry of a child, through sobbing, using some traumatic methods, then psychologists really will subsequently have to sort out children’s Problems. Such children at the age of four or five begin to have serious mental problems, because there is a violation of the basic attachment. It’s a lifelong trauma.
For a child, such actions of parents mean the loss of a mother. He does not understand at this moment that his mother has gone into the next room, he is losing her. And every time he loses her forever. Therefore, I would like to urge parents, first of all, to listen to their hearts. If you are a mother, sit under the door of the room where the child is crying, while you are crying yourself – spit on the advisers, hug the child to you and give him your best. Childhood will pass very quickly. You only need to listen to your mother’s heart, ”says the psychologist.
Experts believe that the best option today is a separate bed, which is attached to the parent’s bed on the mother’s side.
“In an ideal scheme, when the child’s bed is in close proximity to the adult bed, certain boundaries are created, and at the same time, the mother is nearby, the child is calm, he hears her heart and breath. At the same time, it is convenient for the mother to feed the child, she does not have to get up for this a hundred times a night. Everyone gets sleep. If initially the mother slept with the baby in the same bed, then there will be no problems when switching to a new scheme. Over time, the child will begin to send signals to his mother about his readiness for independent sleep. The first time it happens usually at the age of 9-10 months. The child begins the phase of deep sleep, and joint sleep during this period can play a negative role, since the mother has already developed anxiety. For a child, this is the age at which he is already ready to sleep in his own bed, but not in a separate room. If you see that the baby has longer periods of deep sleep, when he does not wake up for a long time, when he eats less often, then you can already safely transfer him to a separate bed, ”Surkova comments.
The stages of separation of the child from the parents should be smooth and gradual, in this case the psyche will not suffer. First, you need to transfer the child to a separate bed, and only when he gets used to it, move this bed to a separate room. To form a child’s interest in their own sleeping place, it is necessary to use bed linen with children’s ornaments, children’s toys, therapeutic fairy tales and nightly rituals.
“Often, parents rudely push the child away from them. For example, a mother is waiting for the second, say, she will give birth tomorrow, and suddenly she decides that it is time for a two-year-old child to sleep separately. The child immediately moves to the next room through tears and stress. Sometimes it happens that the child slept in a side bed, but suddenly he is told that now he has grown up and this bed is no longer his, but a new brother, and now he needs to sleep on a bunk bed in the next room. In this case, the child has two stresses at once – the appearance of a new child and the selected position that is familiar to him. And sleep is very important. Sleep and food are basic human needs, so it is very important that in childhood they are carried out in a calm environment so that nothing injures the child. It is important to do everything very gradually, ”the psychologist shares his advice.
Reverse theories about the dangers of co-sleeping mother and child have no practical evidence. “Old Freud” at one time fantasized too much, modern psychologists are sure.
“During my practice, I have not seen any pathological cases due to the joint sleep of mother and child. Of course, there are setbacks. For example, a child from birth sleeps in his bed on his own, everything is fine with him, and at 9-10 months he begins to ask his mother at night, because his teeth are climbing or something else is bothering him. Then, at two or five years old, ask to go to bed with your parents, because, for example, you had a bad dream or fears appeared. There is no need to push the children away at these moments. No need to take the child back to his room and scare it even more there. It is quite possible to give the child an indulgence by laying him next to you, and in the morning to figure out what happened at night, ”advises Larisa Surkova.
Hunger, pain or the weather: what prevents children from sleeping?
Lace blankets in a snow-white bed, tiny booties on a changing table, an impeccably furnished children’s room… Every family awaits the birth of a baby with special reverence. But the expectation of a beautiful fairy tale of serene parenthood is very often replaced by a harsh reality with sleepless nights, children’s crying and the hope that the colic will soon pass and it will soon become easier. Colic passes, and restless children’s sleep with long bedtimes and frequent awakenings often remains the main problem of young parents. What prevents the child from sleeping at night and how to fix it? Authoritative experts answered this question.
Ekaterina Taran, psychologist, consultant at the BabySleep Center for Child Sleep and Development:
“From the moment of birth to the age of two or three, every child goes through tremendous emotional and physical changes – they learn to roll over, sit, stand up, walk. Growth spurts are replaced by development spurts, the daily routine also changes. And you need to understand that in a normal healthy child under three years old, one to three awakenings are acceptable, but perhaps not every night.
Talking about the causes of poor sleep and frequent nighttime awakenings, first of all, we can highlight physical discomfort: hunger, an overfilled diaper, pajamas that may be oversized or with chafing seams or tags made of fabric that irritates the skin. External factors – noise, light, humidity, heat or cold – can also interfere with the baby’s sleep. As soon as the cause of physical or external discomfort is eliminated, full sleep returns.
Developmental and growth spurts also affect children’s sleep. For example, a baby learns to sit down, and he trains this skill at any time convenient for him, including at night. Only training the skill during the active time of wakefulness will help here, bringing it to automatism.
A fairly common cause of poor night sleep is an incorrectly structured daily routine. This is too much, not enough, emotional overexcitation before going to bed, lack of rituals. Here it is necessary to adjust the daily regimen according to age, taking into account the individual time of wakefulness of the child.
Next: causes associated with sleep associations. If a child falls asleep during feeding, rocking, or sleeps only in a stroller, then, waking up between sleep cycles, he will not be able to fall asleep on his own and will require the restoration of familiar conditions. There is an opinion that breastfeeding or motion sickness is a harmful association for sleep, but here, first of all, you need to look at the age of the baby. For newborns, it is very physiological to fall asleep “on the chest” – the mother is developing lactation, frequent long applications are very important. Yes, and rocking in the first three months will soothe the baby. By six to eight months, such conditions for falling asleep become familiar to the child, and often mothers do not change anything and do not introduce other methods of relaxation. And now such associations for sleep begin to interfere, because, for example, pumping a one-year-old child is no longer so easy.
Of course, every case is different. But there are some general recommendations on how to make a child’s sleep sound and parents’ nights calm.
Analyze if your child’s daily routine is appropriate for their age (if they go to bed too late, stay awake for a long time, have too much or not enough daytime sleep, etc.). It is very important to keep track of your baby’s wake time. For each age, there is a sleep norm that parents need to know. The main criterion is the mood of the child. A smiling baby who falls asleep well, wakes up without tears, sleeps for an hour or more during the day, is actively awake, perfectly regulates his cycles. Mom should listen to her child and, if necessary, increase or decrease the time of wakefulness.
Come up with a bedtime ritual – a set of the same actions repeated one after another in a strictly defined sequence before each bedtime. The ritual sets the baby to sleep and saturates with the attention of the mother. Very often there is a ritual for night sleep, but it is absent for daytime sleep – and this is a mistake.
Remove distractions and lights from the room while your baby is falling asleep. Many parents put a musical toy or their mobile phone in the crib. But toys with sound and light distract the child from sleep too much. At three to four months of age, the “sleep hormone” melatonin begins to be produced in the body. The level of this hormone in children increases in the evening, reaches a maximum around midnight and decreases in the early hours of the morning. The production of melatonin depends on the light – it stops in bright light. In the evening, shortly before putting the child to sleep, it is recommended to dim the lights, and in the process of the bedding ritual, turn off the light altogether. Thus, parents competently set up the child for sleep and reduce the time of bedtime.”
Evgeny Verbitsky, head of the Rostov branch of the Russian Somnological Society, professor of the Southern Scientific Center of the Russian Academy of Sciences:
“As a rule, after six months, the child’s nervous system makes a leap in development, which can also affect his sleep. From this age, the baby may wake up suddenly, with anxiety and crying. This is the so-called physiological crying, it is preceded by a shallow sleep. Often the child thus tries to call his parents, without whom he is uncomfortable and anxious. The baby needs to be made clear that the parents are nearby, they will come and calm him down, but without feeding, playing, without taking him out of the crib. Smooth stroking, repetition of ritual elements, soft humming in most cases return the child to sleep. Perhaps some thing in the crib that the baby saw at the parents and which smells of them will help him with this.
The child is growing, his bed is changing, his environment is changing, and you need to get used to it. If this habituation is successful, the level of children’s anxiety is reduced. The main cause of early childhood anxiety is associated with separation from parents, habitual habitat, environment, familiar elements of the children’s world. All this can lead to difficult falling asleep and a restless night’s sleep. “Intermediaries” in the form of night toys are effective here, as well as firm beliefs like “See you in the morning, baby.” Nightmares can also be the cause of awakenings. Parents should agree on what strategy to follow when the child wakes up and comes to bed with them.
Speaking of bad children’s sleep, it is worth considering the geographical features of the Rostov region. In our steppe region, the direction of the wind and its speed often change. This leads to changes in atmospheric pressure and sudden changes in the weather. A child is more sensitive to such changes than a healthy adult. Therefore, on rainy days, the baby’s sleep, with its still immature nervous system, must be treated with special attention.
The immature mechanisms of a child’s sleep are also vulnerable in the autumn-winter period – the production of the “sleep hormone” melatonin is affected by a short daylight hours. At this time, adults need to monitor the organization of the sleep and wakefulness of the child. This is a constant exam of parents for ingenuity and balance for the sake of deep sleep of the baby – the key to the production of somatotropic hormone, which is essential for the growth and harmonious development of the child’s body.
Natalia Tokmak, osteopath:
“In some cases, difficulty falling asleep can be an important sign for parents that there is some kind of problem. There are few such children in my practice. They have a normal competent regime, they go to bed on time, do not get overexcited, there are no vivid impressions before going to bed. The problem of heavy falling asleep may be associated with a violation of the positions of the cervical vertebrae. How does it affect nighttime sleep? Due to impaired blood flow and chronic spasm in large or small vessels of the brain, the regulation of brain structures is difficult. Poor sleep can be directly related to the “work” of the skull. Small, outwardly insignificant, but very important inside microdisplacements, microrestrictions in the mobility of the bones of the skull lead to a certain tension of its structures. It’s hard for these kids to relax. The transition from wakefulness to sleep is difficult for them. As a rule, they sleep restlessly, often waking up.
If we are talking about children under one year old, waking up screaming or crying is not a good sign. After all, a healthy child wakes up calmly, just gently lets you know that, for example, he is hungry. If the child immediately screams loudly (and the parent understands that this is a cry of pain) – most likely, he has a headache, it is difficult for him to relax, calm down, the baby has to be rocked. These kids need help. The osteopath can gently work with the cervical region, spine, sacrum. Although the sacrum is located far from the head, it is an important paired structure that “works” in sync with the skull.”
Tatyana Valkova, pediatrician:
“One of the main causes of children’s shallow sleep, which parents often neglect, is the lack of a normal microclimate in the room. The most comfortable air temperature for children of any age is 19-20 degrees. At this temperature, children’s sleep is most profound. If the mother is afraid that the baby will freeze, you can cover the baby with an extra diaper, but do not raise the temperature in the room. Humidity should be 50-70%. High temperature and low humidity of the room lead to the drying of the nasal mucosa, a decrease in immunological protection, the appearance of thirst, which provokes frequent nocturnal awakenings.
In conclusion, I want to say that you should not try to treat infantile sleep disorders with medication, since most of the drugs used in our country (nootropic, vascular and some others) are drugs with unproven effectiveness and are not used in developed countries.”
What is normal breastfeeding? | Interview with Dr. Jacqueline Kent
It can be difficult for new mothers to understand if breastfeeding is going well, so we decided to ask the expert if it is possible to talk about the norms when it comes to breastfeeding.
Share this information
Dr Jacqueline Kent , Research Fellow , Hartmann Human Lactation Research Group: Jacqueline joined the University of Western Australia research group in 1986 and received her PhD in 1999. She is currently researching the biochemical and physiological aspects of breast milk synthesis and release in search of scientific information to help mothers breastfeed longer.
Dr. Jacqueline Kent and her colleagues have been studying breastfeeding for many years. As it turned out, for all mothers and babies, this process occurs in its own way.
What were the most unexpected results of your research for you?
Variety. It turns out that the limits of the norm are extremely wide. We are used to textbooks that say that an infant should eat 8-12 times a day and gain 150 grams per week. But babies don’t read textbooks and do things their own way! Some gain weight more slowly, others very quickly.
We looked at infants aged one to six months who were exclusively breastfed. As our studies have shown, on average, a child is breastfed 4 to 13 times a day, and the duration of one feeding varies from 12 minutes to 1 hour. 1
How much milk do breastfed babies usually consume?
According to our research, the volume of milk consumed by baby ranges from 54 to 234 ml per feeding. 1
Sometimes it seems to the mother that the baby has eaten well, but when weighed, it turns out that he ate very little milk. And it happens the other way around: the child is distracted, breastfeeds for only a few minutes and still eats 100 ml of milk. Even if the baby is restless, this does not mean at all that he is malnourished.
All babies are different, but they all get the amount of milk they need in one way or another. One needs 500 ml of milk per day, while others eat up to 1356 ml!
By the way, boys on average eat 76 ml more milk per day than girls. The main thing is that you have enough milk, and the baby will decide when and how much he will eat.
Should I offer my baby a second breast?
I advise offering the second breast to the baby after the first has been completely emptied. If he accepts it, then he hasn’t finished eating. If not, don’t worry. Let the baby decide for himself – only he knows when he is full. According to our research, 30% of babies get enough milk from one breast, 13% eat from two breasts at each feed, and 57% from time to time. 1
How do you know if a baby is getting enough milk?
In my experience, mothers often blame themselves for not producing enough milk. Ask yourself: Is my child growing? Is he putting on weight? Is he cheerful? Is his skin healthy? How often does he get diapers dirty? If the answer is “yes”, then the baby is getting enough milk, no matter if he eats a lot or a little.
What is the most common misconception about breastfeeding?
Mothers usually think that the older the child gets, the more often you need to feed him and the more milk he will eat. They are often surprised to learn that between the 4th and 26th weeks, total milk production normally does not change. 2
In the first few months, the baby grows very quickly and his metabolism is accelerated. The milk that the child consumes during this period is almost completely used for growth and maintenance of metabolism.
Between the ages of three and six months, metabolism slows down and growth slows, so the same amount of milk is sufficient for the baby. In other words, the baby does not have to consume more and more milk as they grow older. On the contrary, feedings become shorter and less frequent, but at the same time the child receives the same amount of milk, because he suckles better.
Do studies say anything about the age at which breastfed babies start sleeping through the night?
Most babies need to be fed at night. A baby’s stomach is not big enough to go all night without a feed, and breast milk is digested very quickly. Therefore, it is natural for the baby to wake up at night – and this usually continues for at least the first six months. Feeding at night is normal. When you feed your baby at night, do not even hesitate – all over the world at this moment other mothers of babies of the same age are doing the same. Be patient – it usually only lasts a few months. 1
What worries new mothers the most during the first few weeks of breastfeeding?
The most common concern is whether the baby latch on correctly, sucks well, and is full during feeding. Often mothers also worry about sore nipples. The main thing is to find the right position for feeding from the very beginning and ensure that the baby is latching on correctly. Practice shows that this significantly affects the flow of milk and the convenience of feeding.
What breastfeeding symptoms should be of concern?
Milk production usually returns to normal levels two weeks after birth. If the child does not begin to gain weight on the fifth or sixth day of life, it’s time to sound the alarm. You should contact your doctor to make sure that milk is being produced and that its composition is changing from colostrum to mature breast milk.
What advice would you give to a new breastfeeding mother?
Try to have skin-to-skin contact with your baby as soon as possible after delivery. If possible, feed your baby within the first hour of life, or at least breastfeed. As soon as possible, contact a specialist to correct the position and grip of the breast during feeding and thus avoid damage to the nipples.
Feed frequently. Young mothers do not immediately succeed in correctly recognizing the signals that the child gives. Be sure to feed your baby on demand, and not at set intervals. Offer the breast as soon as you notice any signs of hunger – as a rule, the baby suckles better when he is calm. If he cries, it is more difficult for him to take the breast. If you are not sure what the child wants, offer him the breast. He decides whether he wants to eat or not.
To learn more about Dr. Kent’s research, download infographic “How to determine the limits of the norm when it comes to breastfeeding” or see it below.
Literature
1 Kent JC et al. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics . 2006;117(3): e 387-395. – Kent J.S. et al., “Amount and frequency of breastfeeding and fat content of breast milk during the day.” Pediatrix (Pediatrics).
As parents, we are used to our babies mouthing and drooling! Drooling is a sign of teething, so it is very common for babies to have excessive saliva in and around their mouths from infancy up until 2 ½ years old. When teething stops, at around 2 1/2 years, drooling becomes less evident. This is because children develop more muscle control, coordination and awareness as they grow. Drooling should not persist past 4 years of age and if it does, there may be one or several factors operating behind the scenes.
Extra saliva in the mouth has been known to cause speech delays, skin breakdown, sleeping issues, swallowing difficulty and social impact. Here are 7 reasons why your child may still be drooling,
Low Tone in Oral Mechanism: Children develop at different rates, and sometimes the muscles in the neck and face have not developed in time with the child. Low tone can certainly affect posture, which has a direct impact on control of saliva. If a child has low tone in their mouth or neck muscles, they could potentially have issues managing saliva in their mouth and swallowing it. They may also have a tendency to choke on their own saliva, liquids and solids, which should be addressed by a speech-language pathologist.
Reduced Sensation or Awareness: Simply put, your child may need to be reminded to close their mouth! If this remains a persistent issue with a child, he or she may have reduced sensation around their mouth and not be aware! This is where the speech pathologist can help the child to improve his/her awareness using various techniques (e.g. mirror, sour tastes, wiping).
Not Swallowing Frequently Enough: The act of swallowing does not necessarily come naturally for some children. Speech pathologists work with children to teach them not only how to swallow correctly, but when to swallow. In addition they can help the child build awareness for closed lips and feeling if their chin is “wet” or “dry”. If a small child is busy playing they may not always remember to swallow, causing saliva build up.
Enlarged tonsils/adenoids: Has your child had repeated strep virus, noisy breathing when sleeping or choking/gagging episodes? Excess drooling can be a sign of enlarged tonsils or adenoids. Often children with these issues will keep their mouth in an open position much of the time to free up their airway. An ENT can take a look at these structures and determine if there is a negative impact on ease of breathing. Once the breathings issue(s) are addressed, speech therapy can begin.
Underlying Allergies/Nasal Blockage: In a similar vein to #4 – excess saliva can be a sign of allergies or nasal blockage. If a child cannot use their nasal passages to breathe with ease, they will assume an open mouth position, causing excess saliva to form. This can lead to mouth and skin rashes, speech issues, frontal tongue placement as well as sleeping problems.
Undetected Tongue Tie: If a child has an undetected tongue tie, it may make it difficult for them to properly swallow their saliva. This tongue tie may not have been seen at birth, but as a child ages, it can cause a restriction in movement, leading to difficulty with managing saliva and concurrent speech issues. Tongue ties are not always obvious and a preferred provider in tongue tie can rule assist the speech pathologist in ruling out a restriction.
Narrow/High Palate: Your child may have either a narrow palate and/or high palate, which can certainly cause the tongue to shift forward, since there is no place for it to rest. When the tongue doesn’t have a landing place within the palate, the tongue has a more work to do to move back in order to swallow. Speech-pathologists have background training in identifying these types of palates and regularly refer to pediatric dentists and orthodontists.
Did you realize that there could be so many possible underlying reasons why your child is drooling? If you notice that your child is having difficulty managing their saliva, give us a call today and we’d be happy to work with you on figuring out why it’s happening. If you have any questions or confusion feel free to reach out and ask me any questions at This email address is being protected from spambots. You need JavaScript enabled to view it.
Latest Articles
How Can I Expand My Child’s Attention and Language?
22 October 2018
WHY is “R” So Hard to Say?
02 January 2018
I CAN’T UNDERSTAND MY CHILD…WHY?
28 November 2017
Children’s Speech: When Should a Parent be Concerned?
26 July 2016
Why Is My Child Drooling?
28 March 2016
MY CHILD HAS A LISP
23 January 2016
TIPS FOR YOUR PICKY EATER- Part 1
11 August 2015
How to Adapt Books for Your Child!
17 July 2015
Toys For The Holidays that Help Langauge Development In Young Children
06 December 2014
Is Your Child a Picky Eater or Problem Feeder?
18 November 2014
Formula Feeding FAQs: Some Common Concerns (for Parents)
Whether you plan to formula feed your baby from the start, want to supplement your breast milk with formula, or are switching from breast milk to formula, you probably have questions.
Here are answers to some common questions about formula feeding.
Is it Normal for My Baby to Spit Up After Feedings?
Sometimes, babies spit up when they have eaten too much, burp, or drool.
Many infants will spit up a little after some — or even all — feedings or during burping because their digestive tracts are immature. That’s normal.
As long as your baby is growing and gaining weight and doesn’t seem uncomfortable with the spitting up, it’s OK. The amount of spit-up often looks like more than it actually is.
But spitting up isn’t the same as forcefully vomiting all or most of a feeding. Vomiting is a forceful ejection of stomach contents. Spitting up is a more gentle flow out the mouth or nose.
If you’re concerned that your baby is vomiting, call your doctor. Keep a record of exactly how often and how much your baby is vomiting or spitting up. In rare cases, there may be an allergy, digestive problem, or other problem that needs medical care. The doctor should be able to tell you if it’s normal or something of concern.
How Can I Keep My Baby From Spitting Up?
If the doctor says your baby’s spitting up is normal, here are some things you can do to help lessen it:
Burp your baby after your little one drinks 1–2 ounces from a bottle.
Don’t give the bottle while your baby is lying down, and keep your baby’s head above their feet.
Keep your baby upright after feedings for at least 30 minutes. Holding your baby is best. The way your baby sits in an infant seat can make spitting up more likely.
Don’t jiggle, bounce, or actively play with your baby right after feedings.
Make sure the hole in the nipple is the right size and/or flow for your baby. For example, fast-flow nipples can make babies gag or may give them more milk than they can handle at once. Many breastfed babies do well with a slow-flow nipple until they are 3 months old, or even older.
Raise the head of your baby’s crib or bassinet. Roll up a few small hand towels or receiving blankets (or you can buy special wedges) to place under (not on top of) the mattress. Never use a pillow under your baby’s head. Make sure the mattress doesn’t fold in the middle, and that the incline is gentle enough that your baby doesn’t slide down.
Most babies grow out of spitting up by the time they’re able to sit up.
How Do I Know If My Baby Has an Allergy?
Some babies are allergic to the protein in cow’s milk formula. Symptoms of an allergic reaction may include:
vomiting
diarrhea
belly pain
rash
blood or mucus in the baby’s poop
If your baby has any of these symptoms, tell your doctor. Also talk to the doctor before switching formulas.
If your baby has symptoms of a severe allergic reaction — like sudden drooling, trouble swallowing, wheezing, or breathing problems — see a doctor right away.
Is Soy Formula Safe for My Baby?
Store-bought iron-fortified soy formula is safe and nutritionally complete. Doctors usually recommend soy-based formulas if:
Parents don’t want their babies to eat animal protein.
A baby has congenital lactase deficiency, a rare condition where babies are born without the enzyme needed to digest lactose. Lactose is the main sugar found in cow’s milk.
A baby is born with galactosemia, a rare condition where babies can’t digest galactose. Lactose is made up of glucose and galactose.
Many babies who are allergic to cow’s milk also are allergic to the protein in soy formulas, so doctors usually recommend hypoallergenic formulas for these infants.
Soy formula is a good alternative to cow’s milk formula for full-term babies (those born at 39 weeks or later). Soy formulas are not recommended for premature babies. Talk to your doctor if you are considering a soy-based formula for your baby.
Do not try to make your own formula at home. Online recipes may look healthy and promise to be nutritionally complete, but they can have too little — or too much — of important nutrients and cause serious health problems for your baby.
Is it OK to Switch to a Different Formula?
It’s probably OK to switch brands of the same kind of formula. For example, parents might buy another brand of cow’s milk formula because it’s on sale or to see if it helps with constipation, or switch to an organic formula because they’re concerned about pesticides.
But before switching formulas, talk to your doctor. Some parents may think that formula plays a part in a baby’s fussiness, gas, spitting up, or constipation. But that’s not usually the case. Your doctor can help find out what may be causing these symptoms and recommend the right formula for your baby.
Do I Need to Give My Formula-Fed Baby Vitamins?
No. Commercial infant formulas with iron have all the nutrients your baby needs. Babies who are drinking less than about 1 quart (1 liter) of formula will need a vitamin D supplement.
Does My Baby Need Fluoride Supplements?
Babies do not need fluoride supplements during the first 6 months. Your doctor may recommend fluoride supplements when your baby is 6 months to 3 years old, but only if fluoride is not in your drinking water.
Is it OK to Prop a Bottle in My Baby’s Mouth?
Never prop your baby’s bottle. Your baby can choke drinking from a propped bottle. Propping a bottle also can lead to ear infections and tooth decay. Always stay with and hold your baby during feedings.
It is OK to Let My Baby Sleep With a Bottle?
Never put your baby to bed with a bottle. Like propping a bottle, sleeping with a bottle can cause choking, ear infections, and tooth decay.
Reviewed by: Mary L. Gavin, MD
Date reviewed: November 2021
Stages of Teething and Helpful Hints – Kids Dental Online
Although the exact timing of can vary from child to child, babies typically begin teething around 6 months of age. Usually the front bottom two teeth (lower central incisors) emerge first, accompanied by the front top two teeth (upper central incisors). Teething can be a painful and difficult process for both babies and parents, as infants may become especially fussy or cranky while their new teeth emerge. Quintessential signs and symptoms of teething include irritability or fussiness, drooling, chewing on firm solid objects, and sore or sensitive gums. Parents also commonly conclude that teething causes diarrhea and fever, but research has shown this to be untrue. Teething does produce signs and symptoms in the gums and mouth but does not generate constitutional or other extended bodily symptoms. In this baby dental topics article we cover stages of teething and helpful hints. Read more about other pediatric dental topics.
Teething happens in 5 stages, lasts a significant amount of time, and can be very tough for both parents and infants to endure. Understanding what to expect during this difficult time, however, can help parents ease the discomfort of their baby as well as navigate their way successfully into toddlerhood.
The 5 stages of teething include:
Stage 1: (0-6 months) At birth, babies have a full set of 20 primary teeth in the jawbones beneath their gums. These are frequently referred to as “milk teeth,” because during this stage a baby’s diet usually consists of milk only.
Stage 2: (6-8 months) During this stage, the first teeth emerge. The lower and upper front teeth, the incisors, begin to erupt around 6 months, but signs and symptoms of pain or discomfort may become evident before 6 months. Prior to eruption, the uneven edges of the teeth may push against the gums, and the baby will typically start chewing on toys, hands, or other solid objects. Putting pressure on the gums alleviates pain and provides a distraction for babies, so make sure to give them appropriate chew items to ease their discomfort. There will likely be an obvious increase in drool during this times period, so keeping a small bib on the baby can make it easier to keep his/her chin dry. This will help keep a rash from forming around the baby’s mouth and chin, which can add to the discomfort.
Stage 3: (10-14 months) During this stage, the primary molars begin erupting. These teeth come in the back of the mouth in the lower and upper jaws. This stage is much like stage 2, but parents will notice an even more evident increase in drool, crankiness, and the need to chew on solid objects. During this time period, it is also common for babies to experience a bit of a loss of appetite, fever, and diarrhea. During stage 3, a baby’s sleep schedule may become more sporadic or get “off.” Unfortunately, it is typical for both babies and parents to lose sleep at night during this period of teething. If a baby’s pain seems to become overly severe or the baby seems to experience inordinate discomfort, consult the pediatrician for advised over-the-counter pain remedies.
Stage 4: (16-22 months) During this stage, the canine teeth (between the top and bottom molars and incisors) will surface. The same recommendations for stage 2 and 3 can be implemented during this period to keep the baby as comfortable as possible.
Stage 5: (25-33 months) For some children, this is the most painful stage of teething. During this time, the large molars emerge. These are the biggest teeth, and parents may find their normal soothing techniques are no longer effective. Try different methods to soothe the toddler until something helps. Many parents find it beneficial to give the toddler a hard vegetable to chew on, and this is also healthy. If implementing this method, make sure to keep a close eye on the child at all times to make sure he/she does not choke!
Helpful Hints For Soothing A Teething Baby
Some helpful hints for soothing a baby’s sensitive and sore gums include:
Massaging a baby’s gums with a clean finger, damp washcloth, or clean dampened gauze pad. Providing this pressure to the gums can alleviate the baby’s pain.
Providing a teething ring made of hard rubber. The liquid filled kind can break as the baby chews.
Filling a bottle with water and allowing the baby to suck. Do not fill a bottle with milk or juice specifically to sooth teething. Extended contact with sugary liquids leads to tooth decay.
Chilling a washcloth or teething ring for a baby to then chew on can also be very soothing. Do not freeze these items, however. Contact with objects that are too cold can cause harm to the gums and teeth.
Giving the baby hard foods that are safe to chew on, if the baby is old enough to eat solid foods as part of his/her diet. Solid vegetables like a peeled and chilled cucumber or carrot can be helpful, but watch the baby closely, as pieces may break off and potentially become choking hazards.
Drying the drool to keep the skin from becoming too irritated or a rash from forming. Keeping a clean dry bib or cloth under the baby’s chin can be helpful.
Giving the baby over-the-counter remedies may alleviate pain as well. Before giving the baby any medicines, however, ask the pediatrician what is safe and appropriate for the child.
Read more on Infant Dental Topics
Why Baby Teeth Are Important
Five Stages of Teething and Helpful Hints
Dental Hygiene for Babies and Toddlers
Baby Bottle (Nursing) Tooth Decay
Thumb Sucking and Pacifiers “Non-nutritive Sucking Habits”
At Kids Dental, we offer comprehensive, family-centered pediatric dental care in a child-friendly nurturing environment. If you are looking for a place to call your dental home, please schedule a consultation with one of our pediatric dentists by completing an Online Appointment Request or calling either office.
Plano Office Phone: 972-378-5437
Carrollton Office Phone: 972-394-2140
Why is my 6 week old drooling a lot? | PopularAsk.net
Researchers believe a baby’s excess drool production is connected to a developing digestive system—so the appearance of drool is likely a sign that your baby’s digestive system is in full development mode. Great!
Read the full answer
Teething often starts when babies are between 6 and 12 months old, though in some cases those first teeth may appear earlier or even a little later. In some very rare cases newborns may be born with a tooth already erupted, or have a tooth come through in the first few weeks.
Beside this, What causes excessive drooling in babies?
According to Morris & Klein in Pre-Feeding Skills, Second Edition, the following possible causes of excess drooling might include: Teething, which results in more saliva production. Poor oral sensory awareness, resulting in decreased triggering of swallowing.
Likewise, What is excessive drooling a sign of?
As if that’s not bothersome enough, drooling can come next. Nervous System Disorders: Disorders like amyotrophic lateral sclerosis (ALS), Bell’s Palsy and Parkinson’s Disease are some examples of conditions that can lead to dysphagia. Stroke: When you have a stroke, blood is not flowing properly to your brain.
Also, Why is my 7 week old drooling so much?
Your baby’s salivary glands have been working since she was in utero, but you may notice that she has started to drool. She’s also putting everything in her mouth and producing more saliva than she can swallow. … The vast majority of babies sprout their first tooth between 4 and 7 months of age.
What does it mean when a baby drools excessively?
Researchers believe a baby’s excess drool production is connected to a developing digestive system—so the appearance of drool is likely a sign that your baby’s digestive system is in full development mode. Great!
Can my baby be teething at 6 weeks?
Teething often starts when babies are between 6 and 12 months old, though in some cases those first teeth may appear earlier or even a little later. In some very rare cases newborns may be born with a tooth already erupted, or have a tooth come through in the first few weeks.
Is it normal for babies to drool a lot at 3 months?
Drooling and blowing bubbles is common in babies during the phase of development when getting what they need is centered on the mouth. This becomes especially apparent at 3 to 6 months of age.
Is my baby teething at 3 months?
Some infants are early teethers — and it usually isn’t anything to worry about! If your little one starts showing signs of teething around 2 or 3 months, they may be just a bit ahead of the norm in the teething department. Or, your 3-month-old may be going through a normal development stage.
How can I soothe my 6 week old teething?
– Rub your baby’s gums. Use a clean finger or wet gauze to rub your baby’s gums. … – Keep it cool. A cold spoon or chilled — not frozen — teething ring can be soothing on a baby’s gums. … – Try an over-the-counter remedy.
What teeth come in at 3 months?
While teething can begin as early as 3 months, most likely you’ll see the first tooth start pushing through your baby’s gum line when your little one is between 4 and 7 months old. The first teeth to appear usually are the two bottom front teeth, also known as the central incisors.
What does it mean when you salivate more than usual?
Constant hypersalivation is usually caused by chronic health conditions that affect muscle control. When you have impaired muscle control, it can affect your ability to swallow, leading to saliva buildup. This can result from: malocclusion.5 days ago
How long does teething last at 3 months?
For most babies though, symptoms of teething can be minor and infrequent. The pain of teething can last for around 8 days, but if multiple teeth come through simultaneously, the pain can continue for longer.
Why is my 8 week old drooling so much?
Eight weeks is a little early for teething, but it’s never too early for drooling! Lot’s of babies drool long and hard before their teeth ever come in, but my daughter got her first teeth at four months so it’s possible your baby is just starting to get ready for teeth.
Is it normal for a 2 month old to drool?
While it’s true that drooling is very common for children around 2-3 months old, and typically lasts until a child reaches 12-15 months-s (roughly the same age that teething begins) drooling merely means your baby’s salivary glands are starting to fire up after not being needed as much when eating easy-to-digest milk.
Why is my 2 month old drooling so much?
While it’s true that drooling is very common for children around 2-3 months old, and typically lasts until a child reaches 12-15 months-s (roughly the same age that teething begins) drooling merely means your baby’s salivary glands are starting to fire up after not being needed as much when eating easy-to-digest milk.
Is excessive drooling a sign of autism?
But it’s common for children with developmental disorders to drool excessively and for longer than is typical with other children. This includes children with autism, many of whom have delays and difficulties with muscle control and sensitivity.
Last Updated: 19 days ago – Co-authors : 8 – Users : 10
How Long Does Teething Last?
You and your baby are both miserable.
How long does teething last, anyway?
Your baby’s first tooth is a moment worth celebrating…and dreading.
Between the drooling, whining, and sleepless nights, you’re probably asking yourself (and every experienced parent in a three-mile radius), “How long does teething last?”
Guiding an infant through their first year of life can be a daunting task. But Kid Care Pediatrics is here to help!
In this article, we’ll answer some of your teething questions, such as “When do babies start teething?” “How long does teething last?” and most importantly, “How can I relieve my baby’s teething symptoms?”
Q: When Do Babies Start Teething?
A: Just like with every other milestone, every baby is different when it comes to teething.
Some babies are born with teeth, others don’t get theirs until they are 12 months old, the rest fall somewhere in the middle.
The most common age for a baby’s first tooth to emerge is about six months, but if s/he still has a gummy smile at their first birthday, there’s probably no cause for concern. The first teeth (or baby teeth) are called milk teeth and the most common ones to erupt first are the central incisors (bottom middle teeth). Remember, every baby is different, so if your baby gets their point teeth first, that’s fine too!
If they reach 18 months and there’s still no sign of any pearly whites, bring it up at your next pediatric appointment.
Q: How Long Does Teething Last?
A: How long your baby is experiencing symptoms of teething can vary, but in general you can expect teething to last for about a week—a few days before the tooth erupts from the gums and a few days afterward. This might not sound like a long time, but it can feel like it, especially if multiple teeth arrive in quick succession.
As for the entire teething process? That takes a lot longer.
Your child will probably have a full set of baby teeth (including premolars) by 3 years of age. As they approach elementary school age, your child will start losing these teeth in roughly the same order that they first emerged.
Q: What Are the Most Common Symptoms of Teething?
A: Some babies will sail through teething with hardly a whimper, while others make their discomfort known to everyone around them.
Common teething symptoms include:
Drooling
Teething causes your baby’s mouth to produce more saliva than usual, leading to a lot (and we mean a lot) of drooling. Some babies may even develop a scary looking (albeit harmless) teething rash on their chin or chest from being so wet all the time.
Excess saliva in the mouth can also cause your baby to cough or even gag. Stock up on plenty of bibs.
Biting & Chewing
New teeth poking through the gums can be irritating and cause sore gums. The easiest way to give the area a nice massage is by biting…on everything in sight. Depending on the position of the tooth, some babies may even pull on their ear or rub their cheek when a new tooth is coming in.
Whining/Fussiness
A teething baby is usually a fussy baby. Although adults don’t remember it, teething can be painful on those sore gums, which can leave your baby feeling fussy and out-of-sorts.
The suction caused by nursing or bottle feeding can make the pain worse, so don’t be surprised if your little one suddenly seems to lose their appetite.
Q: Does Teething Cause a Fever?
A: Sorry, Grandma, but the story about teething causing fever, diarrhea, diaper rash, or a runny nose is an old wives’ tale.
Teething typically starts at roughly the same time as your baby’s immunity begins to wane, so it’s not uncommon for your baby to catch a virus at the same time they are getting a new tooth. But the fact that these symptoms are showing up together is merely a coincidence.
If your baby is experiencing any cold or flu symptoms, bring them into our office (or your local pediatrician).
Q: Which Teething Remedies Work?
A: It’s always hard to see your baby suffering, even if that suffering will one day allow them to eat pizza.
Teething rashes can be treated by keeping their skin dry and applying a small amount of Vaseline (petroleum jelly) to protect the skin. Stick with 100% petroleum jelly with no additives, as this is the safest option for their sensitive skin.
If your baby is chewing on everything in sight, make sure to have plenty of safe teething toys on hand. Nowadays, teethers are made out of nearly every kind of material, but it’s best to avoid hard plastic, as this can be too harsh on their sensitive gums. Silicone and rubber options are best. And remember, since babies are chewing on ‘all the things’ be wary of choking hazards!
To relieve pain and inflammation in the gums, offer them something cold (but not frozen!) to chew on. If your little one loves refrigerated teething rings, make sure they’re filled with nothing but distilled water. If the teething ring is punctured or cracked, you don’t want to worry about toxic materials.
If your child is truly miserable, ask your pediatrician about giving them a small dose of Tylenol or Motrin to relieve their pain (and help them get to sleep). Do NOT use any topical products with benzocaine or homeopathic tablets containing belladonna, as these are highly dangerous for babies.
And those amber teething necklaces? Those are a no-go as well. Not only are they a strangulation hazard, those beads could cause choking if the necklace is broken.
Q: Should I Brush My Baby’s Teeth?
A: Yes! As soon as the first tooth is visible, you can begin brushing after meals and at bedtime.
While your baby will lose these teeth in a few years, brushing now will get them used to having their teeth brushed (and set a precedent for good dental hygiene).
Q: Should I Take My Baby To a Pediatric Dentist?
A: Dentists encourage parents to bring their children 6 months after their teeth start coming in. Usually, the first dentist appointment will happen by 2 years of age.
While s/he might not be eating taffy and lollipops that early, your baby can still get cavities. A good pediatric dentist can spot issues early on and keep an eye on your child’s oral development.
Conclusion
Teething might feel like an eternal process, but we can promise you that it will end. In fact, over the next five years, you’ll go from, “How long does teething last?” to “You lost your first tooth already?!”
Luckily, Kid Care Pediatrics will be there for you at every step along the way. Call us for an appointment and we’ll point you and your baby into the direction of relief.
Why Does My Baby Drool At 3 Months?
I find it funny that when babies hit a milestone in their lives, we adults are quick to mimic them. We clap hands, close and open our fist, and even blow spit bubbles to amuse them–and us. When infants reach three months of age, it’s not unusual to find some people blowing a raspberry at them. Or is it just me? Amusement aside, it is at this age where bibs and extra cloth wipes are indispensable in your baby essentials. Why? Because of drools.
Excessive drooling is one thing that comes naturally to babies. Sometimes, it can happen as early as two months until they are two years of age. The drool production signifies that your baby’s salivary gland is activated, and his digestive system is working great. Hence, we always associate saliva with good digestion. But since babies have not fully developed their muscles, it’s difficult for them to swallow it back. When a baby is teething, he may also drool more than usual.
What causes excessive drooling?
The abundance of saliva or salivary reflex is a good indicator of an infant’s full gear digestive system. According to the American Academy of Pediatrics, saliva serves some important functions for babies. For once, it helps babies to swallow food easily and keeps solids moist and soft. It even neutralizes stomach acid that aids in proper digestion. It also keeps his mouth moistened and protects his teeth in the process.
But why is there too much saliva, you may ask? When should you worry that your baby’s drooling needs medical attention? Here are the common causes of why babies are wetting their bibs so often.
Developmental cause
Babies have a limited ability to swallow. Along with normal hypersecretion, it results in dribbling out their mouths. Add it to the fact that they lack the front teeth to hold it back like a dam. Also, babies’ mouths are adapted to the opening position. Hence, they cannot quite keep their lips pursed together just yet.
When the baby reaches two years of age, the muscle around his mouth becomes fully developed. During this time, he will gain full control of his swallowing reflex. His front teeth are also established. With mature oral motor function, drooling will disappear in babies.
Physiological cause
It is normal for us to relate drooling with teething. In fact, this is the first thing that we likely associate when we see babies dripping with saliva. While it is indeed a common cause, it is only secondary to developmental reasons.
The baby’s mouth gets stimulated to produce more saliva when he is teething. It helps him soothe his tender gums as his body’s stimuli anticipate the pain. When he starts drooling a lot and exhibits other teething signs, expect an eruption of a new tooth.
Oral conditions
Infants and toddlers may, at times, contract mouth conditions like thrush or cold sores. This will make them secrete more saliva. Thrush is a fungal infection prevalent among infants and is characterized by white patches in the mouth. Oral thrush often comes with diaper rash and gastrointestinal problems.
Lesions in the mouth due to cold sores may also cause babies to drool excessively. Although mouth sores are not common in babies, they can likely occur. When this happens, expect babies to get extra cranky and develop a swallowing difficulty.
Neurological problems
Children usually stop drooling when they reach four years of age. To some parents, excessive drooling beyond infancy can get stigmatizing. When it happens in older children, it is sometimes due to neurological problems relating to low muscle tone.
Involuntary drooling is common in children with autism, cerebral palsy, and facial nerve palsy. So, when your three-year-old kid is still dripping saliva, it is best to consult your pediatrician. Usually, this comes with other symptoms like motor, speech, and language delay.
The good things about drooling
The human body produces around 2 to 4 pints of saliva every day, even more so in babies. Drooling in babies happens for a very good reason.
We know how soggy clothing, blanket, and bibs can get annoying. Drooling is simply messy. However, it is pretty natural, and all babies undergo this wet stage. Some kids even dribble spits more than the others. But did you know that saliva hypersecretion also has benefits for babies?
Here are some slippery saliva facts that will make you love your drooling little one:
Drooling indicates baby’s growing sense of smell
Food makes our mouth water – some with the sight of it, others with the aroma. Salivation to food cues is no different with your developing baby. When you prompt him with food, and he increases drooling, it means he has established his sense of smell. It’s the brain that sends this reaction to help his body prepare for digestion.
Saliva aids in digestion
Well, it is a long-known fact – drools contain enzymes that assist in food digestion. So, when he is at the age when he is ready for solids, his salivary gland automatically fires up. Saliva is responsible for moistening the food and binds it together for easy swallowing. It also assists the digestive system to process food smoothly, even without the baby’s chewing it.
Drool protects the gut
Recent research show how neonatal saliva and a mother’s breastmilk interaction can boost babies’ immunity. It is through a study conducted by Dr. Emma Sweeney et al., from the University of Queensland. They observed that a mixture of breastmilk and saliva inhibits the growth of microorganisms.
Imagine the disease-causing germs that lurk in your little one’s toys and stuff. So it is good to know that your baby is naturally protected. And it pays to continue breastfeeding and make the most out of its tons of benefits.
Saliva cleanses the mouth
Food debris in the mouth can cause oral health problems, even for babies. Drool plays an important function in cleaning the baby’s mouth out of it. The slight alkalinity of saliva also protects the new teeth against cavities and other gum problems. Aside from keeping the mouth’s pH balance, its enzymes also combat the harmful bacteria in the mouth.
In teething babies, excessive saliva secretion also helps soothe their tender gums. But do not expect your three-month old’s teeth to pop out soon. Babies would usually grow their first tooth at around six months of age.
Saliva protects the teeth
Early tooth decay is inevitable. Once your baby starts eating solid foods, the possibility spikes up. Sugary and acidic foods may take up some part of his diet. But the saliva’s alkalinity helps buffer the acid. It prevents demineralization of the enamel once his teeth come out.
It is important to note that saliva does not kill the bacteria in the mouth. It simply prevents it from building up in the gums and teeth. Yes, drooling is all good for your baby’s growing teeth. But don’t forget to encourage good oral hygiene and start him on a healthy diet early on.
The nasty side of drool – rashes
You are okay with a few clothing changes for your baby throughout the day. But what worries moms most is the presence of rashes that comes along with the frequent wetness. The excess moisture oftentimes led to redness around the baby’s mouth or skin that comes in contact with it.
There is nothing you can do about it other than ensuring that his mouth remains dry to ward off the irritation. Use a soft cloth and gently dab (never rub) it on the wet surface. The bib is your handy helper during this phase in your baby’s life.
Since drooling never stops even when the baby sleeps, applying ointment may help. Your pediatrician can help you out with the right product.
FAQs
When should I worry about drooling?
If your baby has a steady and unusual stream of drool, have your baby checked. If he has trouble breathing and turning blue along with it, take him to the emergency room. These signs may indicate choking.
My child has no special needs, but still dribbles occasionally. What should I do?
Your child may have a problem with swallowing because of poor coordination. Sometimes, doctors recommend using an oral appliance to help him out with this and decrease the drooling.
It’s a device that manages tongue positioning and proper lip closure. If he has a weak jaw, therapy might help resolve the issue.
Will medication cause drooling?
Yes, drooling is sometimes a side effect of certain medications that the baby takes. Even drugs that the breastfeeding mother is taking can also cause hypersalivation in breastfed babies. This may include medicine for seizures and sleep-inducing and pain-relief pills.
Takeaway
Drooling is a part of your baby’s developmental milestone, although some parents are unaware of it. They would mostly relate it to teething signs. While this is true, teething is not always the root cause of a baby’s excessive drooling, especially not on a 3-month-old. It is so much more than just his growing teeth.
Eventually, they will outgrow this stage when their oral motor is in full function. If your older kid has uncontrolled drooling after the age of four, then it is best to consult your physician.
Why do drooling blisters in a 2 month old baby? How to survive this period?
If a two-month-old baby suddenly drools, then many parents diligently begin to look for swollen gums or teeth that have already crawled out in his mouth.
But the first teeth in children very, very rarely appear in the third month of life. So why then does the baby drool so much and blow bubbles?
Why does a 2 month old baby drool?
1. Beginning of the functioning of the salivary glands.
This is the most common reason. In the third month, the active work of the salivary glands occurs, a large volume of saliva begins to be produced. And the swallowing reflex is fully formed only by 5 months, so the baby simply cannot swallow so much saliva. It is for this reason that saliva flows out.
2. We are waiting for the first tooth.
Although the first teeth appear after four to six months, the gums can already start preparing for this event. The teeth gradually begin to move in the gum, preparing to come out in a few months. The body begins to produce an increased amount of saliva to moisten the irritated gums. As soon as the first tooth cuts a hole in the gum, the amount of saliva will decrease.
3. Saliva protects the little organism.
It turns out that the baby’s saliva contains special antibacterial substances . They help to neutralize infections that enter the mouth. This is an extremely useful and necessary property of saliva. Starting from 2 months, a small child begins to put everything in his mouth.
It can be a rattle, your own hands or your mother’s finger. It is abundant saliva that prevents infections and bacteria from entering the baby’s body. Salivary fluid washes the mouth and flows out along with possible bacteria.
4. Allergic reaction.
Approximately 15% of babies are predisposed to such a disease as allergic rhinitis. Signs of this disease, in addition to profuse salivation, are also swelling of the mucous membrane, watery eyes, sneezing, itching in the nose. The cause of such rhinitis can be dust, flowering plants, pet hair.
Doctors’ advice on what to do if a child has low hemoglobin at 3 months.
Read here about how a baby develops at 7 months. Norms of weight and height.
In this article, read about the baby’s daily routine at 9 months, about his nutrition, development, feeding.
If you observe all these symptoms in an infant, you should consult a doctor and get advice and appropriate treatment from him.
5. Diseases of the oral cavity.
Sometimes excessive drooling can indicate oral diseases such as thrush or stomatitis.
In addition to increased salivation in these diseases, the child is restless, capricious, will suck badly and white plaque or plaques can be found on the mucous membranes.
If you experience these symptoms, you should immediately contact your pediatrician and seek treatment advice.
6. Hypersalivation.
Very rare, but profuse salivation may be one of the signs of serious illness .
In order not to miss the disease, you should carefully monitor the health of the baby, take all the necessary tests and studies according to age.
A consultation with a neurologist and a pediatrician will clarify the picture and relieve parents of unnecessary suspicions.
How to survive such profuse salivation?
From the beginning of the third month of life, abundant saliva occurs in almost all babies.
And if at first they do not cause any discomfort, then over time, constant drooling wets clothes and can cause inflammation around the mouth and on the chin.
Here are 5 tips that you can and should use during your baby’s salivary period.
Change wet clothes more often. And let it add washing to mom, but the baby will always have a comfortable dry breast and neck.
Purchase and use a large number of bibs and change them as needed. In stores, you can now find colorful bibs of various colors and textures.
Wipe baby’s face with sterile gauze or a clean soft handkerchief. In this case, do not rub the already damaged skin of the child. If, nevertheless, irritation appears on the skin, then cracks and pimples should be lubricated with baby cream or sea buckthorn oil.
If increased salivation is associated with the eruption of the first teeth, then it is necessary to acquire special teethers or teethers. Various teething gels have proven themselves very well in this case, they significantly reduce pain and cool the gums.
Be patient and get used to your baby’s constant saliva. After all, children’s drooling is a continuous phenomenon. After six months, active teething will begin and drooling, flowing in a stream, will not disappear anywhere.
Conclusion: Increased salivation for babies under one year old is an absolute physiological norm. If parents are very concerned about this problem, then you can consult a pediatrician about this.
Over time, the drool that flows like a river from your baby’s chin will certainly decrease, and then completely disappear. And you will remember with nostalgia this “dribbling period” in the life of your child.
Share with your friends
Does baby drool at 2 months? Here’s what you need to know!
Your precious child is growing so fast – it seems that he will change in the blink of an eye! Despite all these changes, some of them may bother you, especially if you are a first-time parent. For example, does your baby drool at two months? In this article, we’ll tell you everything you need to know about your drooling two-month-old!
Contents
What to know when your baby starts salivating at two months
Why does this happen?
Your baby is healthy
This is not a sign of teething
What should I do if saliva causes irritation?
10 Facts About Baby Saliva
1. Humans produce 2 to 4 liters of saliva every day
2. Salivation begins between 2 and 6 months of age
3. Infants cannot swallow as well as adults
4. Drooling comes with milestones
5. Drooling can mean your baby is teething
6. Your baby might get a rash
7. Use a bib to fight baby saliva
8. Drooling continues for about two years
9. Salivation should be
10. Can drooling be a sign that something is wrong?
What to know when your baby starts salivating at two months
It’s OK!
Baby salivates at two or three months.
Why is this happening?
Infants cannot fully control the muscles that control swallowing until 18-24 months of age. In addition, the average person produces two to four liters of saliva a day!
Not being able to swallow saliva, expect your child to salivate for a long time!
Is your baby healthy?
Is your baby drooling at two months? Drooling is actually a positive indicator that your baby’s digestive system is developing well.
In particular, saliva helps break down food before it reaches the stomach. In addition, saliva destroys bacteria and washes the mouth, preventing the child from getting sick.
Therefore, if your child is salivating excessively, it means that his digestive system is working properly!
This is not a sign of teething
Many people think that salivation is a sign of teething. However, there is no direct correlation between them. In fact, these two events occur at the same time.
When your child begins to develop fine motor skills such as chewing, receptors send signals to the brain that trigger saliva production. So when your baby is ready to start eating solid food, he will start to drool more!
So salivation is not a direct sign of teething. However, it will probably happen around the same time.
What if saliva causes irritation?
In some cases, saliva can cause irritation around the mouth, such as a rash or dry skin.
If this happens to your child, try to gently wipe off the saliva so that it does not remain on the child’s face for too long. Alternatively, you may consider applying an ointment to the affected area at night.
After all, there is nothing you can do to prevent your child from salivating. This is a natural and healthy part of a child’s development!
10 Facts About Baby Saliva
When you have a baby, you probably have to do a lot of cleaning. Babies burp, blow out diapers, and drool. Blowing soap bubbles is adorable, but you might be worried if your little one is constantly soaking his shirt with saliva. How much is too much, and should you be concerned about excessive salivation?
1. Humans produce 2 to 4 liters of saliva every day
The human body produces 2 to 4 liters of saliva every day. Saliva is needed to keep your baby’s mouth moist. It aids in swallowing and removes leftover breast milk, formula, or food. Saliva helps keep your mouth healthy.
2. Salivation begins between 2 and 6 months of age
Newborns do not produce much saliva. Their digestive system does not need much help from saliva enzymes until they are ready to eat solid food. The body begins to prepare them for this at the age of 2 to 6 months. It is recommended that parents begin offering solid foods to infants at six months of age.
3. Infants cannot swallow as well as adults
Infants do not have the muscle development and coordination necessary to swallow all of their saliva. When their bodies start producing more, they don’t know how to deal with it. There seems to be more saliva coming out of their mouth than inside.
4. Salivation comes with milestones
You may notice that your baby is drooling more around the same time he has mastered other milestones, such as putting his hands in his mouth. Saliva becomes a new sensory experience to explore and play with. Babies will use their hands to feel drool and to explore the sensation on their lips.
5. Drooling may mean your baby is teething.
You may notice saliva coming out of your baby’s mouth when teething. The sensations that occur during teething stimulate salivation. However, just because your 3-month-old is drooling doesn’t mean you’ll soon see a tooth pop out. The first tooth usually appears around 6 months of age.
6. Your child may develop a rash
Constant moisture in your child’s face can cause skin irritation. Sometimes children who have excessive salivation develop red, raw skin or bumps under the lower lip and on the chin. Saliva can even collect in the folds of the neck and cause a rash.
7. Use a saliva bib
Keep your baby’s skin as dry as possible. The bib can act as a barrier between moisture and the neck and chest. Covering the skin with a moisturizing ointment can also prevent irritation. Wiping your baby’s chin and neck can also help prevent a rash. Just pat your skin gently to avoid aggravating it.
8. Salivation lasts about two years
Children drool until they are two years old. This is fine. By nine months, babies may not drool as much as they do gross motor activities such as crawling or walking. But they can still have episodes of profuse salivation when they erupt, eat, or play. Salivation usually slows down by about two years of age.
9. Salivation should be
Your child may appear to be drooling a lot. Regular salivation is normal. If your child has a constant stream of saliva that comes out of his mouth, you might want to check it out.
Some children have problems with their tonsils or adenoids, which may contribute to salivation. A pediatrician or physical therapist can help you determine if there are problems that are causing your child to drool more than usual. Weak jaw muscles or an inability to close the mouth at rest can increase salivation, but these problems can be corrected with therapy.
10. Can drooling be a sign that something is wrong?
Although salivation is normal for babies and toddlers, sudden salivation can be a sign that something is wrong. If your child has trouble breathing, turns blue or chokes while salivating, he may choke. Sometimes a sore throat causes a child to drool. If you ever worry about your child drooling, don’t hesitate to contact your pediatrician.
Increased salivation in a two-year-old child – nipple or other causes
Very often there is a situation when an infant, after two months of life, begins to bleed and drool. The mouth is often wet. Worried moms and dads immediately start looking for information on acquaintances and forums, consult with experts, get nervous and worry if their baby is sick. A worried family is looking for reasons in possible violations of the internal organs. Calm down dear moms and dads. This is no reason to panic.
A child drools at 1 month
The birth of a child is not only a long-awaited event, but sometimes a test for a young and inexperienced mother. The baby is prone to various diseases, since the immune system is not yet sufficiently formed. Alarm signals cannot be ignored. Drooling in such young children, who are not yet three months old, is not uncommon, but increased salivation can be a symptom of certain health problems. In general, salivation at this age is normal, but too strong, of course, indicates the appearance of some irritating factors in the external environment. After all, they don’t just appear, such is the physiology of the baby. Pediatricians say that this is how a protective reaction of a small organism manifests itself.
Drooling occurs in infants at 1 month, but especially plentiful discharge begins at 2-3 months. The child develops gradually, the body is formed in several stages. So, just a few months after birth, a small person begins to explore everything in the most accessible ways for him.
So far, he can cognize the surrounding world only through certain sense organs, the set of methods is limited, all objects must be tasted. Therefore, babies even pull their own legs into their mouths, not to mention all the objects found on the floor. They can be not only toys that parents treat in a special way, but also household utensils, etc.
It is not always possible to keep track of a lively toddler, so the body must be protected. This function is performed by saliva. Bacteria of various viruses can be found on all these numerous objects, and the protective functions of the child are not yet sufficiently formed. Therefore, a lot of saliva in the baby, maybe for a very understandable reason. This is a protective agent, because they have
Just yesterday your baby was a cute baby, and today he suddenly started blowing bubbles. What happened, why are you salivating so much that you don’t have time to wipe it off? What to do: call a doctor or is it not dangerous, and they will go away on their own?
With the birth of a child, a mother has new questions every day. There were no tears before when I cried. Then you need to wipe your mouth, clean your ears, but it’s scary to hurt. Now, suddenly, saliva flowed, and for some reason so much … There are many questions, let’s consult a pediatrician.
Your newborn is growing, getting bigger, reaching two to three months of age. At this stage of development, the salivary glands are formed and begin to work. Therefore, the appearance of profuse salivation is a normal phenomenon.
During this period, the baby becomes more active. The child explores and tastes everything that surrounds him. Therefore, the body produces a protective antibacterial environment ─ saliva, which washes away the dirt that enters the small mouth.
The newborn’s saliva has already appeared, but the baby still does not know how to swallow it, so streams flow down the chin. Parents are afraid of such profuse salivation. If the saliva is transparent, not foamy, not thick, not viscous, experienced mothers do not worry. Mothers know that this is the normal state of the baby at this age.
Abundant salivation in infants 2-3 months old is a common thing, because it is during this period that their salivary glands “turn on”
Saliva and its functions
Saliva is necessary for the body at any age. In the oral cavity under the tongue, on the inside of the cheeks, behind the lower teeth are the salivary glands. They work constantly, producing up to two liters of fluid per day in an adult.
Saliva takes care of maintaining the pH in the right state, prevents the formation of tartar and caries. By means of saliva destroy
Saliva in babies
Saliva in babies is always secreted – this is a normal physiological process. It causes concern if the child’s oral cavity is dry. In this case, periods of strong salivation usually last no more than a month.
Saliva itself plays a vital role in the interaction between man and the environment . Firstly, it is involved in the process of digestion – it contains the enzymes necessary at its initial stage. Thus, we can say that from the moment the food entered the mouth, it began to be digested. In addition, salivation begins reflexively at a time when a person experiences a feeling of hunger.
Secondly, saliva performs a protective function for the body, it is a kind of antiseptic that prevents bacteria from penetrating through the oral cavity.
Why is there so much saliva
Your newborn is growing, getting big, reaching two or three months of age. At this stage of development, the salivary glands are formed and begin to work. Therefore, the appearance of profuse salivation is a normal phenomenon.
The newborn’s saliva has already appeared, but the baby still does not know how to swallow it, so streams flow down the chin. Parents are afraid of such profuse salivation. If the saliva is transparent, not foamy, not thick, not viscous, experienced mothers do not worry. Mothers know that this is the normal state of the baby at this age.
Abundant salivation in infants 2-3 months old is a common thing, because it is during this period that their salivary glands “turn on”
Abundant salivation in children of two years of age and older
case, you should go to the hospital. Only specialists can answer the question of why this happens in a child at this age. They will determine whether drug therapy is needed in this case or whether this moment can be waited out.
When getting rid of these manifestations, it is necessary to compare the methods of treatment with the pathology itself. However, you can’t do nothing. Children with this problem can get a speech disorder
, because a large amount of clear liquid prevents them from pronouncing words well. Subsequently, this can lead to delayed development and sociopathy.
By the age of 2, children can usually swallow. If a child is drooling at 2 years old, and if it is not teething, a speech therapist should be consulted.
At this age, molars may erupt in children. This can cause hypersalivation. As in the case of infants, the problem may arise due to ENT – diseases, diseases of the digestive system, stomatitis, gingivitis, allergies. If the problem manifests itself mainly at night, then the baby may have a helminthic invasion
.
Saliva and its functions
Saliva is essential for the body at any age. In the oral cavity under the tongue, on the inside of the cheeks, behind the lower teeth are the salivary glands. They work constantly, producing up to two liters of fluid per day in an adult.
Saliva maintains the pH in the right state, prevents the formation of tartar and caries. Through saliva, harmful microorganisms are destroyed, thereby preventing an unpleasant odor in the mouth.
Saliva is involved in the processing and digestion of food. Salivary enzymes contribute to the breakdown and digestion of substances, the production of glucose from starch.
The main causes of excessive salivation
1. Teeth are coming soon!
The main cause of increased salivation in babies is preparing the gums for teething. This period can start from 2 months and continue during the first year and a half of the baby’s life. The teeth can move even in the gum itself and cause pain to the baby. And saliva softens inflamed gums and has an anti-inflammatory effect, as nature itself intended.
In this case, you are unlikely to cope with salivation, but you can help the teeth to be born by buying baby teething toys and special teethers, for example, filled with water. They can be cooled in the refrigerator and given to scratch the gums of the child. Pain will be much less intense.
2. Intensive work of the salivary glands.
The salivary glands are not yet fully formed, and during the first year of life they may “test” their work from time to time. There is too much saliva, the baby is not able to swallow it all, and it flows out. Fortunately, such periods are short-lived and are quite rare, but nevertheless they take place.
3. Bacteria control.
From the age of three months, the baby puts rattles in his mouth. And the older you get, the more you want to try “by the tooth”. Any dirty object can cause an unpleasant disease in a child – stomatitis. The body wants to get rid of the causative agent of infection by all means, and since saliva has bactericidal properties, the oral cavity is literally washed by saliva from microbes. Hence the complaints of parents about increased salivation in babies.
4. Hypersalivation.
I would like you to never encounter this term in everyday life. In this case, increased salivation may be a sign of a more serious condition. Parents should monitor every change in the behavior and health of the child. It is necessary to consult with a specialist to rule out brain diseases, unequal systems, and the presence of tumors.
Hypersalivation is one of the signs of the disease, usually the primary one, because it is quite difficult to determine the discoordination of movements in infancy, because the baby is still just learning everything. The neurologist and pediatrician will see the picture more clearly, so do not jump to conclusions, but be on the lookout.
The fact that the baby is drooling in most cases indicates teething. It is useless to fight this, you cannot influence this process. But it is quite possible for you to make life more comfortable for yourself and your child:
so that clothes do not become saturated with saliva, put on special collars with a waterproof lining for your child;
when outside, try to give your baby a pacifier, it will help the baby swallow saliva;
baby’s gums are itchy, so you can massage them with a clean forefinger, applying gentle pressure to the expected teething areas;
gel for gums will cool the inflamed areas, relieve redness and in a couple of seconds the child will be calm and not hurt.
Remember that excessive salivation in a child is a temporary phenomenon, with the eruption of the first main teeth, the child will be much easier and saliva will no longer be released in such a large amount. Wait out this period, and to avoid making false diagnoses, contact a specialist – your local pediatrician. Easy teething to you, be healthy!
Teething
This is the most likely cause of excessive salivation in infants. The gums of a baby during teething become very inflamed, itchy and sore, causing severe discomfort to the child. And saliva, due to its anti-inflammatory properties, has a calming effect on the gums, dulling the pain and, as a result, improving the overall well-being of the baby. In some children, the preparation of the gums for the appearance of teeth begins as early as the second month of life. Therefore, there is no need to be afraid if
The child’s salivary glands have not yet been adjusted. It happens that the baby produces more saliva than he is able to swallow, and then it flows out of his mouth. This is due to the fact that the salivary glands in babies under the age of one year are still being formed. You should not worry about this, the baby is growing and soon the work of the salivary glands will be established, and the profuse salivation will stop.
Fighting bacteria
Stomatitis in babies is quite common. After all, kids pull into their mouths all the objects that fall into their hands – both during teething, when the gums itch, and just out of curiosity – for a child this is one of the ways to learn about the world around them. Therefore, it is very important to keep the toys of the crumbs clean and make sure that he does not pull dirty objects into his mouth (which can result in stomatitis).
If the parents suspect that their child has some serious illness, then you should immediately consult a doctor. Indeed, in rare cases, saliva begins to be abundantly secreted in such serious diseases as a disorder of the nervous system and a brain tumor.
When a child develops excessive salivation, the causes are usually as follows:
During teething, inflammation of the gums occurs, due to the production of a large amount of saliva, the gums are washed, and the infection is eliminated. This helps prevent the development of gingivitis or stomatitis. Most often, as soon as the top of the crown of the tooth appears above the surface, salivation stops. This is the most likely explanation for why a three month old baby is drooling.
Active salivation may indicate the presence of some abnormalities in the health of the baby. Salivation can be caused by a viral infection or allergic inflammation with the development of a runny nose. In this case, nasal congestion, fever, deterioration in the general condition of the child will be noted. In this case, it is best to immediately contact a specialist for medical assistance. Such an explanation may give an answer to the question of why a 2-month-old baby is drooling.
Drooling can be caused by thrush in infants. Therefore, to exclude it, the oral cavity should be examined, and in the presence of a whitish plaque and ulceration, measures should be taken.
Excretion of a large amount of saliva, especially if it occurs at night, occurs with helminthic invasion. Therefore, there is increased salivation in the child.
If your baby is constantly salivating and his stomach hurts, and digestion is disturbed, then in this case, you should consult a doctor to rule out intestinal pathology. This is also one of the common reasons why babies drool blistering at 2 months or younger.
In all newborns, the secretory activity of the salivary glands is quite low. In general, saliva is slightly secreted and has a viscous consistency.
One month old baby is not prone to blowing big bubbles. If suddenly this happens, it rather indicates the immaturity of the system responsible for the regulation of salivation. This becomes the norm by the age of one and a half months, simultaneously with the increasing activity of the salivary glands. If the baby has profuse salivation and there is no other evidence that teeth are really climbing, the possibility of allergic rhinitis, infections of a bactericidal or viral nature, as well as birth defects cannot be ruled out. Then you need to consult a pediatrician.
At 2 months, your baby’s copious saliva should be patiently wiped regularly with a soft cloth so that clothes wet from saliva do not provoke rashes, irritations on the body. You can use a bib, it has a polyethylene back side that will protect clothes from getting wet. If, nevertheless, she gets wet, of course, you need to change the child’s clothes. In case of irritation, use baby cream or petroleum jelly: gently lubricate the chin and lip contour. It is very important that the baby cannot lick off the ointment.
By the 3rd month of a child’s life, the salivary glands begin to function actively in parallel with the endocrine glands. However, the process of swallowing the child can only be carried out during feeding; in another state, he still does not know how to swallow saliva. So, if a baby at 3 months plentifully lets them in, you should not worry: he will soon learn to “communicate” with saliva.
But as for teething, this process, most often, begins by six months. Although there are exceptions, up to the point that a child can be born already with teeth (but this is extremely rare).
important A wake-up call for parents should be a birth defect that interferes with the child’s swallowing of saliva and leads to its accumulation.
This pathology can be seen up to two years, so you should see a doctor as soon as possible. But there are other dangerous signals that should not be ignored.
In medical practice, there are certain provoking factors for the development of hypersalivation in children of different ages.
Name
Description and age
Additional symptoms
Teething
Natural physiological process between the ages of six months and 4 years. Gradual increase in saliva production. It is characterized by constant secretion of transparent liquid saliva from the oral cavity.
Whole body hyperthermia, increased tearfulness, nervousness, sleep disturbance, constant restlessness and rapid fatigue. The gums are inflamed and red, itchy and sore.
Diseases of the oral cavity
Pathological condition associated with the development of inflammation in the oral cavity at any age in children. The most common diseases include stomatitis and gingivitis. Accompanied by a large secretion of saliva with white opaque inclusions. There may also be blood in the saliva.
With stomatitis, ulcers are observed on the oral mucosa, which, at an advanced stage, can bleed. Also, the surface of the tongue is covered with a whitish coating and a strong pain syndrome appears. With gingivitis, inflammatory processes in the gum tissue are observed, accompanied by local hyperthermia, swelling and discoloration.
Gastrointestinal diseases
Can develop in a child at any age. The most commonly diagnosed pathologies in this case include: pancreatitis, peptic ulcer, enteritis, hepatitis, gastritis.
Large salivation is accompanied by the following symptoms: diarrhea, nausea, bouts of vomiting, pain in the abdominal cavity, heartburn, constipation.
Diseases of the nervous system
Abnormal development of the brain and its congenital injuries. Separate forms of cerebral palsy. Also with systematic severe stress or high psycho-emotional overexcitation. These conditions can develop at any age. Therefore, salivation increases regardless of the age category.
Increased nervousness and tearfulness of the child. Inconsistency of development with the age period of the baby and his lack of correct reactions to a certain stimulus.
Fungal infections
Damage to the oral mucosa by pathogenic microorganisms and its inflammation is accompanied by increased hypersalivation. In the secreted saliva, the presence of white flakes is most often noted, which are formed during candidiasis and other fungal infections. The risk group includes children of any age category.
The presence of white coating on the surface of the tongue, lack of appetite, pain when swallowing and chewing food. Persistent or intermittent burning and itching sensation in the mouth.
Poisoning
Intoxication of the body with toxic substances, strong drugs, heavy metals and concentrated chemicals. Age category of children from 2 years and older.
Vomiting, dizziness, respiratory rhythm disturbance, fainting, diarrhea, watery eyes, dermatological rashes. Formation of ulcers, with a chemical burn.
Inability to swallow saliva
This pathological process manifests itself in children aged 1 to 4 years. The swallowing reflex is not developed in children with allergies, because due to allergic rhinitis, the child uses the mouth for breathing. Therefore, saliva flows out on its own.
Hypersalivation of this etiology develops in children of any age. Increased secretion of saliva (a lot of saliva) is noted when eating certain foods that are allergens. It can also be skin contact or inhalation of allergens.
Runny nose, rash in the area of the nasolabial fold, fever, watery eyes, itching and burning. Increased moodiness and tearfulness.
Worm infestations
Excessive secretion of saliva can be caused by the presence of various types of parasites in the child’s body. A special risk group includes children of any age who are in contact with animals, open ground and frequent games in dirty sandboxes. It is also dangerous to eat unwashed vegetables and fruits.
Saliva becomes cloudy. Increased anxiety of the child, a sharp loss of appetite and body weight, itching in the anal area, nausea, vomiting.
Side effects of drugs
Hypersalivation acts as a side effect when undergoing a therapeutic course with the use of medications.
Additional symptoms may be various signs corresponding to the side effects of each group of drugs.
Injuries, etc.
Often one of the consequences of a fall is inflammation of the salivary glands, which provokes increased secretion of saliva. Most often, this cause of hypersalivation is observed in children older than 6 years.
Injuries and inflammation of the skin at the site of the herb. Pain on palpation.
How to help the baby
Help families who are in trouble
Parents will have to come to terms and survive the period of drooling of the little one. It is unpleasant for the baby to be slobbery himself, so parents especially diligently take care and care for the baby at this time.
Not in vain, apparently, even our great-grandmothers invented bibs for babies. Bibs will help even now: the fabric absorbs liquid, blouses remain dry, the skin on the neck and breast is also dry.
Sometimes a baby in the supine position lets out so much saliva that he chokes and simply chokes on it. He may cough, even wheeze. So that the child does not have trouble, put him on his side or on his tummy, you can put him on a low pillow. So, saliva will flow down and will not harm the baby.
Soon the teething time comes, the crumbs itch, the gums itch, he constantly gnaws something to relieve the itch. Help him, massage his gums with your finger. And in places where the first teeth appear, gently press. On the recommendation of a doctor, buy a special tool that lightly lubricates the gums with it, this will calm the baby.
A pacifier can help minimize the problem of salivation. If a baby sucks on a pacifier, he will swallow saliva
What to do for parents
As a rule, even excessive salivation does not need to be treated. But to provide proper hygienic care when the baby is drooling is necessary in order to prevent irritation of the baby’s delicate skin. Followed by:
Remove saliva from the baby’s chin in a timely manner by blotting with a clean cloth.
Protect the child’s clothing with bibs, scarves.
Be sure to treat the area where irritation has occurred. To do this, it is enough to rinse the inflammation with warm water, blot with a diaper and apply a little baby powder. You can also use baby cream.
In the cold season, do not let the baby’s skin and clothes get wet.
A pacifier can be offered to help babies feel better when their gums itch. If parents are opposed to this method, you can give the baby a chilled teether, which can be purchased at a pharmacy.
To prevent the baby from choking on saliva during sleep, try to control that his head is turned to one side, and do not forget to raise the top edge of the mattress by 30-40 degrees.
Place a folded diaper under the baby’s head during sleep, if it gets wet from saliva, it can be easily replaced with a dry one.
Skin irritation is a source of discomfort. Parents should not forget about this, treat the whims of the crumbs with understanding and patience.
A little tip: gauze folded in several layers perfectly absorbs saliva, it is quite soft, does not irritate children’s skin and is affordable.
If you are afraid of the abundance of saliva
Usually, a 2-3 month old baby begins to profuse saliva secretion during the entry into the work of the salivary glands. The second stage, decorating the little one with bubbles, is the period of teething.
During colds and other diseases of the ENT organs, with allergic reactions to house dust or animals, when the nose does not breathe, the baby has to open his mouth. In such cases, the amount of saliva that can drain from the mouth increases. See a doctor, eliminate the cause, and the amount of saliva returns to normal.
The most common cause of excessive saliva is teething. And also if the baby does not know how to tightly close his mouth. It must be said that with the defeat of such a disease of the oral cavity as thrush, saliva partially loses its functions. In particular, the digestion of starch into glucose stops. The absence or insufficiency of sugars in the body of infants will adversely affect their development. Therefore, with daily morning toilet, look into the baby’s mouth, in case of any suspicion, contact the pediatrician.
But if there is too much saliva, it is of a different color, type or consistency, if you are afraid of the abundance of discharge, be sure to consult a pediatrician. If necessary, after a thorough examination and analysis, the pediatrician will refer you to another specialist. An ENT, a neuropathologist, a dentist, a surgeon can help.
The doctor will make a correct diagnosis based on the analysis of saliva. If the crumbs have problems of an endocrine nature or in the adrenal cortex, saliva analysis will show the disease. To obtain accurate data, saliva is taken for analysis several times during the day. It is not difficult, painless, will show the right result.
If the baby is healthy, the drooling period will soon stop, the baby’s mouth and chin will be dry.
When to See a Doctor
It’s not always safe when a baby is drooling and blistering at 2 months. Often, the appearance of such a symptom can mean the appearance of a serious illness.
Temperature 37.4 in a 4-month-old child
If the following symptoms are detected, you should immediately consult a doctor:
Inflamed oral mucosa. If sores, wounds and erosion are visible on the tongue, then qualified treatment should be started immediately.
The gums become inflamed during teething.
Worm infestations. Helminths release toxic substances and products of their vital activity into the body, as a result of which saliva secretion increases.
Inflammatory processes of ENT organs: otitis media, sinusitis.
Poisoning by toxic substances: mercury, lead, chemical pesticides.
Traumatic injuries increase the secretion of the salivary glands and disrupt their activity.
Infectious diseases. In this case, hypersalivation is of an auxiliary nature, so the body gets rid of pathogenic microorganisms. Often, the temperature also rises, a runny nose, cough, redness in the throat appear.
Conjunctivitis.
Streptococcal tonsillitis.
Epiglottitis – swelling of the epiglottis. It is imperative to call an ambulance.
Convulsions.
In case of hypersalivation anticholinergic drugs are prescribed:
Atropine;
Spasmolytin;
Tifen;
Diprofen.
Important! All drugs should be taken with caution. If the remedy is chosen incorrectly, it will cause hypersalivation and more serious consequences. If surgery or radiation is required, then you should be aware that this can lead to abnormalities in the form of caries and facial asymmetry. All decisions about treatment are always made deliberately, the most appropriate method is chosen based on the individual characteristics of the child and expediency.
In some cases, speech therapy massage is required for treatment, since hypersalivation makes it difficult to pronounce sounds.
If the cause of salivation is physiological, then it does not require medical intervention and disappears on its own after a while. In the case of pathology, it is necessary to identify the primary disease, which was the result of hypersalivation, and conduct a course of treatment.
Drooling in babies and their causes
Let’s try to figure out what, in fact, is associated with abundant saliva in the first year of a child’s life. The salivary glands are formed by the age of two to three months, it is at this time that parents notice that their baby is actively blowing bubbles. As a rule, the baby does not know how to swallow saliva, so it seems to the mother that there are too many of them.
Saliva is also a kind of antibacterial agent. It contains a special substance that has antimicrobial properties.
Since children put everything into their mouths, saliva fills
All newborn babies in the first month are distinguished by the fact that their salivary glands have a rather low level of secretory activity. It is not common for a one-month-old baby to drool a lot with blisters in general, but there are several factors that can cause excessive salivation:
Immaturity of the system that regulates salivation. However, by one and a half months, saliva secreted in large quantities will become normal, since it is by this age that the salivary glands begin to work more actively.
Allergic rhinitis or infection of a bacterial or viral nature. Such reasons are quite likely if there are no other symptoms (for example, the first teeth are climbing in the crumbs, and therefore he sucks his fists all the time).
Birth defects. In this case, you should consult a pediatrician.
When a 2-month-old baby drools, it is most often associated with the inability to swallow them – this physiological process naturally occurs only during feeding. During this period of time, the endocrine glands and salivary glands simultaneously begin to function in the baby’s body.
Diseases, such as rhinitis, can cause increased salivation in babies
Causes of hypersalivation
Before you speculate, you need to find out for sure whether the child’s salivary glands really work in “enhanced mode” and produce more secretions. It often happens that there is no violation of the secretory function of the salivary glands at all, and the normally produced saliva flows arbitrarily from the child’s mouth only because the child does not swallow it for some reason. In this case, they speak of false hypersalivation. In other cases, a violation can be recognized by the daily amount of secretion produced, which should not exceed the norm of 2. 5 (!!!) liters.
However, let’s take a closer look. So, among the causes of increased salivation, the following are distinguished:
Physiological phenomenon as a variant of the norm.
Usually, in children under six months, this phenomenon should not be emphasized, since any specialist in the vast majority of cases will say that this is normal. Salivation (ptyalism) occurs at the level of unconditioned reflexes and soon disappears;
Often characterized by a similar symptom, and it can occur long before the appearance of the top of the tooth above the gum. The soft tissues of the gums are injured, the child may feel itching, express concern, try to “scratch” the gums with improvised objects. In response to irritation, the secretory function of the salivary glands also increases;
Allergic rhinitis in an allergic child
Swallowing disorder may be due to swelling of the nasopharyngeal mucosa, the child constantly breathes through the mouth, which is constantly open. This condition may be the cause of ptyalism;
Swallowing problems and jaw anatomical features
Drooling is often the cause of a child having difficulty swallowing (or simply forgetting to swallow) or having some anatomical features such as malocclusion;
Oral infections
The body’s natural defense mechanisms are activated by the presence of pathogens in the mouth, nasopharynx and middle ear area. So the baby’s body fights bacteria, literally washing them out with saliva, which also has a weak antiseptic effect;
problems with the gastrointestinal tract
In most cases, diseases of the digestive system are accompanied by this symptom;
Neurological disorders
If the central nervous system is disturbed, increased salivation may be observed as a symptom, the causes of which lie in a brain tumor, cerebral palsy and other congenital or acquired diseases;
Often characterized by nocturnal salivation;
Poisoning by heavy metals and hazardous chemicals
May be the underlying cause of this symptom. In this case, salivation is accompanied by a number of other signs; when taking lithium-containing drugs, ptyalism is noted as a side effect.
{reklama2}
Care of the skin around the mouth with increased salivation
At this stage, try to keep clothes dry on the chest: change blouses more often or hang a bib on the neck with a waterproof lining. Sometimes around the mouth or on the chin, irritation may appear in the form of small pimples that resemble a rash, or red spots due to constant moisture.
In this case, lubricate the damaged areas with baby cream at least a couple of times a day (ideal with vitamins A, E, chamomile extract). When wiping with a handkerchief, make gentle blotting movements, do not rub dry already irritated skin.
Is there a problem if a child sticks out his tongue: in what cases should I be worried?
The fact is that the baby is not yet able to talk, so if he wants or needs something, he tries to express a request using gestures and facial expressions. Language becomes a kind of communication tool. Seeing that the baby stuck out his tongue, it can be assumed that he is hungry or wants to be paid attention to. Another reason is that the baby is sick and his health leaves much to be desired.
Parents should be wary if the baby sticks out his tongue not only while playing, but continuously, even during sleep, without pulling it back. Here it is advisable to sound the alarm and pay a visit to the pediatrician. Having examined the little one, he may send his parents with him for consultation with other specialist doctors.
Tongue protrusion
The causes of a permanent reflex such as tongue demonstrating by an infant may be neurological, endocrine or infectious. The presence of some alarming symptoms will be an indicator of a particular disease, which we will give below.
Hypothyroidism
Occurs due to problems with the thyroid gland. The main reason is iodine deficiency in the body, the level of which is determined by a blood test. The test is carried out in the hospital, a blood sample is taken from the baby from the heel.
In addition to the protruding tongue, the baby has a number of other signs in the form of:
Yellowish or pale skin tone.
Dry, scaly surface of the epidermis.
Slow mental and physical development.
Severe swelling in the mouth, due to which the tongue does not fit, protruding outward.
Blueness of the area near the nose and lips.
No weight gain.
Development of stable constipation.
This case involves hormone therapy as a treatment and examination prescribed by a doctor.
Damage to the trigeminal nerve – associated with malfunctions of the thyroid gland. Causes: transferred acute respiratory infections or any injuries of the face.
Additional symptoms include:
Lack of movement of the facial muscles, change in facial expressions (the baby stops crying, smiling, he no longer has facial wrinkles).
Lips noticeably swell.
The face becomes asymmetrical.
There is a retraction of the eyelids.
Chin offset to the side.
Maybe due to atrophy
The baby is being treated with medications and vitamins by a neurologist. In addition, the child undergoes MRI, ultrasound. Treatment is mainly medical. Additional treatments include massages and physiotherapy sessions.
Candidiasis
Infection that affects the mucous membranes of the mouth. The reasons may be: reduced immunity and regurgitation more often than usual.
The child sticks out his tongue, besides this is noticeable:
Appearance of a whitish, curd-like plaque in the mouth.
Redness and inflammation of the gums, uvula, palate.
The appearance of a grayish-yellow plaque in the absence of proper treatment.
This case requires a consultation with an infectious disease specialist, as well as a dermatologist, who will prescribe the necessary ointment and topical solution, as well as a complex of vitamins and drugs to improve the immune system.
The main condition that a nursing mother must fulfill is to follow a special diet.
Stomatitis
Appears when viruses or bacteria are found in the baby’s body. Notable symptoms include:
Inflammation, redness and swelling of the mouth.
The appearance of ulcers on the tongue, in the region of the palate and gums.
Increased body temperature.
The baby becomes capricious, refuses to eat.
Sleeping restlessly.
Due to stomatitis
Parents can get help from: a dentist, an immunologist, an infectious disease specialist, who will prescribe a complex of vitamins, immunity modulators, as well as the necessary ointment, medicinal solution, antiviral/antibacterial medicines.
Causes: Birth damage or infection such as inflammation of the brain.
Symptoms that require a mandatory visit to the doctor:
If the girth of a children’s head is more age -related norms
The baby’s head is all the time, the fontanel swollen
Muscles are clearly tense,
pens and chin are trembling
Cauline,
9009 9009 9009 9009
An urgent consultation of doctors is recommended: a neuropathologist and an ophthalmologist, who will prescribe a CT scan of the brain, as well as neurosonography, which can be used to study the condition of the fundus. In the process of treatment, the functions of blood circulation are improved. In addition, special gymnastics, a massage procedure and taking vitamins are prescribed.
Weakness of the muscles of the tongue
Disease caused by birth trauma, abnormalities in the endocrine system, premature birth. The transmission of infections has the same effect.
If the following is added to the leaning of the tongue:
The baby is a lethargic, sedentary
for a long time sleeps
does not gain
Poorly eats
lags behind the physical development
9000 should be addressed to a neurologist. Treatment: taking medications, taking a course of massages, doing gymnastics.
Due to weak muscles of the tongue
When parents see that the child’s tongue is sticking out, the first thing to do is to carefully examine the surface of his skin and examine the condition of the mucous membranes. Having found alarming signs, it is worth paying a visit to the pediatrician, who will make an accurate diagnosis and prescribe treatment.
When drooling is not normal
If increased salivation is explained by the next stage in the child’s development, then he should not have any other signs of pathology. The baby should remain cheerful, calm, eat with appetite, play, walk and feel great, with the possible exception of redness and maceration of the skin on the chin, which occurs in children due to constant irritation with saliva.
Sometimes a 2-month-old baby drools because of:
ARVI or colds – stuffy nose, fever and profuse salivation – these are the main signs of illness in a baby;
allergic reactions – most often appear in young children when plant pollen, dust, detergent fumes and other allergens enter the body. It is quite easy to distinguish allergic rhinitis, in addition to a large amount of saliva, the child’s nose is constantly stuffy, his eyes turn red and watery, he sneezes and coughs;
endocrine disorders – diseases of the thyroid gland at this age can be manifested by profuse salivation, but the child’s mouth is constantly open, the tongue is thickened and may not fit in the oral cavity, and there are other signs of developmental delay;
neurological disorders – in this case, the child, in addition to profuse salivation, has several other signs of developmental disorders – pulsation of the large fontanelle, constant crying, developmental delay – the baby does not hold his head in weight, cannot lift it while lying on his stomach, and so on.
If you think that your child is drooling too much or something is bothering you in his behavior and development, seek advice from a pediatrician or neurologist – a specialist will help you dispel all your fears and simply enjoy every stage of your baby’s growth .
Pediatrician – Questions for a specialist | Children’s Clinical Diagnostic Center in Domodedovo
04.02.2021 Yuri
Electrocardiography with DFN.
Conclusion.
Initial YEKG: sinus arrhythmia with a HR of 73 beats/min. EOS is located normally.
After a physical load, 25 squats. CHS increased. by 42% up to 104 bpm..
After 5 minutes, the ECG returns to baseline.
Please tell me what this means and how it affects sports.
Hello Yuri! Unfortunately, it is not possible to answer your question. The question does not specify the age of the person who underwent the ECG. It would be wiser to contact the doctor with the result of the performed ECG, who ordered the examination, leads the patient and knows a lot more about his state of health. Sincerely, the management of OOO “DDC”
03.02.2021 Anna
Hello! A child of 8 years old, passed a general blood test for a medical examination, leukocytes 3.43, normal 4.5-9; erythrocytes 5.11, at a rate of 3.8-4.9; monocytes 13, at a rate of 3-9%; neutrophils total 1.1 at a rate of 1.78-5.38. The rest of the indicators are within the normal range. Is this critical deviation from the reference values and what can this indicate? What follow-up is needed?
Responsible Kharitonova Marina Alekseevna Head physician, pediatrician, member of the Union of Pediatricians of Russia
Good afternoon, Anna! To avoid erroneous conclusions, we do not comment on the results of analyzes on the site. It is most correct in your case to visit the pediatrician with the child. Based on the results of the examination, the doctor will give a more accurate conclusion about the state of health of the child.
02.02.2021 Lyudmila
Hello, the child is 7 months old. on breastfeeding, on complementary foods (banana, apple, fruit puree) rarely goes for a long time, maybe 3-4 days or more, then we put a candle – we went, and then we wait again. Please tell me what to do?
Responsible Shvetsova Elena Alexandrovna Pediatrician
Hello! Judging by the listed products, only fruit puree is included in complementary foods. By 7 months, the child’s diet should already include vegetable puree, cereals (start with gluten-free dairy-free ones), vegetable and butter, yolk, meat. Of course, everything should be introduced gradually, starting with small doses, bringing to the desired volume. It is recommended to keep a feeding diary to track reactions to the product. Detailed recommendations on the correct introduction of complementary foods should be discussed with the pediatrician at the reception. Detailed feeding schemes can be found on the website of the Union of Pediatricians of Russia in the information for parents section. Subject to all the rules for the introduction of complementary foods, the problem with the stool will go away.
02/01/2021 Alexandra
Child 3.5 months old, fully guarded. Up to 3 months poop every day 1-2 r per day. Now she poops every 4 days. Consistency – creamy, yellow. Is this the norm or not? Feeling good
Replies Shvetsova Elena Aleksandrovna Pediatrician
Hello! Mom can be advised a balanced diet with enough vegetables and fruits. Observe the drinking regimen.
02/01/2021 Tatyana
Hello. The child is 1.5 years old. Stool tight, crying when pushing. Eats from the common table, constantly drinks milk, juice, water. There is no allergy to anything.
Hello. I recommend to pass the analysis of feces, scatology, ultrasound of the abdominal cavity, if not done. Visit a pediatrician or gastroenterologist for examination and treatment.
02/01/2021 Irs
Hello! My baby is 4 months old. We have changed Nutrilon Comfort nutrition. Third day dark green stools. A little temperature. And drooling due to teething. Please tell me why a child can have green stools? And what to us analyzes to hand over?
Responsible Kiseleva Lyudmila Ivanovna Pediatrician, doctor of functional diagnostics
Dear Irs!
Regarding the change in the stool for a child of this age, it is necessary to consult a pediatrician or a gastroenterologist, since this may also be a manifestation of an infection.
To exclude an infectious nature, tests will be prescribed by a doctor. In young children, the colonization of the intestines with microflora is not always only the necessary world-organisms, but also conditionally pathogenic, and sometimes pathogenic.
Come to our center, we will try to help in resolving the situation that has arisen for your child.
01/30/2021 Ekaterina
Hello! Baby 11.5 months. In the last two weeks, during defecation, she sobs from pain. At first he starts to push and then he starts to cry very hard. When washed, it feels like particles of sand. Meals are separate, canned by age. A mixture of 600 ml per day. The chair is not hard, but decorated.
Responsible Luneva Galina Georgievna Pediatrician
Good afternoon Ekaterina. There is very little information on breastfeeding. I recommend to take a fecal analysis for scatology and make an appointment with a gastroenterologist.
01/30/2021 Anna
Hello, my son is 11 years old, 5 years old poops in his pants or in the bathroom 6-8 times a day, he doesn’t sit on the toilet, went to a psychologist, it didn’t help, which doctor should I contact?
Responsible Ermolaev Sergey Sergeevich Candidate of Medical Sciences, neurologist, doctor of functional diagnostics
Hello Anna. The situation is not easy. Most likely, the boy has encopresis (fecal incontinence, inability to control the act of defecation). The reasons can be both developmental pathologies and disorders in the work of the gastrointestinal tract itself, as well as psycho-neurological abnormalities. More information is needed about the child, the disease, whether there has been such a situation for all 5 years, whether there have been episodes of remission, etc. Consultation with a gastroenterologist, neurologist, and also a psychiatrist is necessary.
01/30/2021 Anna
Hello. Tell me please, the child is 7 weeks old, on ultrasound of neurosonography, the child was given a conclusion: the distance of the lateral ventricles of a mild degree, what does this mean and is it dangerous? (The size AB of the anterior horns is 26mm, body: left 3.9, right 4.2, posterior horn 8.7, 9.0)
Answer Ermolaev Sergey Sergeevich Candidate of Medical Sciences, neurologist, doctor of functional diagnostics
Hello Anna. To assess the condition of the child, an integrated approach is needed. Not only numerical values are important, but also a clinical assessment of the neurological health of the child. This is important, because we do not treat the results of tests and indicators of instrumental examination, but the person. At this age, it is extremely important to know how the pregnancy, childbirth, the presence of infection, hypoxia, etc. proceeded. At the same time, I will give some standards for 1.5-2 month old children. Lateral ventricles: anterior horns up to 4 mm, occipital horns up to 15 mm, body 2-4 mm. Third ventricle up to 5 mm, fourth ventricle up to 4 mm, interhemispheric fissure 2-4 mm, large cistern up to 6 mm, subarachnoid space up to 2 mm. Of course, it is important to note that individual sizing is possible.
29.01.2021 Alina
Hello. The child is on mixed feeding. Before that, everything was normal with the stool. But for 2 days already, liquid mustard-colored stools began and with a pungent odor. Today it was dark green 1 time. Is it worth worrying? The child himself, in principle, eats well, sometimes he is naughty and does not sleep.
Responsible Kiseleva Lyudmila Ivanovna Pediatrician, doctor of functional diagnostics
Dear Alina! You did not indicate the age of the child, although if such symptoms appear, it is necessary to examine the child before recommendations and talk with you to clarify some points, including your diet. For a young child, even minimal complaints can be the first signs of a serious bowel problem.
I invite you to a consultation in our center, we will try to help in resolving your situation.
Newborn sleep
Newborn sleep is the most exciting topic that haunts young parents. Why does he have such a hard time sleeping? Why does he often wake up at night to feed? Why is he sleeping so restlessly? As part of our article, we will answer these questions, as well as consider the existing violations of children’s sleep.
When there is nothing to worry about
Let’s look at a few cases in which you can be sure that your baby is growing in perfect health.
A newborn cries and grunts in his sleep
Why does a newborn cry or grunt in his sleep? Does he feel any discomfort, is he in pain? Young parents do not know what to do in such a situation and anxiously rush to see a doctor. We hasten to reassure you. Everything is fine.
Crying or groaning in sleep is normal. Studies show that a similar reaction occurs due to dreams. In addition, babies in this way check the presence of parents nearby, instinctively looking for your protection and support. And if he doesn’t find her, he starts to cry for real. Of course, this requires your intervention.
However, you should not react with excitement every time a newborn starts in his sleep. If you do everything right, then over time the child will learn to calm down on his own. Otherwise, he will require excessive care with age. The skill of self-soothing is developed in children during the first year of life. And it is your duty to contribute to this.
The child often wakes up at night
Another issue that worries parents is the regular awakening of the child. This is also normal. Awakening occurs due to the high frequency of sleep cycles. In infants, they occur more often than once an hour. Older children wake up less frequently and tend to fall asleep immediately. However, with the inability to calm down as a result of excessive attention from the parental side, sleep disturbances occur.
A newborn starts in his sleep
Why does a newborn start in his sleep? – no less relevant for young parents question. This occurs during sleep cycle changes due to the immaturity of the central nervous system. And, of course, this is not a cause for concern. It goes away with age.
When to seek help
Now let’s look at the cases in which your baby needs specialist help. The most common insomnia is difficulty falling asleep, as well as regular awakenings. There are the following causes of insomnia in children:
Secondary – occur as a result of any disease. For example, insomnia in children can occur due to fever or abdominal pain.
Primary – not associated with any disease. The main cause of insomnia in children in this case is the behavior of the parents or the child during the time associated with sleep.
Secondary causes of insomnia in children are treated by treating the disease that causes it. Primary – by adjusting behavior patterns during the period of falling asleep. Let’s see how to do it.
Behavioral insomnia
Irregular behavioral patterns when falling asleep include:
falling asleep in parents’ bed or in arms;
with finger in mouth;
during a meal with a bottle in the mouth.
Most parents will ask, “What’s wrong with that?” Everything is very simple. If the baby wakes up and does not find nearby what made him fall asleep, he will begin to demand it. To eliminate insomnia in children, it is necessary to observe the correct behavioral patterns before going to bed. What are they?
It is necessary to follow a certain algorithm for preparing for sleep every day. Everything is simple here. Bathing, eating, short-term stay at the crib and leaving the child alone with him. Teaching a baby to this sequence is the key to a comfortable sleep. Both for himself and for his parents.
The “subject mediator” will help develop the described behavioral model in the child. This is a certain item that is next to the baby during sleep. For babies, this is, for example, a diaper that keeps the mother’s smell, and for those who are older – a favorite toy. All this gives children a sense of comfort and suppresses the excitement during awakenings, and also allows you to feel your closeness.
What if the child does not want to adopt a certain sleep pattern? Every now and then he goes to the toilet, asks for water, or even comes to bed with his parents. In no case do not put pressure on the child. This will only make the situation worse.
It is necessary to gently persuade the child to comply with the regimen. This will set the baby’s brain for sleep and prepare him for parting with you. So, for example, you can strictly determine the number of fairy tales that you read before going to bed.
Eating disorders
Another cause of insomnia in children is the absence of a fixed meal schedule. Many parents feed the child haphazardly – whenever he begins to express dissatisfaction. Feeding in the evening should occur clearly before bedtime. This will develop a certain reflex in the child.
In addition, there are other ways to treat insomnia in children.
Treatment of insomnia in children
What you can do:
Establish a clear daily routine and meal schedule for your child so that he naturally falls asleep at a certain time.
Use the baby’s crib for sleeping only – do not play or eat in it.
The use of special drugs that improve sleep is not recommended. They can be used occasionally to adjust the regimen. And then strictly individually, after consultation with a doctor.
In case of secondary causes of insomnia, the treatment is to eliminate the pathology that caused insomnia. For this, you need to contact your pediatrician. During treatment, he will prescribe sedatives. However, at the same time, one should not forget about the daily routine, diet and behavioral therapy.
If you are unable to make your child follow the routine on your own, contact the Seven Doctors multifunctional health clinic in St. Petersburg. To make an appointment, please call 8(812)677-0-777. A professional sleep specialist will advise you on all your questions and select the most convenient time for your visit.
See also:
Abdominal ultrasound
Cost of physiotherapy
Sleep treatment in the clinic
Prices for spirometry
The main food of babies is milk (breast or formula). It contains many different nutrients (proteins, fats, carbohydrates), which, with the help of special digestive enzymes, are broken down into simple components and digested. But in young children, the gastrointestinal tract is still immature, there are few enzymes in it, others are not at all or they are not yet working at full capacity. When the baby grows up, there will be more enzymes, the digestive system will mature, but for now there may be various problems with it.
All milk (women’s, cow’s, goat’s, artificial mixtures) and dairy products contain the carbohydrate lactose, also called “milk sugar”. In order for lactose to be absorbed, the lactase enzyme must break it down, but if the child has little or no lactase enzyme, then lactose is not broken down and remains in the intestine. As a result, there is always a large amount of milk sugar in the intestines, which begins to ferment, and where there is fermentation, conditionally pathogenic flora actively reproduces. What we feel during fermentation: intestinal motility increases (it rumbles), plus gas formation increases (the stomach swells). But in an adult, this is usually a one-time situation due to some inaccuracies in nutrition, and it quickly passes. But in babies, everything is different, especially since they lack the enzyme not once, but constantly. What it looks like: The milk sugar lactose retains water, hence loose stools. In the child’s stomach, “rumbles and boils”, colic begins, the stool becomes frothy, greens, mucus and even blood may appear in it. If at first the stool was liquid, then constipation appears, and all this changes in a circle: yesterday there was diarrhea, today and tomorrow there is no stool at all, the day after tomorrow it is liquid again. And the most unpleasant thing is endless colic and endless crying, there is no rest for both the parents themselves and the baby. Mom at some point notices that the baby is crying just after feeding, and then a variety of advice falls upon her. “Your milk is bad, better give the mixture,” says the beloved mother-in-law. “Only breasts and nothing else!” – advise breastfeeding gurus. As a result, the mother tries one thing or the other, but neither breast milk nor artificial mixture gives relief to the child. Colic, crying and problems with the stomach and stool continue. The parents are in a panic because they don’t understand what is going on. In fact, this is a typical picture of bright lactase deficiency (LN), or insufficient production of the lactase enzyme.
various reasons
There are several types of lactase deficiency, and it is with them that confusion arises.
Congenital lactase deficiency is a genetic and very rare disease (one case in several thousand newborns), it is difficult to confuse it with something, since it is very difficult. The diagnosis is made in the maternity hospital or in the first days after birth, the child does not have lactase at all, he quickly loses weight, he is immediately started to be fed intravenously or through a tube. Some experts (but not doctors) on breastfeeding read once that congenital lactase deficiency is an extremely rare disease, and that’s all – they further began to assure young mothers: “In fact, LN is extremely rare, you don’t have it, you don’t need to listen to doctors “, etc. Yes, congenital LN is a rare disease, but the key word here is “congenital”, and there are other types of lactase deficiency.
Transient lactase deficiency in infants . And this is exactly the condition that occurs very often. The baby was born, and so far he still has little lactase enzyme, plus little normal intestinal microflora. Hence the colic, and loose stools, and mucus, and greenery, and crying, and the nerves of the parents. After a while, the child’s digestive system will fully mature, all enzymes will begin to work actively, the intestines will be populated with what is needed, and “lactase deficiency” will disappear. Therefore, such a LN is called “transient”, that is, temporary, or passing. It passes for someone a month after birth, for someone longer – after six to seven months, and there are children in whom lactase deficiency completely disappears only by the year.
Secondary lactase deficiency. This condition appears if a person has had some kind of intestinal infection, and it does not matter if it is an adult or a baby. For some time after the illness, the child does not tolerate milk (any), and then with proper nutrition and sometimes even without treatment, everything quickly passes.
Lactase deficiency in adults. There are people in whom the lactase enzyme begins to be lacking only in adulthood, this happens for various reasons: for some, lactase ceases to be produced in the right amount after some kind of illness, for other people, the activity of this enzyme simply fades over time by itself. yourself. As a result, at some age, a person begins to tolerate milk and dairy products poorly, although before that everything was fine. The symptoms are the same as in babies: he drank milk and after that the stomach rumbles, boils, and the stool is liquid. Sooner or later, a person realizes that milk is not his product, and simply stops drinking it in its pure form.
what to do
If there is transient lactase deficiency, then what to do with it? First you need to understand if it exists at all. Why does the child have problems with the stomach, stool, why does he cry all the time? Is it neurology, common colic, errors in the mother’s diet, an inappropriate mixture (if the baby is bottle-fed), improper breastfeeding technique, lactase deficiency, or a reaction to the weather? It can be difficult to figure it out right away, but if the tests show that there is lactase deficiency, then it is most likely in it. Now what to do next – treat it, wait for the enzymes to mature, or something else? Firstly, everything here will depend on how much the enzyme is lacking and, therefore, on how much LN worries the child and parents. Some children lack the enzyme quite a bit, so their colic is mild and children cry quite normally. Plus, the violation of the stool is also not very bright: there are a couple of times a slightly liquefied stool, but that’s all. In other children, the lack of lactase is more pronounced, the child does not cry, but simply yells after each feeding, if at first he gained weight well, then after two months the increase is minimal, problems with stools begin in parallel (day – constipation, day – diarrhea), stool sometimes green, sometimes with mucus. Atopic dermatitis appears on the skin (the skin is the first to react to problems with the gastrointestinal tract). Parents have no rest day or night: the baby cries – he is fed – he cries again, they try to calm him down in other ways. But nothing helps. Mom and dad are in a panic, and no one has the strength anymore.
If parents see that the child may have signs of lactase deficiency, that he needs help, first of all, you need to look for a good doctor. Only an experienced pediatrician will be able to figure out why the baby has colic or green stools, what the numbers in the tests say, and what is the norm for one baby and the pathology for another. And of course, it is not necessary to cancel breastfeeding and immediately prescribe lactose-free or low-lactose artificial mixtures (even as a supplement). By itself, milk sugar lactose is very necessary for a child, when lactose is broken down, its components (glucose and galactose) go to the development of the brain, retina, for the life of normal intestinal microflora. So do not completely eliminate this sugar, you need to help it break down. With a strongly pronounced LN, the missing enzyme is given before each feeding (it has long been learned to produce and it is sold in pharmacies), with a dim clinic, its dose can be reduced. And it is also possible that there is lactase deficiency (even according to tests), but it does not need to be treated, there are almost no symptoms.
But what cannot be done is to listen to non-specialists who deny either lactase deficiency itself or its treatment. They see the cause of all problems with the child’s stomach and stool either in the wrong technique of breastfeeding, or partially admit that there is immaturity of the enzyme, but this is natural and will pass by itself. Yes, for some, LN is expressed easily and will pass quickly, but what about those parents whose child yells day and night, covered with a crust from atopic dermatitis and stopped gaining weight? Wait for the time to come and the enzymes to mature? Alas, with pronounced lactase deficiency (even if transient), enterocytes (intestinal cells) often suffer, so it is simply necessary to help such a child.
If you see that your baby has signs of lactase deficiency, look for a doctor who is committed to maintaining breastfeeding and has extensive experience. He will definitely help to find out why the baby is crying, why he has a stomach ache or has problems with stool. And then the life of the parents and the child will return to normal.
“Transient” (temporary) lactase deficiency in someone passes a month after birth, in someone longer – after six to seven months, and there are children in whom lactase deficiency completely disappears only by the age of one
If the tests show that there is a lactase deficiency, then the matter is most likely in it.
Do Men Go to Baby Showers? Traditions and Etiquettes Today
Baby showers are gift-giving events meant to celebrate the expected coming of a baby into a family. Usually, a close friend or family member plans the event for the parents-to-be and takes on the job of creating the guest list with the expectant parents and afterward, sending out the invitations. Parents-to-be and baby shower planners are often left wondering whether or not men should be put on the guestlist or left out.
Historically, baby showers have been an exclusively female affair. Nowadays, men do go to baby showers and dads-to-be are perfectly welcome to celebrate showers with their partners. Male friends and family members making appearances at baby showers have also become increasingly common.
With attitudes towards pregnancy and child care shifting in recent years to include fathers more, men are more likely to be open to the idea of celebrating baby showers. Fathers are also becoming more hands-on parents than ever before – it makes sense for the dad-to-be to take want to take part in celebrating his baby’s arrival.
There are no hard and fast rules to baby showers, and who you want to invite is up to you entirely. Feel free to invite (or disinvite) who you want. If you would like to have men at the baby shower, go ahead and invite them. If you would prefer celebrating a baby shower with women only, that is completely okay too.
Baby Shower History
The earliest forms of baby showers and gift-giving may have emerged in the Middle Ages when gift-giving was overseen by appointed godparents who would give gifts to the baby on the day of their baptism.
Later on, in Renaissance times, new mothers would be gifted with a Desco da parto, or a birth tray painted with intricate pictures and well-wishes for the mother and baby, to symbolize the successful birth of a baby. Because infant and maternal mortality were so common in those times, successful childbirth and motherhood were celebrated lavishly. Because infant and maternal mortality was so common in those times, successful childbirth and motherhood were celebrated lavishly.
The modern tradition of showering expectant mothers with gifts came about during the post-World War 2 baby boom in the 1950s and 1960s when expectant mothers were gifted with household and commodities and goods that could become rather expensive in light of the financial toll that child care brings. The tradition of having a close friend or family member plan the event also originates in this time.
Traditionally, baby showers were exclusively open to women. Aside from being a celebration for an expectant mother, they were seen as an opportunity for women to “talk shop” about pregnancy and childbirth, topics which were back then deemed too intimate to be discussed in the company of men.
Baby Shower Traditions and Etiquettes Today
Modern-day baby showers are casual, intimate gatherings celebrated with close friends and family. Depending on the preferences of the expectant parents, they may be casual events celebrated at home or formal events held at nice venues. And of course, guests are expected to bring a shower-appropriate gift.
What the guest list looks like may also depend on who is throwing the baby shower. A shower thrown among the expectant parents’ friends is more likely to have an equal number of men and women in attendance as friends will likely be close in age and have similar attitudes towards men attending baby showers.
On the other hand, a shower thrown by a family member for family will probably have a male attendance that skews towards the younger generation.
While some people may still prefer to have female-only baby showers, co-ed or mixed-gender baby showers are becoming more and more common, with male relatives and even some of the expectant dad’s friends along for the celebration. Some fathers may even hold their own versions of baby showers, sometimes known as a “dadchelor party” or “diaper party”.
Co-ed Baby Shower Etiquette
Gift Etiquette
Both mom and baby can end up with quite a large haul after a baby shower. Items such as diapers, baby clothes, toys, breast pumps, and luxury items for the mom are all common baby shower gifts.
If you happen to be invited to a co-ed baby shower, consider bringing along a gift for the dad-to-be. Diaper bags and baby carriers made specifically for fathers and even items such as kitchen gadgets and edible treats make great baby shower gifts for fathers.
Conversation Etiquette
While moms may share stories and talk about their experiences with pregnancy and childbirth, men may not be as keen on discussing the nitty-gritty details of prenatal and postpartum care.
Chances are, dad is experiencing just as much anxiety around his partner’s pregnancy and may need some coaching on how best to support his partner. One of the advantages of having a co-ed baby shower is getting to have a few veteran fathers in attendance to give the dad-to-be some advice and words of wisdom while the ladies have their own time together.
Food Etiquette
Food is a must at any gathering, baby shower included. While traditional baby shower food may consist of dainty finger foods and pink and blue baby-themed treats, you may also want to have more substantial eats prepared at a co-ed baby shower.
Consider throwing a backyard cookout-style baby shower and task the dad-to-be with the grilling. This allows him to play a more significant role in the shower and provides him with a nice conversation starter for getting to know some of mom’s friends.
Ideas and Traditions for Co-ed Baby Showers
Have Co-ed Planners and Hosts
Having female and male hosts will bring 2 different perspectives into the plan and help balance out the masculine and feminine aspects of the event, making guests of all genders more likely to feel included on the day itself.
If the female host is a close friend of the mother, try having her male counterpart be a friend of the father to better incorporate elements that both parents will enjoy. Bonus points if the hosts are parents themselves – it can be a big help with planning and hosting if the host and hostess have lived the other side of the event themselves.
Heartier, More Filling Food
While you don’t have to skip out entirely on the dainty pastel cookies and finger sandwiches, try incorporating heavier, more filling foods into the menu. Some menu ideas for co-ed baby showers are backyard barbeques and even buffet-style full lunches.
If mom-to-be is comfortable with it, you can even set up a few beers (alcoholic or non-alcoholic) for the dad-to-be to enjoy with his friends while the expectant mother enjoys a few mocktails.
Entertainment Ideas
Traditional baby shower games such as blindfolded baby food tasting and guessing the circumference of mom’s belly with string are outdated and may not be as enjoyable for male guests.
Go for games that couples can play together in teams such as trivia games about the parents-to-be and pacifier beer pong. Guys against girls games like a blindfolded diaper changing challenge on dolls. Other interesting game ideas for men at baby showers include stroller races and baby bottle chugging contests.
Gender Neutral Shower Favors
Not only do shower favors serve as mementos of the event, but they are also a tangible way of thanking guests for coming.
Instead of beauty products and other traditionally feminine party favors, try sending guests home with chocolates or other sweets that everyone can enjoy. Another popular idea for gender-neutral shower favors are personalized honey jars and mini champagne or sparkling juice bottles.
Baby Showers For Men Are Here, And They’re Way Better Than Ours
Parenting
byJerriann Sullivan
Updated:
Originally Published:
Say goodbye to boring games and hello to a lot of beer
Rejoice! The baby shower has gotten a makeover and is now officially fun. Technically the parties are called “baby showers for men” or “Dad-chelor parties. ” But they sound so much better than the traditional one that it could be time to retire the classic baby shower.
The trend is gaining popularity quickly, according to Pinterest. The term “man showers” increased by 149% and “co-ed showers” increased by 255% in 2015, Mashable reported. Co-ed showers are for mom and dad, but the relaxed vibe the dad-chelor parties specialize in is taking over the co-ed parties as well.
So what exactly goes into a baby shower for men? Well, besides the dudes, a lot of beer and typically a giant pile of diapers. There are no weird poop games or pretending to care about the onesie a distant relative sent. Instead, the host buys a ton of beer and makes chicken wings or other assorted snack foods. How many showers have you been to where the only food available were five different kinds of salads? Not at dad showers! Look at this spread of melted cheese, pretzels, and, of course, beer. Yes, please!
Image via Pinterest/Chicago Now
Instead of taking a quiz that only makes you feel bad for not knowing every fact about the miracle of childbirth, baby showers for dads have drinking games.
Image via Pinterest/ Catch My Party
Another great thing about baby showers for men is that the only gift guests are expected to bring, besides more beer, is diapers. And no one expects you to dress them up. You get to avoid the hassle of wrapping an oddly shaped toy, and the new parents leave with months worth of diapers. A win-win for everyone. Even the themed crafts at dad baby showers are better. No more elaborate pastel monstrosities that seem like a good idea but never end up looking like the picture. The standards for dad showers are much lower, so these “crafts” can be thrown together the day of the party. Look at this one – beer, ribbon, done.
Image via Pinterest/ This Heart Of Mine Blog
For the crowd that likes more than just beer.
Image via Pinterest/ Pizzazzerie.com
And for the overachiever who really wants to bring beer and diapers together.
Image via magicmaman.com
It is unlikely the traditional baby shower will disappear forever. It might be too hard to explain to Aunt Linda why all of your husband’s friends are drinking beer out of baby bottles. But with their surge in popularity it is likely you’ll be invited to one soon. RSVP “yes.”
Feature image of invitation via Etsy
This article was originally published on
proven facts – article on TChK
Many people jump into the hole at Epiphany, douse themselves with ice water after a bath, but forget about the beneficial effects of cold when they take a shower. But our grandmothers also talked about the benefits of systematic hardening. We learned what will happen to the body if we make this habit permanent.
What Science Says About Regular Cold Showers
There is a lot of worldwide research related to hydrotherapy in general and hardening in particular. One of the largest was held in the Netherlands in 2015.
More than 3,000 people aged 18 to 65 were divided into four groups. Every day the participants warmed up under warm water. The first group then took a 30-second cold shower. Participants from the second group stood under him for a minute, and from the third – 90 seconds. The fourth group (control) simply enjoyed the heat. The experiment lasted a month. All groups, except for the control group, were offered an optional extension of the practice for another 2 months. 64% of the subjects agreed because they liked it.
After a three-month follow-up, the researchers found that people in all three hardening groups were 29% less likely to take sick leave. Given the number of participants in the experience, this is indeed a significant result. But the length of stay under cold water did not affect the incidence.
Scientists believe that a cold shower tones the body, which ultimately affects all its functions.
Strengthens the heart and blood vessels
Alternating hot and cold water while showering is an easy way to improve blood circulation. Cold water causes blood to flow more actively to the organs in order to warm them. In addition, cooling is stressful for the body, leading to the release of adrenaline. Warm water reverses the effect: blood rushes to the surface of the skin. This is how a kind of “gymnastics” takes place, which strengthens the heart and blood vessels.
However, those who suffer from cardiovascular diseases should not practice it.
Restores muscles after training
Cold water has regenerative properties. No wonder ice is applied to bruises and bruises. After training, microtraumas form in the muscles. A cold shower will provide additional oxygen, improve blood circulation and relieve inflammation. Your muscles will relax and bounce back faster.
Helps relieve stress and prevent depression
Try standing under cold water for at least 5-6 seconds. You will see: a bad mood will be removed like a hand! You will feel a surge of endorphins that will make you more energetic and happier.
A few minutes of practice a day can have an antidepressant effect, says Nikolai Shevchuk, a scientist who conducted a 2008 study at the University of Virginia School of Medicine.
If you take a cold shower every day, your nervous system will gradually get used to a little stress. As a result, when a difficult life situation arises, you will meet it fully armed.
Promotes weight loss
During a cold shower, the body begins to actively burn brown fat, which is responsible for heat transfer, as a result of which more calories are spent. Stocks of white fat associated with excess weight also decrease: it begins to turn into energy-burning brown. Here is such a cycle.
In addition, according to Czech scientists, immersion in cold water speeds up metabolism by 350%! So an ice shower can really help improve metabolism and get rid of extra pounds.
Of course, you won’t lose weight just by taking a cold shower. It would be nice to focus on proper nutrition and sports. However, such a procedure will definitely become your faithful assistant in maintaining harmony.
Improves skin condition
Cold water helps shrink blood vessels and pores, reduce swelling and redness. Often people with dry skin feel itchy after taking a hot shower. One way to combat this is to lower the temperature of the water as much as possible. Then apply moisturizer.
Another bonus: cold water doesn’t wash away the sebum layer, the natural barrier that protects skin and hair.
How to take a cold shower
In the morning, a cold shower helps you wake up and tune in to the right wave. In the evening – calm the nerves and relieve tension. Most importantly, do not take it right before bedtime, otherwise insomnia may torment you. Best 2 hours before bedtime and 1 hour after waking up.
Warm up under lukewarm water and then turn on cold water abruptly.
Stand in a cold shower for 10 seconds, change to warm. Repeat 3-4 times.
Standing under cold water, try to breathe regularly, taking slow and deep breaths.
Increase the duration of the treatment each time. The ideal time is 5 minutes.
Stop practicing if you suffer from cardiovascular disease, colds, flu, fever. Be careful during pregnancy.
After a week of practice, you will feel that cold water is not so “burning”, and you have much more strength!
Hot water is also good if not abused
A hot bath at the end of the day is a pleasant and relaxing experience. However, please note that high temperature:
dries out the skin, damaging the cells of the epidermis, resulting in irritation and itching;
exacerbates acne breakouts;
weakens hair;
increases blood pressure and negatively affects the work of the heart.
Therefore, lovers of such procedures should be careful and follow the rules:
Experts recommend staying in water up to 37 degrees for no longer than 20 minutes.
Do not stay in water up to 40 degrees for more than 5 minutes.
Do not take hot baths more than 2-3 times a week to keep your skin hydrated.
Otherwise, the skin will lose a lot of moisture, and the heart and blood vessels will get too much stress.
The benefits of hot baths are sure to be, if you know the measure. Such procedures relax, lower blood pressure and stimulate the natural cleansing of the body. And it is even more useful to alternate them with a contrast or cold shower during the week.
Do you like to take cold showers or hot baths?
Rising shower: indications and contraindications
Most therapeutic baths and showers have a wide range of applications and affect the entire body. Unlike other balneological procedures, the ascending shower is used to treat diseases limited to the perineum and small pelvis. The ascending shower is indicated for the pathology of the female and male reproductive systems, diseases of the distal intestines, bladder and perineum.
During the procedure, the patient is placed in a sitting position on a special seat with an opening at the bottom. Under the hole is a shower head through which water is supplied under pressure. Rising shower water jets are directed upwards. The temperature of the water can be different, its choice depends on the nature of the pathology. In inflammatory diseases in the pelvic organs, warm water with a temperature of 38-40 degrees is used. The use of cool water with a temperature of 24-30 degrees has a tonic effect.
Rising shower water jets massage soft tissues, activate intestinal motility, improve blood circulation and lymphatic drainage in the pelvic area and perineum. As a result, intestinal functions are restored, the muscles of the perineum are strengthened, signs of inflammation disappear, blood supply and nutrition of the muscles and internal organs in the affected area are improved.
Indications for treatment with rising shower
The rising shower in the spa hotel is included in the treatment of gynecological and urological diseases. In gynecology, the ascending shower is used in the complex treatment of chronic inflammatory diseases of the female reproductive system, primary and secondary infertility, and menstrual dysfunction. In urology, the appointment of this type of balneotherapy is indicated for chronic prostatitis, impotence, neurological disorders with impaired sexual function. A course of treatment with an ascending shower is recommended for hemorrhoids, fissures in the anal region, inflammation of the rectum, chronic atonic constipation. For children, an ascending shower is prescribed for nighttime urinary incontinence.
Contraindications
Rising shower procedures are contraindicated in the presence of general contraindications to spa treatment, increased tendency to bleeding, acute infections and colds with fever, the presence of benign and malignant neoplasms.
The course of treatment requires 10-12 procedures. They take an ascending shower daily or every other day, an hour before a meal or one and a half to two hours after a meal.
The American Academy of Pediatrics (AAP) recommends placing your child on his back for naps and bedtime. This will help avoid risks such as choking, poor breathing, and even SIDS (Sudden Infant Death Syndrome).
But you can also avoid these risks by using a firm sleep surface, keeping soft objects and loose bedding out of the crib or bassinet, and avoiding overheating which can lead to problems with breathing.
Avoiding all these things will help you keep your little one safe while he sleeps!
You want to make sure that when your baby is asleep he’s in the safest position possible. Below we have discussed how to stop baby sleeping face down and make his sleeping comfortable. So let’s dig deep inside.
How To Stop Baby Sleeping Face Down
When placing the baby into his crib or bassinet, place him on his back, not on his side or tummy. Just like with adult beds, avoid using bumpers or blankets in your baby’s crib. Instead, attach fitted sheets snugly around the mattress. Although this may take extra time and effort when you change them, they will help keep out loose blankets and other things that could be hazardous to your baby’s health.
We all love our soft toys but we need to remember that they can cause suffocation if a baby accidentally gets one over their face while sleeping. Leave these out of sight and always check under the bedding for any mistakes before laying her down to sleep.
Make sure the sleeping area is not too hot for your baby by checking under his blankets or sheets to see if he’s kicking them away. If so, try using a lighter blanket or sheet. You may also want to adjust room temperature and humidity levels with a humidifier.
When you’re ready to stop baby sleeping face down, dress her in sleep clothes that are loose-fitting and made of soft, breathable fabrics like cotton to help avoid overheating. And make sure she doesn’t get too hot while playing since overheated babies can’t always control their body temperature well enough to regulate it correctly when sleeping.
If you are still finding it difficult to keep your little one on his back when sleeping, place him in the crib or bassinet while he is still awake. This way, you won’t have to worry about him falling asleep on his tummy before drifting off into dreamland.
You can also try putting your baby in the crib when she’s drowsy but not yet all the way asleep. She may adjust quickly to this new routine without much fuss.
If you are worried about SIDS , make sure that your baby doesn’t get too hot during sleep by using a thin blanket or sheet and avoiding thick pajamas and over-bundling. Also, don’t cover your baby’s face or head with stuffed animals or other soft objects since they might obstruct their breathing if they shift around in their sleep their mouth falls within the object.
Remember that SIDS is the leading cause of death among infants, and 90 percent of babies who die from it are under a year old. While we can’t prevent every tragedy, we know that following safer sleep guidelines for babies will help to reduce the risk. Getting little ones used to these practices when they’re young can mean a lifetime of better sleep habits.
So if you are wondering how to stop baby sleeping face down, follow all the safe sleep recommendations and you should notice a change in your child’s nap time almost immediately!
Why is my baby facing down?
Babies often fall asleep while breastfeeding or bottle-feeding and will naturally roll towards their stomachs as they drift off into deeper stages of sleep. Sometimes parents don’t know their babies are positioned this way until they wake up for nighttime feeding and find them sleeping face down.
If this is a common occurrence with your baby, try to encourage them to sleep on their backs from the very beginning of the feeding by using a wedge or rolled up blankets that raise the head of the bed just enough to keep his chin from falling into his chest as he feeds. In addition, always feed your baby in an upright chair and never on a couch or bed – even for daytime naps.
Also remember Don’t let him fall asleep while swaddled and think too hard about where he’s positioned (which can lull you right off to dreamland yourself). Once you find him like this it’s pretty easy to roll him over without waking him, but if he wakes suddenly it could be disconcerting for both of you.
Read more: Best baby carrier for preemie baby
What if my baby is more comfortable on his stomach?
Some babies prefer to sleep face down because it can give them a sense of feeling more tightly swaddled and wrapped up, which feels comforting and secure, so some parents choose this position for their babies by keeping them swaddled at night.
But remember: Babies should be able to wiggle out of the swaddle as they get older and become more active, moving into a sleeping bag or just loose blankets instead. If your baby’s doctor approves it, you might consider switching to something like the Zipadee-Zip (Zipadeezip) at bedtime instead of continued use of traditional swaddling.
It still provides that “feeling like baby is still swaddled” sensation, but doesn’t restrict the arms and leaves the option open for those who want to transition from swaddle before their babies become too mobile.
A good middle ground position (which we prefer and recommend) is to place your child on his back with a small blanket folded under his chest and tummy – not over his face – so that he feels more “burrowed in” and supported while still being able to breathe freely.
This also helps him feel like he’s being cuddled without giving him the feeling of being wrapped up tight enough to interfere with breathing or cause overheating problems.
Read More: BABY FLAILING ARMS AND LEGS WHILE SLEEPING – How to Deal With It
What are some ways I can keep my baby sleeping safely on her?
To keep your baby sleeping safe, avoid letting her sleep on a soft surface like pillows or fluffy blankets. Try placing her in her crib with just a fitted sheet over the mattress and adding another sheet if it feels too drafty throughout the night.
And always keep the room at a temperature that is comfortable for you – never hotter than 75 degrees F – as overheating can become an issue, too.
In addition, avoid any items that could cover your baby’s face while she sleeps such as loose-fitting sheets, long hair, or even stuffed animals.
All of these things pose a suffocation risk for the baby and should be avoided when she’s napping and sleeping – no matter what position she’s in.
What about pacifiers? Some babies use pacifiers to feel safer or more secure while they sleep, but pacifiers should never be used at the same time as a bottle.
Be sure to wait until the baby finishes drinking from his bottle before offering a pacifier. Also, make sure it doesn’t fall out of the baby’s mouth when you put her down for a nap or at bedtime and take steps to prevent this from happening by using the right size pacifier (smaller is better).
For example, if she’s still waking up crying because the pacifier falls out repeatedly throughout the night and day, try switching to a smaller one that will be easier for the baby to keep in her mouth during sleep and minimize these interruptions.
Keeping these tips in mind can help your little one become an expert at getting the sleep she needs when she needs it most.
What is the difference between “SIDS” and “suffocation”?
SIDS, also known as Sudden Infant Death Syndrome, is a diagnosis given when an infant dies suddenly and unexpectedly and after a thorough investigation, there does not appear to be an explanation for the death.
Suffocation is caused by a physical obstruction that prevents breathing such as something covering the nose and mouth. This can be accidental such as suffocating under bedding or intentional such as strangulation via hanging. Suffocation can occur during sleep so babies who are sleeping face down may be more at risk for this complication.
Sudden Unexplained Infant Deaths (SUID) is a term used to describe infants who die suddenly and unexpectedly with no explanation for the death.
This includes SIDS, suffocation, and other related causes such as accidental hanging/strangulation without being able to determine if it was intentional or not. This often occurs when a baby rolls into something that obstructs their breathing like loose bedding or plush toys that they can roll off of, but some babies are found after sleeping face down which adds another layer of danger.
Asking your pediatrician about safe sleep practices before settling on one method for you and your baby will help ensure the most comfortable night’s rest possible!
Should I worry if my baby sleeps face down?
Most babies should continue to be positioned for sleep on their backs. However, if your baby has specific risk factors that put him or her at high risk for SIDS (sudden infant death syndrome), then you should consult with your doctor before turning your baby onto his or her back.
How long can a baby sleep face down?
Baby sleeping face down isn’t recommended until after the first birthday. Sometimes people put babies to sleep on their stomachs because it is easier to calm them back to sleep when they are used to sleeping on their stomachs. Sleeping face down increases the risk of sudden infant death syndrome (SIDS).
Will a baby wake up if they can’t breathe?
A baby will not wake up if it can’t breathe. Most of the time, babies are deep sleepers and won’t wake up until morning. Even if a baby doesn’t wake up, it would suffocate or be extremely uncomfortable.
At what age is SIDS no longer a concern?
Concerns about SIDS reduce with each passing week. After 8 months, SIDS (Sudden Infant Death Syndrome) is no longer a concern. The risk of SIDS peaks at 2-4 months, then begins to decline as infants get older, falling dramatically after age 1 year.
Is it OK to let baby sleep on my chest?
Yes, you can let your baby sleep on your chest. This is a great way for them to benefit from the sounds of your heartbeat and breathing while also feeling comforted by physical closeness. But make sure to take a few precautions before laying down with your baby.
Thanks for reading this article on How To Stop Baby Sleeping Face Down and feel free to share this with anyone who could benefit from it. If you have any questions please leave them in the comment section below and we will get back to you as soon as possible.
My Baby Sleeps Face Down in the Mattress, Should I Worry?
We’re supported by moms. When you buy through links on our site, As an Amazon Associate, I may earn a commission.
As a mother of three, I’ve been through three periods of infants wanting to lie on their stomachs instead of on their backs. When a baby sleeps face down, it is a frequent worry.
Common wisdom used to be that babies should always sleep on their stomachs, but studies have linked this practice to SIDS, or sudden infant death syndrome. To protect your baby, know when to permit stomach sleeping and why it is dangerous.
Table of Contents
1 Put Babies On Their Backs
2 Understand the Dangers
2.1 Pockets of Carbon Dioxide
2.2 Developmental Abnormality
3 Know the Facts About SIDS
4 When to Start Stomach Sleeping
4. 1 Understand Your Baby’s Development
4.2 Rolling Over
5 Supervise Tummy Time
6 Changing Views with Changing Times
7 Products That Can Help
7.1 Sleep Sacks and Swaddling Blankets
7.2 Firm Sleep Surfaces
7.3 Breathing Monitors
8 Safe Sleeping Habits
9 Perceived Dangers of Back Sleeping
Put Babies On Their Backs
Always put babies to sleep on their backs. Even if they are old enough to roll over, and even if they do so during their sleep, start them out on their backs. Remember the slogan that back is best. If they wriggle onto their sides as they grow stronger, babies can safely be left in this position. But stomach sleeping, particularly initially, runs the risk of suffocation and SIDS.
View in gallery
Understand the Dangers
Pockets of Carbon Dioxide
When babies do not have experience with stomach sleeping, there is one risk that stands out more than others. They exhale carbon dioxide into the space in which their faces rest and cannot take in oxygen. Experienced babies lift their heads and turn them, while babies who are new to stomach sleeping lift their heads up and put them right back down into the carbon dioxide. Without oxygen, they suffocate. This tragedy can be prevented with precaution and care.
Developmental Abnormality
International research has revealed an abnormality that is found particularly often in boys and in premature babies that is linked to SIDS. This problem lies in the brain’s control of the movement of the head and neck as well as the body’s response to being deprived of oxygen. In the presence of this abnormality, there is a greater likelihood of SIDS occurring, according to Science Daily.
Know the Facts About SIDS
SIDS has been found as the number one cause of death for babies between the ages of one month and one year old. This adds up to about 3,500 infants dying suddenly in their sleep in the United States each year. More boys die from SIDS than do girls. About 75% of infants dying unexpectedly and suddenly do so while sleeping on the same furniture as someone else. This includes couches, armchairs, and beds. While SIDS is not identical to suffocation, both can occur during a baby’s sleep time; this is why it is often called crib death. The National Institutes of Health describe SIDS as a silent, sudden medical disorder that can occur in an infant who seems otherwise healthy.
View in gallery
When to Start Stomach Sleeping
From my own experience, stomach sleeping babies are inevitable. Some sleep comfortably on their backs from the first, but even those will eventually start to roll over. The key to when to permit this is that the older the baby is, the better. Older babies are more likely to lift their faces rather than letting them be pressed dangerously into their mattresses.
Understand Your Baby’s Development
Every baby’s development is distinct. Watch while your baby sleeps, especially during stomach time. When infants can move their heads from side to side, you can safely leave your baby slumbering. If a baby is lying truly face down, with the face pressed into the mattress, there is a problem.
Rolling Over
Babies should be able to roll over and have strong necks to turn their heads. These abilities can be encouraged through waking tummy time, which should start at about two months according to doctors. Safe is always better than sorry.
Supervise Tummy Time
Whether waking or sleeping, keep an eye on tummy time at first. Watch your baby’s developing strength and abilities. SIDS has been frequently linked to a baby having little experience in sleeping stomach down, according to researchers in St. Louis at Washington University’s School of Medicine.
The first several times babies accustomed to sleeping on their backs or sides move to the prone, or face down, position, they are 19 times more likely to suffer from SIDS. Studied infants with catheters taped beneath their noses to monitor levels of carbon dioxide showed the infant’s rebreathing exhaled air. All babies woke up after a span of about five minutes to try and reach air that was fresher. The experienced infants turned their heads from the stale air. Inexperienced infants nuzzled their bedding or bobbed their heads briefly up, returning them straight down into the problem area.
View in gallery
Changing Views with Changing Times
Bad advice pertaining to baby sleep can be dangerous. Many inexperienced parents look to family and friends for information about everything from feeding to diaper rashes, and sleeping styles fall into the spread of potential misinformation. Before the mid-1990s, experts widely preached stomach sleeping. The campaign of Back to Sleep, led by the National Institute of Health to encourage parents to put infants down for bedtime on their backs, reduced sleep deaths by 2,000 fatalities in just five years. While back sleeping has not solved SIDS, as CNN points out, fewer than half of parents follow the ABC guide to safe sleep: sleeping Alone, with babies on their Backs, in Cribs.
Products That Can Help
Some products can help ensure that your baby does not move to sleeping supine, or on the back; others ensure that even on their stomachs, babies sleep safely. Each can be used in turn during different stages of the baby’s development. I used all three, at the appropriate times, to make sure my babies slept safe and sound.
Sleep Sacks and Swaddling Blankets
A swaddled baby does not toss, turn, or roll over. Swaddling should be done so that the baby is not so snug that the hips can’t move. The baby should also be able to breathe freely when swaddled. When babies start to try to turn over, it is time to take away the sleep sack or blankets for swaddling.
View in gallery
Firm Sleep Surfaces
A firm mattress should meet the standards set forth by the CPSC, or the Consumer Product Safety Commission. Firmness will prevent the baby’s face from forming a depression when the head presses into the mattress. When the baby lies on it, a sufficiently firm mattress will not indent.
Breathing Monitors
A baby monitor that monitors the infant’s breathing is helpful when the baby starts stomach sleeping and you want to be sure of safety. Provided that your baby has begun rolling over and has a strong neck, this kind of monitor gives you peace of mind even when other tasks call your attention away. This is no replacement for keeping a personal eye on things, but it can help when you have other children to attend to and cannot be personally present every moment.
We recommend the Sense-U Baby Monitor for tracking your baby’s breathing, rollover, and temperature. There are several other brands available on the market but the Sense-U has the most reviews and is generally seen as the best option available at the moment. View in gallery
Safe Sleeping Habits
After putting the baby to sleep on their back on a firm surface, there are other safe sleeping tips to follow. Never put a baby down for a nap on a sofa, armchair, or adult’s bed. Only use a crib. Share sleeping areas until the baby is six months old. You will be more alert to trouble this way. Only bring the baby into your bed for comfort or to feed; when you are ready to sleep, back into the crib with the baby. Keep soft objects like stuffed toys or loose bedding out of the sleeping area for the baby. Pillows, bumper pads, and quilts are included in this category. They increase the risk of suffocation, strangulation, and entrapment, as stated by healthychildren.org.
Perceived Dangers of Back Sleeping
Some people fear the risk of plagiocephaly or a head that is oddly shaped or flat, in babies that sleep on their backs. While babies do have softer skulls at birth, this shaping is normally and generally goes away on its own. One way to prevent this, while laying babies on their backs, is to place things outside the crib that are bright or interesting, and move the object around so that babies change the positions of their heads. Do not hang mobiles directly over infants, but to the sides, so that they turn their heads to look, according to healthline.
Choking is another fear of new parents when it comes to back sleeping. The fact is, according to the NIH, back sleeping gives a lower risk for choking to babies. They can clear their airways more effectively while sleeping in a supine position. Healthy babies naturally cough up or swallow fluids. In the back sleeping position, the baby’s trachea, or tube that runs to the lungs, lies atop the esophagus, or tube that runs to the stomach. Anything regurgitated from the stomach would have to work against gravity to gain access to the trachea.
When a baby sleeps face down, there are several factors to keep in mind and risks to be aware of. Suffocation and SIDS are both dangers to watch for. However, with the right practices and equipment, you do not need to worry about such perilous consequences.
Lorie Anderson, M.S.Ed.
Hello, my name is Lorie and I’m a mother of three beautiful kids. I have a masters of science in education, learning design, and technology. I like to share my experiences from raising 3 kids and review products I’ve found useful.
Baby sleeping on stomach, face down
Question:
Hello! Son is 2 months old. Sleeping face down on the mattress. I shifted it, and he shoved it off and lay down again face down. He does not sleep on his back at home. Only on the stomach or on the side. Recently, even the side turns over like this. And terribly creepy. God forbid she suffocates… Evgeniya
______
Dear readers! We continue to accept questions on the Azbuka Zdorovya forum.
Hello. Not many parents are aware of the danger of SIDS (Sudden Infant Mortality Syndrome) and the need for proper and safe organization of a child’s bed.
The child must be placed on their back. Most children calm down more easily and quickly when lying on their side or on their stomach, after falling asleep they still need to be transferred to the supine position. Babies under the age of 4 months have the most sound sleep within 20 minutes after falling asleep, it is advisable to do this during this time interval.
It is also important to note that the child’s crib (if the child sleeps in a separate crib) must not contain a blanket , soft bumpers, toys and other fabrics that the baby may inadvertently draw to the face. The mattress should be firm, the sheet stretched. To ensure a comfortable temperature regime, it is important to control the air temperature in the room, dress the baby according to the temperature.
Quite effective swaddling, swaddled babies calm down more easily and do not wake themselves up with their hands. For swaddling, there are currently cocoon diapers in different designs, sleeping bags are intended for older babies, the child feels comfortable in it, and there is no risk that he will throw off the blanket and freeze. If the baby still continues to roll over on his stomach, try using a cocoon-shaped mattress (like Cocoonababy), in which the baby sleeps in a supine position. The side lying position is still preferable to the prone position.
Author: Pediatrician Solovieva E.A.
You can express your gratitude to the doctor in the comments, as well as in the Donations section.
Attention: this doctor’s answer is for informational purposes only. Does not replace face-to-face consultation with a doctor. Self-medication with drugs is not allowed.
Please note that the information provided on the site is for informational and educational purposes and is not intended for self-diagnosis and self-treatment. The choice and prescription of drugs, methods of treatment, as well as control over their use can only be carried out by the attending physician. Be sure to consult with a specialist.
4 thousand 0
0
Doctor
Why does the child sleep on all fours? | Eternal questions | Question-Answer
Estimated reading time: 3 minutes
88749
AiF. Health #5. Unemployment shortens men’s lives 01/30/2014
Category:
Children
Q&A from the newspaper:
AiF. Health №5 30/01/2014
Why does the baby sleep on all fours?
Reply pediatrician, doctor of medical sciences, professor Lev Khakhalin :
We are talking about the usual, favorite sleeping position, right? If the child is healthy, sleeps deeply for 3-4 hours in a row, does not scream, does not cry, does not spin – everything is in order with him. Protruding ass, many healthy children, boys and girls, sleep on all fours, I got the impression that this is typical for large children.
In general, a healthy baby sleeps in a variety of positions. And usually pediatricians brush aside questions like yours, they say, what trifles bother parents! However, child psychologists consider such questions to be far from trifling and even undertake to interpret these postures. And although I am not convinced of the correctness of their interpretations, try to look at your son’s usual sleeping position through the eyes of these psychologists.
So, while the baby was sleeping on his stomach, he demonstrated his subordination to circumstances, lack of confidence in his abilities, his dependence on you. From the point of view of pediatricians, this is a good pose, it helps the proper development of the hip joints, warms and massages the tummy. For some children, sleeping in this position becomes a favorite for years.
Over time, such children begin to sleep on their side, psychologists believe that sleeping in this position is a sign of appeasement and subordination, complaisance of character.
All babies spit up. Some babies spit up more than others, or at certain times.
Typically, babies spit up after they gulp down some air with breastmilk or formula. A baby’s stomach is small and can’t hold a lot, after all. Milk and air can fill it up quickly.
With a full stomach, any change in position such as bouncing or sitting up can force the flap between the esophagus (food pipe) and stomach to open. And when that flap (the esophageal sphincter) opens, that’s when some of what your baby just ate can make a return appearance.
So, what can you do―if anything―to reduce the amount of your baby’s spit up? How do you know if your baby’s symptoms are part of a larger problem? Read on to learn more.
Common concerns parents have about spit up
My baby spits up a little after most feedings.
Possible cause:
Gastroesophageal reflux (normal if mild)
Action to take: None. The spitting up will grow less frequent and stop as your baby’s muscles mature—especially that flap we talked about earlier. It often just takes time.
My baby gulps their feedings and seems to have a lot of gas.
Possible cause: Aerophagia (swallowing more air than usual)
Action to take: Make sure your baby is positioned properly during feeds. Also be sure to burp the baby during and after feeds. Consider trying a different bottle to decrease your baby’s ability to suck in air.
My baby spits up when you bounce them or play with them after meals.
My baby’s spitting up has changed to vomiting with muscle contractions that occur after every feeding. The vomit shoots out with force.
I found blood in my baby’s spit-up or vomit.
Possible cause: Swelling of the esophagus or stomach (esophagitis or gastritis), or another health problem that requires diagnosis and treatment.
Action to take: Call you pediatrician right away so they can examine your baby.
Remedies for spitty babies
Regardless of whether or not your baby’s spit up warrants watchful waiting or medical intervention, there are some simple feeding suggestions that can help you deal with the situation at hand.
5 tips to reduce your baby’s spit up
Avoid overfeeding. Like a gas tank, fill baby’s stomach it too full (or too fast) and it’s going to spurt right back out at you. To help reduce the likelihood of overfeeding, feed your baby smaller amounts more frequently.
Burp your baby more frequently. Extra gas in your baby’s stomach has a way of stirring up trouble. As gas bubbles escape, they have an annoying tendency to bring the rest of the stomach’s contents up with them. To minimize the chances of this happening, burp not only after, but also during meals.
Limit active play after meals and hold your baby upright. Pressing on a baby’s belly right after eating can up the odds that anything in their stomach will be forced into action. While
tummy time is important for babies, postponing it for a while after meals can serve as an easy and effective avoidance technique.
Consider the formula. If your baby is
formula feeding, there’s a possibility that their formula could be contributing to their spitting up. While some babies simply seem to fare better with one formula over another without having a true
allergy or intolerance, an estimated 5% of babies are genuinely unable to handle the proteins found in milk or soy formula―a condition called Cow Milk Protein Intolerance/Allery (CMPI and CMPA). In either case, spitting up may serve as one of several cues your baby may give you that it’s time to discuss alternative formulas with your pediatrician. If your baby does have a true intolerance, a 1- or 2-week trial of hypoallergenic (hydrolyzed) formula designed to be better tolerated might be recommended by your baby’s provider.
If breastfeeding, consider your diet. Cow’s milk and soy in your diet can worsen spit up in infants with Cow Milk Protein Intolerance/Allergy (CMPI and CMPA). Removing these proteins can help to reduce or eliminate spit up.
Try a little oatmeal. Giving babies cereal before 6 months is generally not recommended—with one possible exception. Babies and children with dysphagia or reflux, for example, may need their food to be thicker in order to swallow safely or reduce reflux. In response to concerns over
arsenic in rice, the American Academy of Pediatrics (AAP) now recommends parents of children with these conditions use of oatmeal instead of rice cereal. See
Oatmeal: The Safer Alternative for Infants & Children Who Need Thicker Food for more information.
Vomit vs. spit up: what’s the difference?
There is a big difference between vomiting and spitting up:
Vomiting is the forceful throwing up of stomach contents through the mouth. This typically involves using the abdominal muscles and is often uncomfortable, leaving you with a crying child.
Spitting up is the easy flow of stomach contents out of the mouth, frequently with a burp. Spitting up doesn’t involve forceful muscle contractions, brings up only small amounts of milk, and doesn’t distress your baby or make them uncomfortable.
What causes vomiting?
Vomiting occurs when the abdominal muscles and diaphragm contract vigorously while the stomach is relaxed. This reflex action is triggered by the “vomiting center” in the brain after it has been stimulated by:
Nerves from the stomach and intestine when the gastrointestinal tract is either irritated or swollen by an infection or blockage (as in the stomach bug)
Chemicals in the blood such as drugs
Psychological stimuli from disturbing sights or smells
Stimuli from the middle ear (as in vomiting caused by motion sickness)
Always contact your pediatrician if your baby vomits forcefully after every feeding or if there is ever blood in your baby’s vomit.
Remember
The best way to reduce spit up is to feed your baby before they get very hungry. Gently burp your baby when they take breaks during feedings. Limit active play after meals and hold your baby in an upright position for at least 20 minutes. Always closely supervise your baby during this time.
More information
How to Keep Your Sleeping Baby Safe: AAP Policy Explained
Alejandro Velez, MD, FAAP is a second-year gastroenterology fellow at Cincinnati Children’s Hospital who is interested in practicing general gastroenterology with a focus in motility and functional GI disorders, has a love for medical education at all levels, and harbors a passion for supporting and uplifting those that identify as unrepresented minorities in medicine.
About Dr. Waasdorp
Christine Waasdorp Hurtado, MD, MSCS, FAAP is a member of the American Academy of Pediatrics and the North American Society of Pediatric Gastroenterology Hepatology and Nutrition. She is an Associate Professor of Pediatrics at the University of Colorado School of Medicine and practices in Colorado Springs.
The information contained on this Web site should not be used as a substitute for the medical care and advice of your pediatrician. There may be variations in treatment that your pediatrician may recommend based on individual facts and circumstances.
Tell the Difference Between Baby Spit-up or Vomit
One’s normal, one’s not—which is which? Get the lowdown on spit-up
Your baby just spit up. Or maybe vomited. You’re not sure which it was or whether you should be worried. Baby spit-up isn’t usually an issue.
Also known as reflux, spit-up is simply the flow of food from your little one’s stomach to their mouth.
It’s common, not painful, and might happen from time to time until your baby is about a year old. Baby spit-up is often just the result of a still-developing digestive system or overfeeding.
The difference between spit-up and vomit is outlined below. If you have further questions or concerns, contact your healthcare provider.
What is spit-up?
Spitting up is a common occurrence in healthy infants early in life. This is partly because of immaturity of their digestive system. It’s relatively harmless and usually resolves as the digestive system matures, when your baby reaches 12 to 14 months of age.
Spit-up is sometimes called by other terms like “regurgitation” and “gastroesophageal reflux.” They’re just fancier ways of saying spit-up, with a minor difference. Regurgitation and reflux refer to the backwards movement of the stomach (gastric) contents up into the esophagus—and at times into the mouth. When the contents of your baby’s tummy spill out of their mouth, it’s called spit-up.
Why do babies spit up?
At birth, your baby’s tummy is about the size of a small marble. After 3 days, it is about the size of a ping-pong ball, but still can’t hold much.1 Until they are about 4 months old, most babies’ tummies can hold only small amounts of milk at a time. Too much milk during feedings can cause your baby to spit up or be fussy.
Babies also have less developed muscles in the upper esophagus, which makes it easier for fluids to flow back up from the stomach.
Spitting up can also happen when your baby burps (called a wet burp) or swallows too much air. It isn’t painful to your baby, and most babies don’t even realize they have done it.
As long as your baby is healthy and gaining weight, spit-up should be seen as just a normal part of infancy.
How much spit-up is normal?
It may look like a lot when it’s on your shirt, but the amount of liquid your baby spits up isn’t as much as you think. Usually, it’s just 1 or 2 tablespoons at a time. If your baby spits up more than this—or if their spitting up is the effect of respiratory events like choking, coughing, or wheezing—ask your pediatrician if there is a reason to be concerned.
How can you lessen spit-up?
To help your baby spit up less often, here are a few things you can try:
Hold baby in a more upright position while feeding
Burp baby after every 1 to 2 ounces while feeding
If you bottle-feed your baby, make sure the hole in the bottle’s nipple is not too large. If milk drips out when you turn the bottle upside down, replace the nipple with a smaller one
Keep your baby upright after eating. Laying them flat on a full stomach can lead to spit-up
Avoid too much activity for your baby immediately after eating
Feed your baby less food, but more often
How much and how often to formula feed
Your newborn will probably be hungry 6 to 10 times in a 24-hour period. As a baby grows, so does their stomach, so your baby should begin to eat more at each feeding and eat less often, as the chart below shows.
Number and volume of feedings during the first year
2-4
Age
Average number of feedings per day
Average amount per feeding
Birth to 1 week
6–10
2-3 fl oz
1 week to 1 month
7–8
2-4 fl oz
1 to 3 months
5–6
4-5 fl oz
3 to 6 months
4–5
6-7 fl oz
6 to 9 months
3–4
7-8 fl oz
9 to 12 months
3
7-8 fl oz
The best way to feed your baby is to allow them to take as much as they seem to need. If your baby’s fussy and has not been fed in more than 2 hours, it is probably time for a feeding.
How is baby spit-up different than vomit?
When spitting up begins to make your baby uncomfortable, and more liquid than usual comes up with greater force, this is probably vomit. When a baby vomits more than once, it’s usually caused by a virus. Viruses usually aren’t dangerous, but they can cause your little one to get dehydrated. If your baby is less than 1 year of age, they are at more risk for dehydration. Consult your healthcare professional immediately if you think your baby might be dehydrated.
How can you tell if your baby is dehydrated, and how can you help?
When your baby has a sudden bout of vomiting along with diarrhea, it usually means they have a virus. A virus usually isn’t dangerous, but it can lead to dehydration, which can be a serious problem. It’s important to know these signs of dehydration in your baby:
Fewer wet diapers than normal
Seems very tired or weak
Has tearless, sunken eyes
Has dry skin and little saliva
The younger your baby, the more concerned you should be about dehydration. There are things you can do to help when your baby is ill. Replace the fluids your baby is losing by giving them small, frequent feedings. In some cases, an oral rehydration solution such as Pedialyte® may be recommended. Check with your healthcare provider for advice.
When should you be worried about your baby vomiting?
Although it can be alarming, an occasional vomiting episode is usually nothing to worry about. However, if your baby vomits often, this can be a sign of reflux disease, intestinal obstruction, infection, or a protein allergy. Get in touch with your pediatrician if your baby’s usual spit-up:
Increases in amount or force
Causes choking or respiratory difficulty like wheezing or coughing
Leads to other issues including discomfort, fussiness, poor weight gain, or weight loss
Is accompanied by a fever, diarrhea, bloody mucus, or a bloated tummy
Is green
Is “projectile,” meaning very sudden and with great force
Repeated vomiting in babies between 2 weeks and 4 months of age can be a sign of a blockage at the stomach. Contact your healthcare professional if your baby vomits repeatedly.
Would switching baby formulas help with baby’s tummy troubles?
Consult your pediatrician before changing your baby’s formula.
Similac® offers several easy-to-digest formulas designed to be gentle on your baby’s tummy. For help choosing a formula, check out our Tummy Trouble Tool.
Questions about formula feeding? See our Frequently Asked Questions.
References: 1. Spangler AK, et al. J Hum Lact. 2008;24(2):199-205. 2. Behrman RE, et al. Nelson Textbook of Pediatrics. 16th ed. Philadelphia: WB Saunders Co; 2000:165. 3. Samour PQ, et al. Handbook of Pediatric Nutrition. 3rd ed. Sudbury, MA: Jones and Bartlett Publishers; 2005:90. 4. Fomon SJ. Infant Nutrition. 2nd ed. Philadelphia: WB Saunders Co; 1974:24.
Join Similac® Rewards for up to $400* in benefits and support throughout your journey. * Offers may vary.
Sign Up
Why Tummy Time Is so Important for Babies
Development,Parenting,Most Recent
February 05, 2020
So you just left the hospital overwhelmed with new information on how to best care for your new baby. As you get accustomed to your child’s immediate needs — meals, changing diapers, learning to safely strap them into their car seat — it is easy to forget the importance of early initiation of tummy time.
As pediatric physical therapists, some of the most common questions we receive from parents are “When should we start tummy time?” and “How much time should my child spend on their tummy?” We also hear “My child hates tummy time. What should I do?” If you also have felt this way, you are not alone.
What Is Tummy Time?
Tummy time is a term used to describe the action of placing your baby on their stomach when they are awake and being supervised. Your infant should never participate in tummy time when they are asleep or unsupervised. Infants should sleep positioned on their backs to prevent what is known as sudden infant death syndrome (SIDS).
Remember this helpful phrase: “Back to sleep, tummy to play.”
Why Is It Important?
Tummy time is essential for developing neck muscle strength and control, as well as stability within the shoulder girdles. Positioning your child on their stomach allows them to gain the strength and coordination they need for future motor skills like rolling, sitting, crawling and walking.
Delayed onset of developmental milestones has been associated with a lack of tummy time. It fosters visual-motor development, cognitive functioning and oral-motor skills important for feeding and speech development. Tummy time is the most important method to prevent conditions frequently seen with children who spend sustained periods of time on their back such as torticollis and abnormal skull/facial shaping (plagiocephaly and hemihypoplasia). It also allows for appropriate jaw development.
When Should I Start?
You can start tummy time when your child is as young as one week old. The best way to initiate this is by laying your child on your chest when you are in a reclined position. This allows them to adjust to tummy time in an environment where they feel safe. As they do so, you can recline further until you are lying on your back and they are on their stomach. As soon as possible, transition to tummy time positioned on a firm surface, such as a mat on the floor.
How Much Time on Their Tummy?
The first tummy time sessions can last for only a few minutes, depending on your child’s tolerance. Work up to 80 cumulative minutes a day by the time they are three months old. The more, the better!
What if They Hate It?
Begin slowly and be persistent, even if they don’t appear to enjoy it. Start with what they are able to tolerate and gradually add more time. Provide them with reassurance and encouragement. Be aware of the difference between your baby crying because they are angry and crying because they’re distressed. Babies learn early that crying gets them picked up. Consider allowing them to cry for 30 seconds before doing so if it’s an angry cry.
Throughout tummy time, monitor for pain or distress symptoms (abnormal breathing, a change in facial color) and terminate immediately if you notice this behavior. Allow them time to be soothed and reassured prior to resuming.
You may make tummy time easier by doing it with your baby on your chest or positioned over your lap. Visual work helps! Provide a toy for them to interact with. Toys are best positioned within arm’s reach and near their waist. Once they adjust to tummy time while on your chest or lap, you may progress to positioning them on a blanket on the floor. You also can roll up a blanket and place under their chest to provide additional support.
What if They Have Reflux?
Many infants who experience reflux (frequently spitting up after feeding) have a poor tolerance of tummy time. To improve their comfort level, we recommend waiting at least 30 minutes after their feeding to position them on their tummy. It is helpful to gradually transition them to their stomach by allowing them to play while positioned on their back. After a few minutes, gradually roll them to their side (preferably the left). Allow them to play in that position for a few minutes before helping them roll to play while on their stomach.
Be encouraged that despite any chaos you may feel as an early parent, you are doing a great job! As therapists, we repeatedly observe that once a child adjusts to tummy-time positioning, it becomes their preferred position for play.
Be brave and be focused. You can do it!
Are You Interested in Learning More?
Sign up for our e-newsletter for more tips and best practices from pediatricians.
Sign Up Here
Preventive measures against regurgitation in children
08.03.2017
Regurgitation is the spontaneous reflux of gastric contents into the esophagus and mouth. This condition is not uncommon in infants and is often a cause for concern for parents. The frequency of regurgitation syndrome in children of the first year of life is 18-50%: up to 4 months – 67%, up to 6 months 24%, up to 1 year 5%. In most cases, regurgitation is “benign” and disappears on its own after 12-18 months. At the same time, “benign” or physiological regurgitation characterizes:
the age of the child is up to 12 months;
spitting up 2 or more times a day for 3 or more weeks;
sufficient weight gain;
The child has no signs of metabolic disorders, diseases of the gastrointestinal tract or the central nervous system. The child does not experience difficulty in swallowing or feeding, there is no forced position of the body.
Do not confuse regurgitation with vomiting. When a child burps, the abdominal muscles do not tense up. With vomiting, on the contrary, muscle tension occurs and food is ejected by pressure not only through the mouth, but also through the nose. In some cases, there may be general anxiety, pallor, cold extremities. Often with vomiting, the temperature rises, loose stools appear, which is a sign of an infectious disease. Vomit may contain unchanged milk, mucus, blood or bile.
What explains physiological regurgitation
What is the tendency of babies to spit up? This phenomenon is explained by the peculiarity of the structure of the gastrointestinal tract of young children. At the age of one year, the esophagus is shorter and wider, physiological narrowing is weakly expressed. The stomach is located horizontally, its capacity is small, and the muscles that close the entrance to the stomach and prevent the contents from being thrown back into the esophagus are poorly developed. As the child begins to walk, the axis of the stomach becomes more vertical. The capacity of the stomach increases by the year from 30-35 ml to 250-300 ml. The secretory apparatus matures, the work of the closing muscles (sphincters) improves, which leads to a gradual decrease in the frequency and disappearance of regurgitation. These features explain the predisposition of young children to regurgitation and even the inevitability of this condition. However, there are measures to help reduce the frequency of regurgitation.
Factors contributing to physiological regurgitation include:
Overfeeding. As a rule, actively sucking babies begin to suffer from overfeeding, with abundant milk secretion, as well as when switching to artificial or mixed feeding with an incorrect calculation of the required amount of milk formula. Regurgitation appears immediately or some time after feeding in the amount of 5-10 ml. Milk can flow out unchanged or curdled.
Swallowing air during feeding (aerophagia). A similar situation arises if the child suckles greedily at the breast, and the mother’s milk is not very plentiful; due to the retracted, flat nipple of the mother’s breast, since the child fails to fully capture the nipple and areola; with artificial feeding, if the hole at the nipple of the bottle is large enough or the nipple is not completely filled with milk. Babies with aerophagia often experience anxiety after feeding, bulging of the abdominal wall (belly inflates). After 10-15 minutes, the swallowed milk flows out unchanged, which is accompanied by a loud sound of air eructation.
Intestinal colic or constipation. These conditions lead to an increase in pressure in the abdominal cavity and a violation of the movement of food through the gastrointestinal tract, causing regurgitation.
Until the child is four months old, spitting up up to two teaspoons of milk after feeding, or one spitting up of more than three spoons during the day, is considered the norm. You can check the amount of spitting up in the following way: take a diaper, pour one teaspoon of water on its surface, and then compare this spot with the spot formed after the next spitting up.
Pathological regurgitation may be due to:
surgical diseases and malformations of the digestive system;
diaphragmatic hernia;
pathology of the central nervous system, trauma of the cervical spine during childbirth;
food intolerance, lactase deficiency;
increased intracranial pressure.
Such regurgitation is characterized by intensity, systematicity, the child spits up a large amount of milk. At the same time, there is a violation of the general condition of the baby – the child is whiny, loses or does not gain weight, cannot eat the amount of food necessary for his age. In such a situation, a pediatrician, gastroenterologist, surgeon, allergist, neurologist should be examined. It also requires examination and exclusion of anomalies in the structure of the upper gastrointestinal tract, the preservation of regurgitation for more than 1 year.
Scale for assessing the intensity of regurgitation:
Less than 5 regurgitations per day with a volume of not more than 3 ml – 1 point.
More than 5 regurgitations per day with a volume of more than 3 ml – 2 points.
More than 5 regurgitations per day up to half the amount of formula or breast milk, not more often than in half of the feedings – 3 points.
Spitting up a small amount of milk for 30 minutes or more after each feeding – 4 points.
Regurgitation from half to full volume of formula or breast milk in at least half of the feedings – 5 points.
Regurgitation with an intensity of 3 or more points requires a visit to a doctor.
Preventive measures against regurgitation in children
If regurgitation is physiological in nature, then it is not worth treating or correcting in this case. It is necessary to deal with the elimination of the cause, if possible, and carry out prevention.
Prevention of regurgitation in children includes the following measures:
Postural therapy: when feeding, it is necessary to hold the baby at an angle of 45 °, make sure that he completely grasps the nipple with the areola; after feeding, hold the baby in an upright position (“column”) for 20 minutes – to drain the swallowed air. Due to this, the air that has entered the stomach will be able to go out. If nothing happened, then put the baby down and after a minute or two, lift him upright again.
Make sure that the opening in the bottle is not too large and that the nipple is filled with milk. Experiment with nipples – perhaps the other will be better. Milk should come out in drops, not a trickle.
Before you start feeding your baby, lay him belly down on a solid base.
After feeding, try to minimize the baby’s physical activity, do not disturb him unnecessarily, and change clothes only if there is an emergency.
Avoid squeezing diapers or clothes on the abdomen of the child.
If the baby’s appetite is good, then it is better to feed him often, but in small portions, otherwise, due to the large amount of food, the stomach may overflow, and this, as a result, leads to regurgitation of excess food.
The surface in the bed on which the baby lies should rise 10 cm at the head.
In addition, it is possible to use special “thickeners” of milk or anti-reflux mixtures, which the doctor will help you choose.
In the event that regurgitation begins to become more frequent or becomes abundant, or first began after six months of the baby’s life, or does not subside by one and a half to two years of life, the child should be consulted by a pediatrician. With a high probability, additional help from a gastroenterologist will be needed.
In our Family Medical Center you can always find highly professional help.
← Back to the list of articles
Why does the baby spit up after feeding?
Search Support Icon
Search Keywords
Regurgitation is a common condition in newborns and infants and is most often a normal variant. However, it is not uncommon for parents to worry if their baby is spitting up frequently, believing that it is due to nutritional or health problems in general. Sometimes these fears are not unfounded, and regurgitation really has a pathological origin. What is its cause and when should you really consult a doctor about this?
Regurgitation – Return of a small amount of food (uncurdled or partially curdled milk) from the stomach up the digestive tract: into the esophagus and further into the oral cavity. According to statistics, at least 1 time during the day can spit up at least 50% of babies from 0 to 3 months, more than 60% of children 3-4 months, and 5% of children spit up until the year 1 .
Regurgitation in newborns is considered a physiological process. It is caused by a number of factors, including:
Features of the structure of the upper digestive tract in babies
In newborns and infants up to a year of age, the stomach has a spherical shape. It holds a small amount of food, besides, the release from it into the duodenum is slower in comparison with children after the year 2 .
Weakness of the lower esophageal sphincter that separates the esophagus from the stomach
Normally, the lower esophageal sphincter should tightly “close” the esophagus, allowing food to pass into the stomach and not allowing it to enter back into the upper digestive tract. However, in young children (up to a year), the muscles of the esophageal sphincter are poorly developed, and it does not do its job very well 2 .
Slow movement of food through the gastrointestinal tract
The neuromuscular system of newborns is immature. It does not ensure the proper movement of food through the esophagus, causing regurgitation.
One of the important risk factors contributing to regurgitation in newborns is aerophagia. This is the swallowing of large amounts of air during feedings. This happens when the baby is not properly attached to the breast, the mother has a lack of breast milk, or the bottle is in the wrong position in the child who receives the mixture. The size of the opening in the nipple also matters – if it is too large, the newborn swallows a lot of air 3 .
With aerophagia, the baby becomes capricious, restless immediately after feeding. Noticeable bloating. If the baby spits up immediately after a feed, the milk (or formula) remains practically fresh, uncurdled 3 .
Promotes post-feeding regurgitation and baby’s predominantly horizontal position during the day, combined with relatively high intra-abdominal pressure 4 . Therefore, the correct position of the baby after feeding is so important. To avoid regurgitation of an excessive amount of stomach contents, after feeding, it is necessary to hold the baby in an upright “column” position for some time (10-20 minutes), lightly patting on the back and allowing excess air to “exit”.
Regurgitation in many newborns can be provoked by other situations in which pressure in the abdominal cavity increases and stomach contents are thrown into the esophagus, in particular 3 :
tight swaddling;
stool disorders, in particular constipation;
long, forced cry and some others.
Want to avoid common feeding problems?
Start with a baby bottle with an anti-colic system that helps avoid common feeding problems such as colic, gas and spitting up*
How can you tell the difference between normal spitting up and vomiting?
Sometimes regurgitation is considered a manifestation of disorders in the digestive tract of children. Due to the constant reflux of acidic stomach contents into the upper sections, inflammation and other complications may develop, including growth retardation, a decrease in hemoglobin levels, and others. Therefore, it is important for parents to understand where the line is between physiological and pathological regurgitation 1 .
If the mother is worried that her baby is spitting up, keep track of when this happens and count the total number of spit ups per day. Normally, regurgitation usually occurs after eating (the child burps after each feeding), lasts no more than 20 seconds and repeats no more than 20-30 times a day. With pathology, the problem manifests itself at any time of the day, regardless of when the baby was fed. Their number can reach 50 per day, and sometimes more 1 .
The amount of discharge during regurgitation also matters. With normal, physiological regurgitation, it is approximately 5 – 30 ml. If this volume fluctuates between 50 and 100 ml, it is already defined as profuse vomiting. When the range of the jet of vomit is up to 50 cm, doctors talk about “vomiting a fountain.” A variant of atonic vomiting is possible, when the contents of the stomach flow “sluggishly”. It occurs with atony of the stomach (decrease in muscle tone of the stomach wall) and disruption of the esophagus 1 .
Vomiting in babies is a warning sign. Doctors are especially alarmed by repeated vomiting, a fountain, with an admixture of bile, in combination with constipation. Vomiting can lead to the development of dehydration, acid-base imbalance and other consequences, therefore, if it occurs, you should urgently contact a pediatrician to find out the cause and begin treatment. A doctor’s consultation is necessary if the child is spitting up a lot (more than 15-30 ml at a time), with a frequency of more than 50 episodes per day 1.3 .
Physiological regurgitation: symptoms
Regurgitation in newborns, which is considered normal and not of concern to pediatricians 3 :
usually lasts for a certain period of time;
is characterized by slow, “passive” outflow; if the baby spits up a fountain, it is better to consult a doctor;
has a sour smell of curdled milk;
occurs without the participation of muscles – the baby does not strain during regurgitation;
does not affect the general well-being of the baby.
How to help a newborn who spit up often?
If the baby is healthy, no medication is prescribed for spitting up. To help the child allow simple measures based on lifestyle changes and feeding.
Frequent feeding of the baby It is known that babies are more prone to spit up if their stomach is full. To improve the situation, it is recommended to feed the baby more often, avoiding oversaturation, best of all – on demand 5 .
Correct feeding technique Every feeding, the mother must ensure that the baby does not swallow too much air during suckling. When sucking, there should be no loud, smacking, clicking sounds. You also need to control that the baby captures the nipple along with the areola.
Choosing the right bottle and nipple If the newborn is bottle-fed and receiving formula, it is important to choose the right bottle and nipple. The hole in it should be such that the milk flows out in drops, and not in a stream. The nipple must not be filled with air
New Anti-colic bottle with AirFree valve
The AirFree valve prevents air from entering the baby’s stomach.
Baby standing upright after eating
To allow air that has entered the digestive tract during meals to escape, it is important to hold the newborn upright for 10-20 minutes after feeding 4 .
Ensure the correct position of the baby during sleep
To reduce the negative impact of stomach acid on the esophagus, put your baby to sleep in a supine position. The side or prone position, which many pediatricians used to recommend, is no longer recommended. It was found to be associated with an increased risk of sudden infant death syndrome 5 .
If parents notice alarming symptoms, such as regurgitation that occurs too often or is large in volume, etc., it is important to consult a pediatrician without delay. This will allow you to identify the real problem in time and help the baby grow up healthy and happy.
References
1 Zakharova I. N., Andryukhina E. N. Regurgitation and vomiting syndrome in young children // Pediatric pharmacology, 2010. V. 7. No. 4.
29015 Nagornaya V., Limarenko M. P., Logvinenko N. G. Experience with the use of domperidone in suspension in young children with regurgitation syndrome // Child Health, 2013. No. 5 (48).
3 Zakharova IN Regurgitation and vomiting in children: what to do? //Pediatrics. Supplement to Consilium Medicum, 2009. No. 3. S. 58-67.
4 Zakharova I. N., Sugyan N. G., Pykov M. I. Regurgitation syndrome in young children: diagnosis and correction // Effective pharmacotherapy, 2014. No. 3. P. 18-28.
5 Vandenplas Y. et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) //Journal of pediatric gastroenterology and nutrition. 2009; 49(4): 498-547.
You are leaving the Philips Healthcare (“Philips”) official website. Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
I understand
You are about to visit a Philips global content page
Continue
You are about to visit the Philips USA website.
I understand
why the baby spit up after feeding
If a child spits up after feeding, this is in most cases due to the anatomical immaturity of the upper digestive system. More often than others, premature babies, babies with congenital pathologies suffer from regurgitation. Sometimes the cause is the wrong breastfeeding technique.
Regurgitation in infants is perhaps the most common occurrence in modern pediatrics. More than half of children spit up at least once a day, which is almost always a physiological reaction.
As the baby grows older, spitting up less and less and by 6 months it practically stops doing so. However, sometimes the problem remains, and burping continues for up to a year. In such a situation, you need to make sure that the gastrointestinal tract is functioning normally and consult a doctor.
Why does the baby spit up after every feed
There is a very simple explanation for this. The esophagus of newborns is a funnel with a wide part at the top, and the sphincter at the transition to the stomach actually gapes and hardly retains food.
Normally, after food enters the stomach, the sphincter contracts and prevents it from “returning” into the esophagus. But in this case, when the stomach is full, part of the contents immediately comes out if the baby takes an inclined or horizontal position.
Babies have two more features: increased pressure over the lower esophageal sphincter, as well as a straight and sometimes obtuse angle of His, formed by the side walls of the esophagus and stomach. In adults, this angle is sharp, which also prevents the return of food eaten into the esophagus.
After feeding, do not put the baby on his stomach, it is better to hold him upright in your arms, trying not to put pressure on his chest. But if he still burps, you should not worry, this is a normal process. If in doubt, please contact our doctors. At a remote consultation, they will explain the causes of regurgitation, talk about pathologies. If necessary, they will tell you which specialists to go through.
A few more reasons why a child often spit up
Physiological belching after feeding is due to two factors: swallowing air (aerophagia) and increased intra-abdominal pressure. The first is usually associated with fast and greedy suckling, improper attachment of the baby to the breast, or the wrong position of the bottle when it comes to artificial feeding. An air bubble forms in the stomach, pushing out a small amount of milk or formula.
The same results are obtained by a quick change in the position of the baby’s body after feeding, which will easily burp if it is immediately started to swaddle, shake, bathe or massage. After all, his stomach resembles an open bottle: tilted / turned over – the contents spilled out.
As for the increase in intra-abdominal pressure, it increases with a too tight diaper or tight swaddling, as well as against the background of increased gas formation, intestinal colic or stool retention.
Regurgitation in newborns after feeding may be due to the lack of a feeding regimen and overeating.
Baby burps an hour after feeding: what does it mean
The most common cause is constipation, which increases intra-abdominal pressure. Food moves slowly through the gastrointestinal tract, so the child can burp an hour or two after feeding.
Attention! Delayed regurgitation combined with delayed defecation may be a sign of a lazy stomach. But such a diagnosis should be made by a doctor.
5 causes of regurgitation in newborns after formula feeding
The selection of artificial nutrition is a purely individual process with an unpredictable result. There is no 100% guarantee that the mixture will suit the child, even if the brand is very popular.
Poor digestion of the mixture may well cause not only frequent spitting up, but also other digestive problems, including colic, constipation and allergic reactions. In addition, store-bought baby food has a denser texture than breast milk and lasts longer in the stomach. Therefore, the likelihood of its reverse promotion to the esophagus after feeding is higher.
Your baby may spit up after every feed because:
the proportions of dilution of the mixture are violated;
the feeding regime is not observed;
the transition from breastfeeding to artificial feeding was too abrupt;
the wrong bottle is selected;
allergy.
Improper mixing ratio
Each manufacturer indicates on the packaging of the mixture how much water is required to dilute it, and what volume is suitable for the baby by weight and age. Sometimes mothers mistakenly or intentionally dilute food in a way that is not recommended, and the child eats more than normal. As a result, the surplus, of course, comes out.
Case study:
After 3 months, a breastfed child suddenly began to behave restlessly, sleep poorly, spit up after eating, weight gain became slightly below normal. From a conversation with the mother, the doctor learned that the baby was fed too often, the feeding regimen was not observed. After increasing the intervals between breastfeeding, the regurgitation stopped.
Refusal of night feedings is also undesirable: the daily volume of food is distributed during the daytime, which leads to stomach overload and regurgitation.
Feeding schedule not followed
Unlike natural, artificial feeding involves eating by the hour.
Baby food takes longer to digest, so the recommended interval between feedings is at least 3 hours. If you feed the child more often, he will “give out” the excess back, since the previous portion has not yet been absorbed.
Abrupt transition from breastfeeding to artificial feeding
When changing the diet, the child’s body must first get used to, adapt to the new food. This applies not only to the transition from breastfeeding to artificial feeding, but also from one type of mixture to another.
Wrong bottle selected
This refers to the too wide neck of the container, because of which the child swallows a lot of air along with food. Its discharge will provoke regurgitation after feedings.
Allergy
An allergic reaction to cow’s milk protein causes inflammation of the intestinal wall, which in turn leads to malabsorption. Carbohydrate metabolism worsens, since secondary lactase deficiency occurs against the background of an inflammatory reaction – a decrease in the synthesis of the lactase enzyme.
As a result, sugar is broken down incorrectly, increased gas formation occurs, and the baby spits up a fountain. In addition, the baby may feel discomfort at the beginning of feeding and react with an increase in nervous excitability during the period of increased intestinal motility. This also often leads to belching.
What does curd regurgitation mean
Belching with curdled milk after feeding only indicates that the food was in the stomach for some time and managed to curdle – it was fermented. The reason may be in a change in body position or indicate pyloric stenosis with profuse vomiting with a fountain.
Attention! When spouting against the background of pyloric stenosis, the child spits up profusely, the jet scatters to a distance of half a meter.
What to do
First you need to make sure that you really need to do something. Pediatricians are advised to determine the intensity and frequency of regurgitation on a five-point scale.
Points
Regurgitation frequency
Volume
one
No more than 5 per day
Not more than 3 ml
2
> 5 times a day
> 3 ml
3
> 5 times a day
> 0. 5 volume of food eaten
four
After every feeding
Small amount over 30 minutes or more
5
At least half of the meals are accompanied by regurgitation
> 0.5 volume of food eaten
Now you can determine if there really is a problem. The criteria are:
the baby is not yet a year old;
he spits up 2 times a day for 3 weeks or longer;
before burping there are no precursors, specific signs;
during regurgitation, the tension of the anterior abdominal wall is not felt;
there are no difficulties with swallowing, sucking, the child does not take any specific forced position;
the baby does not begin to sweat a lot, turn pale after burping, and feels normal;
he is active, has a good appetite, and is gaining weight appropriately for his age.
The above points indicate that everything is in order.
If the intensity and frequency of spitting up is 3 points or more, this is a reason to consult a doctor. Our doctors are ready to advise on all issues at any time of the day. At a remote consultation, possible causes will be identified, and a plan of further action will be drawn up.
How parents determine the amount of rejected food
Normal regurgitation after feeding occurs in small volumes, within 1-2 tablespoons. You can determine how much food came out when you burp.
When the child burps into the diaper, you need to pour 1 tbsp nearby. l. water and compare the size of the spots. If they are almost the same, there is no reason to worry.
Alarm symptoms
Medical assistance is necessary if the child spits up a lot after feeding, while crying and acting up. A bad symptom is the requirement of supplementary feeding, that is, the baby remains hungry after he has eaten his portion.
Serious illnesses can present with symptoms such as:
sudden weight loss, weight gain does not meet the standards;
lack of stool;
profuse vomiting with an admixture of bile;
urination less than 8-10 times a day;
continued spitting up after the child is one year old.
How to deal with regurgitation: a step-by-step guide
If the baby is spitting up after feeding breast milk or formula, you can start with a nutritional correction. When breastfeeding, it is important to ensure that the baby completely captures the nipple along with the areola. His lower lip is usually slightly twisted.
Step 1
It is better to feed the baby while sitting, holding the baby at an angle of 45-60 ° to the chest. In this position, the air freely leaves the stomach, due to which the likelihood of reflux of food into the esophagus is reduced. After eating, it is preferable to put it on its side in a crib: this way, when returning from the stomach, the masses will not enter the respiratory tract. If the child burped while lying on his back, you should lift him up and turn him face down.
Step 2
After the baby has eaten, it must be held upright (pose of a soldier) for at least 20 minutes.
Step 3
You can partially remove the air from the stomach before feeding, putting the baby on the stomach for 10-15 minutes. With a tendency to intestinal colic, a light massage of the abdomen, which is done in between meals, will help.
Step 4
Even if the child is constantly spitting up, this is not a reason to transfer him to artificial mixtures. But a clear feeding regimen is desirable after a more or less strict period of time. In addition, mom should follow a hypoallergenic diet and exclude foods that can provoke flatulence – cabbage, legumes, black bread.
Step 5
For artificial babies, it is preferable to use a special anti-colic bottle and a nipple with a special design. The bottle has a valve that prevents you from swallowing air while eating. It is also necessary to make sure that the milk does not flow like a river, but slowly drips, that is, the hole in the nipple must have the appropriate diameter.
Step 6
When buying a mixture for a spitting up baby, it is better to consult a pediatrician. He may recommend a hypoallergenic formula or a formula that does not contain bovine protein. For some children, the so-called anti-reflux mixture is suitable.
Step 7
Normally, complementary foods are introduced from the 4th month of a child’s life, but in the presence of regurgitation, it is allowed to include food thickeners in the diet after the 1st month. It can be mixtures with rice flour, rice porridge without milk. But they are used in an amount of a maximum of 1 tsp. in one feeding.
Step 8
Do not swaddle too tightly, massage, and generally somehow disturb the child after eating. You can only lightly pat him on the back, putting him on his knees, to prevent spitting up.
Step 9
Is the child overeating? To check this, you just need to weigh it before feeding and after. And it does not matter what he eats – mother’s or artificial milk.
FAQ
What symptoms should you call an ambulance for?
+
If, after spitting up, the child does not breathe or has lost consciousness; lips and face take on a bluish tint; reflux – gastric contents – has a green or brownish color, which may indicate intestinal obstruction, gastric bleeding.
Why does a baby spit up breast milk, but formula does not?
+
If everything is in order with the calculation of “doses”, and there is no overfeeding with breast milk, most likely it is lactose intolerance. To clarify the diagnosis, it is necessary to take tests.
Child care is critical to working parents, and Harvard understands that finding the right fit for your family means considering numerous factors. You are encouraged to review the options below to see which one may best meet your needs.
On-Campus Child Care
Off-Campus Group Child Care
In-home Child Care/Babysitters
Nanny Placement Services
Nanny Payment Service
On-Campus Child Care
Allston and Cambridge
Six child care centers operate on Harvard’s Cambridge and Allston campuses. Each center has its own characteristics and culture, so families are encouraged to familiarize themselves with information provided below.
Feel free to contact any center directly, email the executive director of Campus Child Care, or email the Office of Work/Life. For more information on the Massachusetts Department of Early Education and Care, please visit EEC’s website.
Learn more about the on-campus child care centers:
Campus Child Care, Inc. is the independent, nonprofit operator of the child care centers on Harvard’s campuses. To learn more about CCC, please visit their website.
Application and Enrollment information: Read Work/Life’s FAQs for information on the application and enrollment processes and the role of the Harvard affiliation. Read CCC’s FAQs for complementary information on application and enrollment, and for detailed information on center policies.
Application fees: Find answers to questions specifically about application fees
Individual center information: Find contact information, rates, age groups, and schedules and hours. Read about individual centers. Read CCC’s FAQs for information on child care center policies, and life in the centers.
Changes for 2023:
Botanic Gardens Children’s Center will be closed for the summer of 2023 for renovation.
Peabody Terrace Children’s Center (PTCC) will be moving back to its permanent location at 900 Memorial Drive in June 2023.
A new program, Western Avenue Children’s Center (WACC), will be opening at 114 Western Avenue, Allston, when PTCC moves back to Cambridge in June 2023. Applications for that center are being accepted now through the online application (see below). As part of Harvard’s cooperation agreement with the City of Boston, a limited number of spots in this new center will be initially reserved for residents of Allston zip codes 02134 and 02135. In addition, families who reside in these zip codes ― and who are not eligible for any other Harvard scholarship ― may apply for a means-tested child care subsidy. For more information, please email the Harvard Office of Work/Life.
Online application: You can apply to all six centers via a single online application. We encourage you to read about individual centers before applying.
Visiting centers: If you would like to know more about an individual center, please feel free to contact directors.
Harvard Longwood Campus
Affiliates of Harvard Medical School, the Harvard T.H. Chan School of Public Health, and the Harvard School of Dental Medicine and others on the Harvard Longwood Campus may have access to Longwood Collective-managed Longwood Medical Area child care centers.
Off-Campus Group Child Care
High-quality, affordable child care is in high demand in the greater Boston area. The following resources are designed to make your search a little easier. Only you know what child care arrangement will be right for your family. We encourage you to review these and other available resources and to carefully consider the safety and appropriateness of any child care provider or setting.
If you are a benefits-eligible Harvard employee, you may use the free dependent-care resource and referral service available through Harvard’s Employee Assistance Program.
Any member of the general public can get a list of licensed family day care providers and group child care centers in your community, visit the Massachusetts Department of Early Education and Care.
Several nonprofit agencies are members of the Massachusetts Child Care Resource and Referral Network and can help you find child care:
Child Care Choices of Boston serves Boston, Brookline, Cambridge, Chelsea, Somerville, Revere, and Winthrop.
Child Care Circuit serves several towns near Harvard’s campuses including Arlington, Belmont, Medford, Newton, and Watertown, as well as many others.
Community Care for Kids serves Braintree, Cohasset, Dedham, Hull, Milton, Needham, Quincy, Randolph, Wellesley, Weston, and Weymouth.
In-home Child Care/Babysitters
Online search for caregivers through Care.com membership: If you are a benefits-eligible Harvard employee, you have unlimited, free access to Care. com, a self-service online database of caregivers. Visit the HARVie Care.com page to learn about all of the services available through Care @ Work. Only you know what child care arrangement will be right for your family. We encourage you to review these and other available resources and to consider the safety and appropriateness of any child care provider or setting. Care.com offers a safety center which includes a menu of additional background checks that you can purchase to supplement information supplied by caregivers on the digital platform.
Note:You must register before you need it! To use any service provided by Care @ Work, Harvard faculty and staff must first complete and return a waiver. Once the Office of Work/Life receives this waiver, the employee’s name is added to an automatic filed feed that goes to Care.com on a daily basis. Go here for more about what Care @ Work offers and detailed information on how to register.
Nanny Placement Services
Boston Nanny Centre (BNC) provides a range of nanny-placement services to Harvard University affiliate families. BNC nanny-placement services range from comprehensive placement packages to a-la-carte services such as in-depth consultation, thorough background checks, post-hire contract support, and other services. BNC offers Harvard affiliates 10% off any service. You can read more about BNC and their services by visiting their website, reading their description of services and reviewing their price list.
Nanny Payment Service
However you choose a caregiver, nanny or babysitter, you may have payroll and tax responsibilities.
Boston Nanny Centre (BNC) (see above) will refer its clients to firms that can assist with these processes.
In addition, through the Care @ Work benefit, benefits-eligible employees have access to HomePay from Care.com. As with all Care.com services, you must first register. To use any service provided by Care @ Work, all Harvard faculty and staff must first complete and return a waiver. Once the Office of Work/Life receives this waiver, the employee’s name is added to an automatic filed feed that goes to Care. com on a daily basis. Visit the HARVie Care.com page to learn more about services available through Care.com and for detailed instructions on how to register. Once you are pre-registered and have submitted the waiver, you will be directed to Harvard’s Care @ Work portal to register once using your Harvard email address. From there, you will be able to learn more and sign up for HomePay services.
Child Care Services | Child Care and Family Services
Choosing a child care provider is one of the more important decisions you will make for your child. ISU Child Care and Family Services provides expertise and guidance as you explore your child care options. Whether you are looking for information about the types of child care, licensing standards, or quality measures, we are confident we can help.
Request a consultation with a member our team to discuss your child care needs and questions.
Campus Child Care Services
Iowa State University has three campus child care centers, each of which has achieved and maintains the highest levels of quality. These centers are open year-round and care for children six weeks through school-age.
We encourage families to tour and interview many child care programs before making a decision. Use the links below to explore what our campus child centers have to offer!
Child Development Laboratory School
4380 Palmer Building, Ste. 035 | (515) 294-3040
Director: Eileen Canafax
Ages: Infants through preschool
Hours: 7:30am-5:30pm, Monday-Friday
ISU Child Care Center at Veterinary Medicine
1520 Christensen Drive | (515) 294-2273
Director: Angela Adams
Ages: Infants through preschool
Hours: 7:00am-6:00pm, Monday-Friday
University Community Childcare
2623 Bruner Drive | (515) 294-9838
Director: Stacy Lehman
Ages: Infants through school-age
Hours: 7:00am-5:30pm, Monday-Friday
Off-Campus Child Care Services and Resources
Iowa Child Care Resource & Referral
Iowa Child Care Resource & Referral (CCR&R) is a statewide agency that helps parents take the guesswork out of choosing care by providing FREE, non-biased, and customized referrals to local child care providers. Referrals are provided so that parents can look into all of their options and find the child care arrangements that best meet the needs of their family. Parent Referral Specialists are available Monday through Friday, 8:00AM – 4:30PM by calling (855) 244-5301. Families can also conduct their own child care search online 24/7.
Iowa Department of Human Services – Child Care Provider Search
The Iowa Department of Human Services (DHS) is the agency which supervises child care providers in the state of Iowa. On their website, you can search for child care providers in your area, based upon a variety of criteria.
Iowa Department of Human Services – Child Care Compliance Reports
The Iowa Department of Human Services is required to make child care provider compliance and complaint reports to the public.
ISU Student Job Board
The Student Job Board is ideal for part-time jobs in the community and surrounding area.
Care. com
Helps families find child care, senior care, special needs care, tutoring, pet care, housekeeping, etc. Families are able to sign up and search for providers.
College Sitter Contact
Connects families with highly qualified college student child care providers in a safe, convenient, and reliable way. Families are able to sign up and search for providers.
Additional Information
Use the following tools, guides, and checklists to help you make the best decision for your child and your family.
Guide to Choosing Quality Child Care – A detailed guide to Iowa’s child care system from Iowa Child Care Resource & Referral
Starting Your Child Care Search – An overview of the process of choosing a child care provider, published by Child Care Aware of America
Selecting a Child Care Program – Checklists to help you organize information and make the best decision for your child from Child Care Aware of America
Budgeting for Child Care – Tips and tools to help you plan for this major expense, published by Child Care Aware of America
Regional Training and Certification Centers
Regional Training and Certification Centers – CERTIFIED NUNSPERS
Payment completed successfully.
Your order number No. 10010
An email was sent to [email protected] containing links to a full video training course.
If the letter was not delivered, write to us by email: [email protected]
Links to the full video course:
https://www.youtube.com/watch?v=bMQjYGXfKD4
Copy links to clipboard.
Back to site
No.
Subject of the Russian Federation
Organization on the basis of which the center was created
Center address
1
Belgorod region
Association of non-governmental institutions and organizations engaged in educational activities (private kindergartens) and providing child care and development services
308034, Belgorod, st. Shchorsa, 15
2
Vologda region
Regional public organization “Union of social workers” of the Vologda region
162562, Vologda region, settlement Sheskna, st. Labor 7-87
3
Republic of Bashkortostan
ANO “Center for Social Services to the Population “SOCIUM”
452550, Republic of Bashkortostan, Mechetlinsky district, Bolsheustinskoye village, Lenina street, 2
4
Republic of Buryatia
State Autonomous Institution of Additional Professional Education “Buryat Republican Institute of Educational Policy”
670000, Republic of Buryatia, Ulan-Ude, st. Sovetskaya, 30
5
Ulyanovsk region
Regional state budgetary institution of social services “Integrated center of social services for the population” Istok “in Ulyanovsk”
432034, Ulyanovsk, st. Polbina, 45A
6
Khanty-Mansi Autonomous Okrug – Yugra
Municipal autonomous preschool educational institution of the city of Nizhnevartovsk kindergarten No. 41 “Rosinka”
628616, Khanty-Mansiysk Autonomous Okrug-Yugra, Nizhnevartovsk city, Severnaya street, house 9a, building 1
7
Khanty-Mansi Autonomous Okrug – Yugra
English kindergarten «SunSchool» (IP Mustafina O.V)
KhMAO-Yugra, Nizhnevartovsk, Mendeleev house 8A. Photo from June 25, 2019
8
Khabarovsk Territory
Interregional Public Organization “Far Eastern Association of Preschool Organizations” (OO DVADO)
Legal address: 680013, Khabarovsk, st. Leningradskaya 7/109. Actual address: Khabarovsk, st. Dzerzhinskaya 65, of. 302
Home
Login
Input
Authorization
*
*
Remember
Lost your password?
Authorization
Password generation
Regional Training and Certification Centers
Regional Training and Certification Centers – CERTIFIED NUNSPERS
Payment completed successfully.
Your order number No. 10010
An email was sent to [email protected] containing links to a full video training course.
If the letter was not delivered, write to us by email: [email protected]
Full video course links:
https://www.youtube.com/watch?v=bMQjYGXfKD4
Copy links to clipboard.
Back to site
No.
Subject of the Russian Federation
Organization on the basis of which the center was created
Center address
1
Belgorod region
Association of non-governmental institutions and organizations engaged in educational activities (private kindergartens) and providing child care and development services
308034, Belgorod region, city of Belgorod, Shchorsa street, 15
2
Vologda region
Regional public organization “Union of social workers” of the Vologda region (SSR VO)
162562, Vologda region, Sheksna village, Labor street, house 7, apartment 87
3
Vologda region
Charitable Foundation “Assistance”
162600, Vologda region, city of Cherepovets, Sovetsky avenue, building 98, office 49
4
Vologda region
Charitable Foundation “Our Children”
162600, Vologda region, city of Cherepovets, Godovikova street, house 28, apartment 35
5
Vologda region
Limited Liability Company “Service Center “Good Helper”
(LLC TsU “Good Helper”)
162627, Vologda region, city of Cherepovets, Sheksninsky pr-kt, house 16, apartment 270
6
Vologda region
Vologda regional public organization of young disabled people “Areopag”
( VRO OMI “Areopag”)
160000, Vologda region, Vologda city, Zosimovskaya street, 65, office 108
7
Vologda region
ANO Center for Counseling and Family Development “Mama Can”
(ANO “Mama Can”)
160033, Vologda region, city of Vologda, Tekstilshchikov street, house 18 “A”, apartment 36
8
Vologda region
Budgetary social service institution of the Vologda Oblast “Rehabilitation Center for Children and Adolescents with Disabilities “Overcoming”
162616, Vologda region, city of Cherepovets, Yubileynaya street, 47
9
Trans-Baikal Territory
Limited Liability Company “PIFAGOR”
(OOO Pifagor)
672023, Trans-Baikal Territory, city of Chita, Krasnoyarskaya street, house 12
10
Irkutsk region
State Autonomous Institution of Additional Professional Education of the Irkutsk Region “Regional Institute of Personnel Policy and Continuous Professional Education”
(GAU DPO “Regional Institute of Personnel Policy and Continuous Professional Education”)
664510, Irkutsk region, Irkutsk district, Dzerzhinsk village, Sadovaya street, 2
11
Kostroma region
Department of Education and Science of the Kostroma Region
156013, Kostroma region, city of Kostroma, Lenin street, house 20
12
Leningrad region
Committee for General and Vocational Education of the Leningrad Region
191311, Leningrad region, St. Petersburg, Rastrelli street, building 2, “Lit A”
13
Lipetsk region
Private agency for the selection of professional nannies “Manezhik”
398000, Lipetsk region, city of Lipetsk, Lutova street, 18
14
Perm region
Private educational institution of additional professional education “ARSENAL-PROF” (PHOU DPO “ARSENAL-PROF”)
614068, Perm region, city of Perm, Plekhanov street, house 39
15
Republic of Bashkortostan
Autonomous non-profit organization Center for social services to the population “Socium” (ANO Center for Social Services to the Population “SOCIUM”)
452550, Republic of Bashkortostan, Mechetlinsky district, Bolsheustinskoye village, street. Lenina, house 2
16
Republic of Buryatia
State Autonomous Institution of Additional Professional Education “Buryat Republican Institute of Educational Policy”
(GAU DPO RB “BRIOP”)
670000, Republic of Buryatia, city of Ulan-Ude, Sovetskaya street, 30
17
Republic of Dagestan
General educational autonomous non-profit organization “Vatan” (OANO “Vatan”)
367015, Republic of Dagestan, Makhachkala city, Magomed Yaragsky street, house 128
18
Republic of Dagestan
State budgetary preschool educational institution of the Republic of Dagestan “Kindergarten No. 92″ Zvezdochka “ (GBDOU” Kindergarten No. 92 “Zvezdochka”)
367032, Republic of Dagestan, city of Makhachkala, street. Mohammed Gadzhiev, house 160 “A”
19
Republic of Mari El
Ministry of Social Development of the Republic of Mari El
424033, Republic of Mari El, city of Yoshkar-Ola, Embankment Bygge street, house 3
20
Republic of Sakha (Yakutia)
Municipal Autonomous Preschool Educational Institution Kindergarten No. 18 “Prometeychik” named after T.S. Komarova urban district “city of Yakutsk”
(MADOU “Kindergarten No. 18 “Prometeychik” named after T.S. Komarova of the urban district “city of Yakutsk”)
677000, Republic of Sakha (Yakutia), city of Yakutsk, Avtodorozhnaya street, 13, building 1 “G”
21
Sevastopol
Sevastopol Regional Public Organization “League of Social Workers”
(SROO “League of Social Workers”)
299001, city of Sevastopol, Rosa Luxembourg street, house 52, apartment 33
22
Sevastopol
Sevastopol regional public organization for the protection of motherhood and childhood “Sevastopol mothers”
(SROO “Sevastopol mothers”)
299000, city of Sevastopol, Lenin street, house 36
23
Sevastopol
Autonomous non-profit organization of additional education “Institute of Family Pedagogy” (ANO DO “Institute of Family Pedagogy”)
299006, city of Sevastopol, Gogol street, house 22 “A”
24
Tambov region
Tambov Regional State Autonomous Preschool Educational Institution “Child Development Center – Kindergarten “Renaissance” (TOGADAU “Center for Child Development – Kindergarten “Renaissance”)
392002, Tambov region, city of Tambov, Pervomaiskaya square, house 15
25
Ulyanovsk region
Regional state budgetary institution of social services “Integrated center of social services for the population” Istok “in Ulyanovsk” (OGBUSO “Integrated Center for Social Services to the Population” Istok “in Ulyanovsk”)
432034, Ulyanovsk region, city of Ulyanovsk, Polbina street, house 45 “A”
26
Ulyanovsk region
Regional state budgetary institution of social services “Integrated center of social services “Doverie” in Dimitrovgrad”0033
433508, Ulyanovsk region, city of Dimitrovgrad, Melekesskaya street.
Click Here for Class Availability and Registration
For more information, to set up a tour, or request a brochure call the office at 301-829-0014 or email Amanda Norman, St. James’ Nursery School Director at [email protected].
Thank you or your interest in St. James’ Nursery School. We believe that the early years in a child’s life are truly significant in their development.
Through careful and thoughtful planning of the learning environment and hands-on experiences, you child is involved in activities that stimulate and motivate their interest and academic growth. Social skills, such as getting along with others and working in a group, are a focus of our program. St. James’ will prepares each child for kindergarten and for later life experiences – and most of all – to enjoy their first school experience!
St. James’ Nursery School holds dual accreditation with the National Association for the Education of Young Children (NAEYC) and the Maryland State Department of Education (MSDE). Additionally, we are licensed with the State of Maryland Office of Child Care, License No. 151353.
Dual Accreditation We work hard to continue being the best preschool in the region, continuing to maintain two accreditations. These accreditations are with the National Association for the Education of Young Children (NAEYC) and the Maryland State Department of Education (MSDE). Additionally, we have yearly inspections with the office of Child Care, the licensing agency with MSDE. License No. 151353. We hold the highest possible rating in the Maryland EXCELS program.
Family Connection and Involvement Your role n your child’s nursery school experience is very important. Families are encouraged to volunteer in the classroom or in other ways. A monthly school-wide newsletter and individual classroom agendas/calendars will help to keep you informed about what your child will be working on in the classroom. Parents are encouraged to volunteer for events throughout the school year. Connections are made at Parent Night, Parent Get-togethers and Class Events, Field Trips, and Parent-Teacher conferences.
Spiritual Growth St. James’ has a deep Christian identity which is foundational to our educational program and part of what makes our school special. Children participate in Chapel Time with our Rector monthly. St. James’ is a member of the National Association of Episcopal Schools. This national organization offers resources for spiritual development, leadership mentoring, grants, and so much more.
Enhancement Experiences A connection to the larger community is an important part of a strong preschool education. Children at St. James’ are involved in a variety of field trips, special guest presentations, monthly library story times, other enriching enhancement experiences. From safety units in the fall with visiting fire fighters to other special visitors children are engaged and stimulated.
Educated, Experienced, and Consistent Staff Our school strives to be the best in early childhood education and our dedication to completing and maintaining these accreditations is a testament to the comment of our administrative and teaching stag. Your child will benefit from this commitment and will gain a strong first school experience.
Innovative Curriculum St. James’ Nursery School follows the guidelines set forth by the Teaching Strategies: Creative Curriculum. This curriculum has been approved by MSDE for use in Maryland accredited preschools. Lesson plans cover all curriculum areas, including: language and literacy, science, math, and social studies. The critical importance of emotional development and social skills are recognized by teachers and addressed on a daily basis.
Families First of Southern MN
Skip to content
HomeVision Design
Head Start
Head Start is a high-quality preschool program that focuses on parent and child development at no-cost for those who qualify.
Learn More
Early Head Start
Early Head Start is a high-quality early childhood education program for infants and toddlers that focuses on parent and child development at no-cost for those who qualify.
Learn More
School Readiness
The School Readiness program allows children 3 years old to kindergarten enrollment to participate in early childhood programs and services.
Learn More
Crisis Nursery
Crisis Nursery is a child abuse prevention and family support program that provides temporary, short-term care for children in Olmsted County while families address a crisis.
Learn More
Child Care Aware
Child Care Aware (CCA) helps families find child care and supports the professional growth of child care programs.
Learn More
Early Learning Scholarships
High-quality early learning ensures our children enter kindergarten ready to succeed in school and life. Eligibility is based on family income.
Learn More
Child Care Wayfinder
Funded through a grant from the Minnesota Department of Human Services, Child Care Aware (CCA) helps families find child care and supports the professional growth of child care programs.
Learn More
Family, Friend & Neighbor Childcare
Family, friend, and neighbor (FFN) providers include grandparents, aunts and uncles, elders, older siblings, friends, neighbors, and others who help families by providing childcare.
Learn More
What’s New
View All News
Consider Contributing to Families First
Thanks for thinking of the parents, children and community members we serve.
Make a Donation
Head Start
Head Start is a FREE Preschool Program Focusing on Parent and Child Development, for those who qualify.
Learn More
Early Head Start
Early Head Start is a FREE, full-day, full-year, family centered early care and education program for pregnant women, infants and toddlers ages 0-3 years and their families.
Learn More
School Readiness
The School Readiness program allows children 3 years old to kindergarten enrollment to participate in early childhood programs and services.
Learn More
Crisis Nursery
Crisis Nursery is a child abuse prevention and family support program that provides temporary, short-term care for children in Olmsted County while families address a crisis situation.
Learn More
Child Care Aware
Child Care Aware (CCA) helps families find child care and supports the professional growth of child care programs.
Learn More
Early Learning Scholarships
High-quality early learning ensures our children enter kindergarten ready to succeed in school and life. Eligibility is based on family income.
Learn More
Child Care Wayfinder
Funded through a grant from the Minnesota Department of Human Services, Child Care Aware (CCA) helps families find child care and supports the professional growth of child care programs.
Learn More
Family, Friend & Neighbor Childcare
Family, friend, and neighbor (FFN) providers include grandparents, aunts and uncles, elders, older siblings, friends, neighbors, and others who help families by providing childcare.
Learn More
What’s New
View All News
Consider Contributing
to Families First
Thanks for thinking of the parents, children and community members we serve.
Make a Donation
Page load link
“I was sitting in the classroom and my mother came for me. She was drunk”
There is a whole list of stable ideas about children from the orphanage in society. For example, that they study poorly and do not want to achieve anything. Rita Westfall for the Arithmetic of Good foundation blog tells the story of Stas, an excellent student who dreams of becoming a famous surgeon and refutes all stereotypes.
Telling about Stas in one article is like telling about the whole universe in a school essay. This boy is so filled with thoughts, feelings, ideas and dreams that it is absolutely impossible to fit everything in letters. But it is very necessary, because it is important for Stas, it is important for his future, and, therefore, it is important for us.
In a video questionnaire filmed 3 years ago by volunteers from a foundation looking for foster families, a brown-eyed, smiling boy says with admiration and confidence that he wants to become a surgeon. Today, after so much time, during which everything would have changed 20 times for an ordinary child, having matured, but the same boy with even greater confidence reports that he dreams of treating people and becoming a surgeon.
Stas will soon be 16 years old. From the maternity hospital, his mother took him home to his older brother Zhenya. But after 3 years, the boy was removed from the family and placed in an orphanage – the mother abused alcohol and could not perform parental duties. Stas remembers little from that time. He knows that he went to kindergarten, where his own grandmother got a job as a nanny. She was allowed to take the boys home.
After 2.5 years, the restriction on the mother’s parental rights was lifted and almost six-year-old Stas was back at home with his mother. “It seemed to me that it was normal there, she, mother, fed us. My grandmother often sat with me. I don’t remember such a thing that my mother read to me or played with me. I remember that she scolded Zhenya. He must have gotten bad grades.” Stas lived at home for about a year, went to first grade.
“I always went to the extension, we studied English there, did our homework, played. I was sitting in the class, and my mother came for me. She was drunk. She said, “Come to me.” And I didn’t know what to do. The school called the police and they took me away. It seems I didn’t cry. I had to wait at the department, there were good aunts, they gave me books. And then they took me to a shelter. Later, my brother was brought there. Mom didn’t come, grandmother came. From there we left for the orphanage. I never lived at home again.”
Stas thinks harmoniously, formulates well and clearly knows what he wants. In the fifth grade, he became an excellent student in all subjects and never studied poorly, showing not just interest and respect for studies, but real passion. “At the very beginning, I studied so-so, even badly. And then, it dawned on me. I felt such a push, strength, and began to learn. Everything went well, I became an excellent student. I love to study, it’s interesting for me. As if something was missing, and once it appeared.
Stas borrows books from the library, additionally works with tutors, attends a circle at a medical institute in order to better know chemistry and understand his future profession. He dances, reads poetry and is fond of theater. “Of course, we don’t have special teachers in theatrical art, but we ourselves prepare productions and perform. I like to recite from the stage, to speak with the audience. I am a versatile person, not only focused on biology, mathematics. I love literature and chemical reactions equally. And I love talking to smart people. To be honest, I don’t know how it happened. I know what they think about children in orphanages.”
Stas’s first memory from the orphanage is the teacher, whom he is very afraid of. The older brother was settled separately, but the fact that he was nearby was great support. Now Zhenya is 21, they are not very close with Stas. “The very beginning of my life is like a fog, I just don’t remember anything. I think I saw my father once. I was standing in the entrance, and there was a man, he brought me something, he was wearing glasses. And this memory that I am small, and he is so big – it is very strong, so I think that it was not just a man.
Grandmother visited Stas regularly and is visiting now. We don’t know why she didn’t get permanent custody, and neither does he. But Stas did not agree to meet with any of the foster families who came to meet him: “I thought it was a betrayal, I could not take and leave her, leave the orphanage for a family.”
Stas takes good care of the pocket money he receives at the orphanage. “I’m not a spender at all, I know how to save money, I’m calm about money. Depending on my mood, I can buy something harmful and eat, but I will never spend everything on unnecessary nonsense. I’m not going crazy because I can’t buy myself what I really dream about yet: a laptop, a cool big one. For example, I have never been abroad. When I finish university and become a surgeon, I will go on my first trip. I’ll start with France, I want to visit Paris. I think it’s a good start for a famous doctor’s vacation!”
Stas knows a lot, but he gets lost on the question of who he could call a significant adult in his life
“You see, I can’t single out anyone. I have the same attitude towards all adults, they are all equal. I took a little bit from everyone, something at school, something at the orphanage. But so that some special adult, no, there is no such thing in my life.
Stas loves books by Michelle Paver, Kate Carey and Cherith Baldry. “He reads a lot in his free time” will be a description of reality, not a figure of speech. In the Chance program, Stas has been studying English, chemistry and biology for two years. In high school, he would really like to take additional subjects in order to improve his USE scores and enter a Moscow university.
Stas’s belief in his own strength, his desire and inner core can motivate any adult with a much easier fate. It is very important for us that Stas remains in the program and has the opportunity to study remotely and further. And it depends on everyone who reads the article about this amazing boy from the Arkhangelsk region.
During the interview, I asked Stas: “What is your worst childhood memory?” “I think it’s something unpleasant that I don’t remember. From very early childhood, for sure.” “And what is the best childhood memory?” “The best is yet to come, I hope. It’s just in the future.”
* The collected funds will be used to pay for lessons for Stas and other children from his orphanage.
You are in the “Blogs” section. The opinion of the author may not coincide with the position of the editors.
Honest songs about the main thing
I wonder if Gumer-aga will sing today? As soon as Fanil thought about it, and then his mother’s voice: “Let’s go quickly, Gumer-aga sings!”
And whoever was doing what at that moment in the large Zamanov family, where there were nine children, everyone quit their job and ran into the house to listen to their favorite singer, whose songs were often heard in the traditional daytime concert on the Bashkir radio.
More than a dozen years have passed since then, and Gumer Abdulmanov’s song “Oak forests are noisy” still remains the family anthem of the head of the Durasovsky village council of the Chishminsky district, Fanil Zamanov, who came to Ufa to open a memorial plaque to his favorite singer. The memorial plaque to the honored artist of the BASSR, holder of the Order of Salavat Yulaev Gumer Abdulmanov was solemnly opened at the address of Richard Sorge, 32/1, where he lived for many years. The artist died on October 20, 2020 at the age of 91, he managed to do a lot in his long life.
The singer was born in 1929 in the village of Chukrakly, Chishminsky District, graduated from the Bashkir Theater and Art School. He worked in the Committee on Radio Broadcasting and Television under the Council of Ministers of the BASSR, the Ministry of Culture. He taught at the cultural and educational school in Sterlitamak, worked as a soloist of the Bashkir Philharmonic. In 1969-1992 he was the director of the Bashkir branch of the musical fund of the Union of Composers of the Russian Federation.
Abdulmanov’s performing style is simple and sincere, the songs are about what is close to everyone. His repertoire included both Bashkir folk songs and vocal compositions by Khusain Akhmetov, Zagir Ismagilov, Tagir Karimov, Rauf Murtazin, Roza Sakhautdinova. He was the first performer of lyrical songs by Rim Khasanov and Talgat Sharipov. The fund of the republican radio stores more than 60 songs performed by him, the most famous of which were hits of the Bashkir stage.
— Gumer-agay and I were born in the same village, I remember him very well, and what always amazed me was his love and interest in people. He very often came to his native village and knew everyone here: not only the representatives of the older generation, but also their children and grandchildren. Previously, transport was not very good, so he brought his friends on the road – artists, dancers, singers, so that they would perform and please people. He was always with us, – says Fanil Zamanov.
“I am very glad that so many people gathered at the ceremony, that so many people love kortatay’s work, respect him as a person,” says the singer’s grandson, music producer, director, songwriter Murat Abdulmanov.
He has been living and working in Moscow for many years, he is a songwriter for Russian pop stars: singer Slava, Yulia Volkova, the Tatu group, Alsu and others. As Murat said, he talked a lot with his grandfather, from whom he and his father passed on a love of music, and from childhood he was inspired by the example of kortatai. Already as a teenager, with the support of his father, Murat organized the Impromptu VIA in Ufa, where he was an artistic director, keyboardist and vocalist.
In 2000, he implemented the republican musical project “We are the Stars” in Ufa, and then the foundation for supporting creative youth “Bashkortostan”. In 2009In the year he moved to Moscow and opened a production company.
– We talked a lot with kortatay, discussed creativity, – says Murat Abdulmanov. – He said: “This is a difficult path, are you sure that you want to go on it?” And I always answered “yes”, because I never looked for easy ways and wanted to be like my grandfather, to achieve the heights that he achieved.
Once he asked me: “Murat, you hold concerts, auditions, auditions. And how do you evaluate the performers, by what criteria do you select? I started listing: clean notes, presentation of the material… And he says: “And you listen to my songs and think about what is important in them, what do you hear in them?” After some time, I analyzed this conversation and now I understand very well that there are things that are much more important than finely tuned notes, perfect recording, glossy arrangements, compliance with the format. In fact, the key to success is not in this, but in singing with the soul, as my kortatai sang, singing with the heart. Only in this way can you reach the listener.
I have been living in Moscow for many years. And to everyone I work with, I say that we, in Bashkiria, have the word “mon”. It is not easy to explain the meaning to Muscovites. It can be said in a modern way: this is a kind of vibe, a flight of the soul, an inner vocal charisma that is “wired” into the voice, into a piece of music that cannot be synthesized artificially, it can only be innate. I always argued with Kortatai, saying that he was of the old school, that now everything is not the same as before, and only now, from the height of the years I have lived (even though I am not old yet, but I am not twenty anymore), I understand that 99 percent of what he said was correct. I am grateful to him for every word and I use the experience passed on to me in my work. I am grateful to my grandfather and father for instilling in me not just a love for music and creativity, but real respect and devotion to this work. Therefore, no matter what situations in life may be, I have never turned off this path and I am going to follow it to the end.
I asked a Moscow producer what songs are becoming popular now.
— I am sure that the secret of the success of artists who are becoming popular right now is honesty. These are songs that are honestly written and honestly performed. There was a period when you could do a good production, write lyrics with the right key phrases, pay and get the song on the radio station. Now everything is changing, and songs that have been lived are becoming popular: if this is lyrics, then this is a song of suffering – text, music, performance. I think if Gumer Abdulmanov were alive and young now, he would sing his songs, of course, in a modern interpretation, and would be a popular and respected artist. After all, what is happening around now, in general, repeats the time when he was just embarking on his musical path, says Murat Abdulmanov.
According to the producer, covering old songs – covers, which are now very popular, is partly a good trend: it is a tribute to the artist who first performed the song, its author.
— Therefore, I think it is possible and even necessary to cover songs. They must live forever, I myself strive for this in my work. I want to leave something behind: it is very important for me to live this life not just as an average resident of the Russian Federation, leaving behind only children and grandchildren. I want to leave something for the people, for society. I hope that my songs will remain after me and my children and grandchildren will be just as proud of me as I am proud of my kortatai,” says Murat Abdulmanov.
The producer believes that in Bashkiria today there are big problems with the quality of music content. “I specifically watched BST and Kurai for half a day and saw on these channels a lot of low-quality music videos, clips, if you can call them that. Why is everything so bad with the quality of music content in our republic?” – Abdulmanov asked this question in a letter to the head of the republic, Radiy Khabirov, last year. He called the clips that are broadcast on local TV channels a shame, and said that he did not believe that they did not have the resources to shoot quality videos and record quality music. “You give grants for the implementation of projects, but there are no results! It’s sad for me to look at clips in a field or a birch grove, exactly the same as my kortatai had 50 years ago, ”wrote the producer.
– It just felt very sad for our native republic, for the fact that someone on the ground does not want to do anything in order to improve the quality of video content on TV.
Miami Babysitter Agency – Babysitter Services for Miami parents. Find a trustworthy Babysitter in Miami
Sign in
Advanced caregiver search
Find caregivers by country
Find caregivers by nationality
Find caregivers by language
Find child care
Find nanny
Find babysitter
Find au pair
Find tutor
Find housekeeper
Find senior caregiver
Find pet sitter
Find personal assistant
Advanced job search
Find jobs by country
Find jobs by nationality
Find jobs by language
Find child care jobs
Find nanny jobs
Find babysitting jobs
Find au pair jobs
Find tutor jobs
Find housekeeping jobs
Find senior care jobs
Find pet sitter jobs
Find personal assistant jobs
Resources
Founders’ Video
Customer Videos
GreatAuPair customer reviews
Security Center
How to find caregivers
How to find caregiver jobs
Interview questionnaire
Au pair program requirements
Au pair programs
J-1 au pair visa costs
Au pair & nanny salary
Au pair visa programs
Au pair agencies
Caregiver & nanny taxes
Child care tax deduction
Immigration services
Advertise on GreatAuPair
Work for GreatAuPair
Deborah O.
Italian hard-working and honest baby sitter
Hi!
I am an honest hard-working italian woman. I would like to take care of your children. I am a teacher too. I am organized and reliable. …
more
Last logged in
Today
Available Nov 22 – Dec 22
View
Babysitter 3242060
Seeking
Full Time,
Live-in
View
Babysitter 3242060
Nity R.
I love babies!
I love kids, please read all the things I can do, I also have a video online! cheers!…
more
Last logged in
6 days ago
Available Nov 22 – Dec 22
View
Babysitter 3183627
Seeking
Full- or Part-time,
Live-in or Live-out
View
Babysitter 3183627
Natasha L.
Responsible Babysitter in Davie seeks Babysitter Job
Sou brasileira, me mudei pra Fort Lauderdale há 1 mês, no Brasil eu atuava como dentista dias de semana, e final de semana eu era babá para algumas famílias conhecidas que os pais saiam ou viajavam final de semana e eu ficava responsáve…
more
Last logged in
6 days ago
Available Oct 22 – Sep 24
View
Babysitter 3265937
Seeking
Full- or Part-time,
Live-out
View
Babysitter 3265937
Tania m D.
Mi nombre es Tania, soy colombiana
Hola me llamo Tania y me considero una persona sociable y manejo la empatía. Una persona capaz de adquirir nuevas experiencias y conocimientos….
more
Last logged in
9 days ago
Available Nov 22 – Dec 23
View
Babysitter 3265428
Seeking
Part Time,
Live-out
View
Babysitter 3265428
Tona W.
Former Teacher looking to babysit
I am a former teacher, ESL teacher and homeschooled my own kids to middle school. I have a criminal background check. I have had a side pet sitting business for 18+ years with ‘s Wags and Whiskers. I am hoping to branch out to childc…
more
Last logged in
12 days ago
Available Oct 22 – Sep 24
View
Babysitter 3264124
Seeking
Part Time,
Live-out
View
Babysitter 3264124
Best Babysitter in Miami, FL
Meredith R.
Babysitter in
Miami, FL
My family has 5 members including my little brother that is 5 years old and my sister which she is 16 years old. Since I’ve been the biggest… Read More
$13 – $25 / hr
•
12:00 am – 11:45 pm
Larimal G.
Babysitter in
Miami, FL
“I’ve was an after school care teacher for two years, then was a preschool teacher for the past three years and I am currently a VPK teacher… Read More
$15 – $40 / hr
•
8:00 am – 11:45 pm
Diana Marcela C.
Babysitter in
Miami, FL
Niñera con 2 años de experiencia en cuidado de niños y bebés.
Soy una persona organizada y muy creativa, constantemente organizo dinámic… Read More
$20 – $25 / hr
•
9:00 am – 5:00 pm
Jessica S.
Babysitter in
Miami, FL
I am an older sister of 3 brothers. I had my first brother when I was 12. Since little, I have had those maternal and nursing instincts. I a… Read More
$22 – $35 / hr
•
7:00 am – 11:45 pm
Stephanie D.
Babysitter in
Miami, FL
I’ve been in the child care field for about 3 years now and it’s been the best experience for me because my passion has always been to be su… Read More
$20 – $30 / hr
•
6:00 am – 11:45 pm
Maria F.
Babysitter in
Coral Gables, FL
My mother has been running a successful home day care since before I was in school and is still currently running it so I have lots of exper… Read More
$17 – $26 / hr
•
8:00 am – 11:45 pm
AR
Andrea R.
Babysitter in
Miami, FL
And a very intelligent, hard-working, fun and intuitive person I don’t let things get me down so easy and I always look for a solution apart. .. Read More
$18 – $45 / hr
•
6:00 am – 11:45 pm
Jamila S.
Babysitter in
Miami, FL
I’ve been a babysitter for 3 years and I love the kids and the kids love me
$25 – $100 / hr
•
12:00 am – 11:45 pm
Xochilth E.
Babysitter in
Miami, FL
I like babysitting and I am very patient with them. It would be my pleasure to help you with the care of your children.
$20 – $35 / hr
•
8:00 am – 11:45 pm
Svetlana O.
Babysitter in
Miami Beach, FL
I have been working as a nanny for over 10 years. By education I am a Librarian -bibliographer. I have experience working as a nanny with a … Read More
$20 – $35 / hr
•
12:00 am – 11:45 pm
Map
Location not displayed
Search map as I move
List
Popular Searches
Nearby WeeCare Neighborhoods
Nearby WeeCare Cities
Child Care Job in Miami, FL
Entrance
Extended search for desired
Find trustees by country
Find caregivers by nationality
Find trustees by language
Find childcare
Find a babysitter
Find a babysitter
Find an au pair
Find a tutor
Find a housekeeper
Find a head caregiver
Find a pet
Find a personal assistant
Advanced Job Search
Find a job by country
Find a job by nationality
Find a job by language
Find a childcare job
Find a babysitting job
Find a babysitting job
Find an Au Pair Job
Find a job as a tutor
Find a job around the house
Find a job caring for the elderly
Find babysitting jobs
Find a job as a personal assistant
Downloads
Founders Video
Customer video
Customer Reviews GreatAuPair
Security Center
How to find caregivers
Finding a Career Job
Interview Questionnaire
Au Pair program requirements
Au Pair programs
J-1 Au Pair visa fee
Au Pair and Nanny Salary
Au Pair visa programs
Au Pair agency
Guardian and nanny taxes
Child care tax deduction
Immigration Services
Advertisement on GreatAuPair
Work for GreatAuPair
James M.
Housekeeper
…
Last logged in today
Available Oct 22 – Oct 22
View Housekeeper Job 3267965
The job is full time or part time, live or live.
View Housekeeper Job 3267965
Jimmy N.
North Miami Beach family looking for guardian for elder
Companion, caretaker, companion, driver, when it is necessary to take the elder to the doctor, a car will be provided. Full-time job, but may be residential. Our goal is to find someone who can grow up to a full time and live a 5 month old…
Read more
Last logged in today
Available Nov 22 – Jan 23
View the work of the senior educator 3262993
Full-time work, live or alive
View the work of the senior educator 3262993
Edward L.
Senior assistant needed
Five years ago, he suffered a stroke that affected his right side. I need help showering, getting dressed, but above all I need a companion, someone to talk to, a nice person. If anyone I’ve interacted with before has read…
Read more
Last logged in yesterday
Available Feb 23 – Mar 23.
View Senior Caretaker Job 2733135
Full Time Job, Live-in
View Senior Caretaker Job 2733135
Nadia B.
Housekeeper / nanny
Position: Live in Housekeeper/Nanny SUMMARY: The Nanny/Housekeeper is a specialist working in the family home, responsible for all tasks related to the upkeep of the home and childcare. MAIN DUTIES AND RESPONSIBILITIES …
Read more
Last logged in 4 days ago
Available Nov 22 – Dec 22
View Housekeeper Job 2105606
Full time job, from life
View Housekeeper Job 2105606
Chonticha S.
Live in a nanny
…
Last login 10 days ago
Available Oct 22 – Oct 22 for 4-14 months
View job Au Pair 3264741
Full or part-time job, Live-in
View job Au Pair 3264741
Nanny jobs in Miami – job search without intermediaries on the site Homey.
pro
Advanced search
clear filter
Geolocation of work
City
Miami
Area
All districts
Underground
Specify metro
Determine location
Schedule
Full time employment without accommodation
Full time with accommodation
Part-time employment
Watch without accommodation
Watch with accommodation
Daily
night shifts
Weekends
1 half day
2 half a day
Age
work experience
Without experience
From 1 year
From 2 years
From 3 years
From 4 years old
Over 5 years
Payment
₴
From
₴
Before
Education
Higher
Specialized secondary
Average
Speciality
Pedagogical
Medical
Recommendations
Not required
Desirable
Wanted
To use sorting by distance, enter your address
Address
Sort
By date added descending
By salary
By salary
By date added
By date added
By experience
By experience
By distance
By distance
Need a nanny-governess in the USA (Miami)
Miami
Age
from 35 to 55
An experience
2 years
Salary
Negotiated
Description
Job information
Position: Nanny – governess
Working conditions: Boys, 8 years old – twins, 5 years old and 6. 5 years old, with accommodation (2 nannies, a nanny is needed for the younger ones)
Responsibilities: Babysitting, childcare, laundry, ironing, escort
More details
Nanny Live in Miami
Miami
Age
from 38 to 55
An experience
3 years
Salary
Negotiated
Description
Vacancy: Nanny with accommodation for a boy of 13 months.
Getting Started: Now.
IN THE USA. US visa required. The employer does not issue a visa. WHO vaccination required to enter the US
Read more
Nanny for a child of 5 months in Miami (USA)
Miami
Age
from 35 to 60
An experience
No experience
Salary
Negotiated
Description
Nanny needed in Miami (USA) for a 5 month old baby.
With accommodation 6/1. Care, feeding, walking, bathing, washing children’s things, maintaining cleanliness in the children’s room. The nanny has a separate room for living.
Baby receiving blankets are a must-have on any baby registry. They’re so versatile and useful, that almost every new parent will swear by always having them on hand.
But there’s a lot of options. Like which material is best? How big should they be? What’s the difference between vs. swaddles or sleep sacks? Do I need swaddle blankets and receiving blankets? Be sure to read through our guide of FAQ’s on baby receiving blankets below. But the short answer is they are awesome. You need to stock up receiving blankets for babies.
Below we break down a list of the best receiving blankets for babies, swaddles, and sleep sacks. Plus what to look for when choosing the best baby receiving blankets for you and your little ones.
Do I need receiving blankets? Yes! They are so versatile and useful. A must-have to add to your baby registry.
Best Muslin Baby Receiving Blanket
Muslin Baby Swaddle Blankets Set of 4
The colors on this set of baby receiving blankets are so rich and luxe. They are gorgeous and the softest baby blanket for swaddling and tons of other uses too. They’re definitely a unique style and color.
Viviland Baby Muslin Swaddle Blanket
If you’re a mermaid lover, these are an absolute must for your baby. They’re made of silky bamboo making them super soft baby blankets, and the mermaid pattern is so fun! Perfect for a little girl, but hey, boys like mermaids too on their baby receiving blankets.
CozyBubs Swaddle Blankets Set [3-Pack]
It’s the sweet little elephants that got up on this one. Just so charming, and made with hypoallergenic materials that are chemical-free. Perfect for worry-free cuddling and swaddling.
LollyBanks 100% Cotton Muslin Swaddle Nautical Ocean Baby Blanket Set
So in love with the blue nautical vibes from these fishy cotton baby receiving blankets. The blue whales, waves, and sharks scream little boy. The designs are so kid-friendly, but a stylish take on typical kid prints.
Baby Swaddle Blanket Upsimples Unisex Swaddle Wrap Soft Silky Bamboo Muslin Swaddle Blankets Neutral Receiving Blanket for Boys and Girls
With four swaddles in this pack, it’s a good bang for your buck without sacrificing quality. They are highly popular with parents because they are big, soft, and have delightful animal patterns. They’d work great as baby receiving blankets.
Best Organic Baby Receiving Blanket Set
LifeTree Baby Boys Girls Swaddle Blanket
It doesn’t get more aesthetic than this swaddle set. They are gorgeous and would fit in nicely with a cottagecore theme nursery or newborn shoot. Choose from packs for 2, 3, or 4 to stock up on these 100% organic baby receiving blankets
Oliver & Rain Organic Muslin Swaddle Sampler
Grab these adorable muslin baby receiving blankets in packs of one, two, three, or four. Choose from a bunch of different totally aesthetic options. These are very gender neutral without giving up the cute factor, and parents rave about how they are such super soft baby blankets.
If you have a woodland or cottagecore themed nursery or newborn shoot, then these are a must! The prints on these are simply enchanting, and gender-neutral. Reviewers love the high quality that makes these feel like luxury baby blankets and baby receiving blankets.
Burt’s Bees Baby – Blankets, Set of 2, 100% Organic Cotton Swaddle
Change it up from the muslin receiving blankets to these organic cotton receiving blankets from a trusted brand, Burt’s Bees. These are a bit smaller in size than the muslin blankets, but they do seem to be a bit thicker. Parents love using these to cover up babies after they’re all buckled up in the carseat.
Muslin Swaddle Blankets – 100% Organic Cotton
Want organic swaddling and baby receiving blankets, but with a bit more pop of color? Try these! Babies and kids will love the bright colors and animals that are a bit more of a traditional baby style vs. trendy.
Best Flannel Baby Receiving Blanket
Simple Joys by Carter’s Baby 7-Pack Flannel Receiving Blankets
With seven flannel baby receiving blankets in this pack, it is such an awesome value. If you want something for burping and a soft receiving blanket to lay your baby on, these seem awesome. They are a littel small for swaddling though. So if swaddling is your jam, maybe keep looking.
Gerber Boys and Girls Newborn Infant Baby Toddler Nursery 100% Cotton Flannel Receiving Swaddle Blanket
Super cute and cozy, these Gerber baby receiving blankets have charming prints and design. Some reviewers loved them for swaddling, but for others the size wasn’t quite right. It can be hard to find just the right size swaddling and receiving blankets that are made of flannel.
An affordable price and lots of color and pattern options make these receiving blankets a perfect choice for a lot of families. These are on the smaller side compared to a lot of the muslin blankets on the list. So they might not be the best for waddling, but would be great for burping and general use.
Best Mom and Baby Receiving Blanket Matching Set
4 Pack Maternity Robe and Matching Baby Swaddle Blanket with Hat Headband Set
Create picture-perfect newborn photos while matching your new bundle with this receiving blanket and robe matching set complete with hat and headband.
This set has different patterns and color choices, but all are quite feminie. So if you want something gender-neutral, this isn’t the set of baby receiving blankets and robe for you.
Matching Maternity/Delivery Robe with Baby Swaddle Set
For a ton of different patterns and color choices, go for this matching robe and baby receiving blankets set. There are so many options you’ll be sure to find a set that fits you and your little one’s personality and style.
Plus, a lot of the choices are gender-neutral if you are team green (don’t know the baby’s gender).
Mommy and Me Family Matching Women’s Pajamas and Baby Swaddle Blanket/Hat Set
Most matching sets for parents and newborns are robes, but this one is awesome because it’s pajamas! There are a few different options, most of which are floral and feminine, but this blue pattern is a nice choice for a boy or gender-neutral.
Best Baby Swaddle Sleep Sack
Happiest Baby Sleepea 5-Second Swaddle
This space design is absolutely delightful, and straight up cool. But parens also love the ease with which you can swaddle up your babe in seconds. It’s made of organic material and is ranked the #1 swaddle by the New York Times.
A simple wearable blanket made of fleece to keep your baby warm and cozy. The design is so easy to use, even for sleep deprived parents during middle of the night diaper changes.
Nested Bean Zen Sack – Gently Weighted Sleep Sacks
If you have a little one who struggles to sleep, this might be a good investment. While it didn’t work for every single babe, it helped enough parents who swear by this that it is definitely worth a try!
Baby Merlin’s Magic Sleepsuit
Another product that is hit or miss with babies, but for some families it is a game changer! It’s a super cuddly suit that helps babies feel safe and secure while sleeping so they wake less. If you are desperate for some sleep, give this a go.
What is a receiving blanket for a baby?
Receiving blankets are thin and soft multi-purpose blankets mostly used for newborns and small babies. The best part of baby receiving blankets is they can be used for so many different things like a burp cloth, a swaddle, a blanket for warmth, a playmat, and more! They’ve been around for basically… ever… and with good reason. They’re so functional and inexpensive.
Do babies need receiving blankets?
There are not a lot of baby items that are truly must-haves for everyone, but baby receiving blankets should be on your registry or shopping list for 99.9% of families.
The versatility of receiving blankets is key, and the fact that you can get a large pack of them at a decent price is a bonus. While some families will prefer other types of blankets or swaddles, nearly all at some point use receiving blankets.
How Many Receiving Blankets Do I Need?
It depends on how often you do laundry! Seriously, if you do laundry daily, you can probably get by with 3-5. But if you’re a little lax on the laundry routine, you’ll probably want to stock up on maybe 10. That way if you have a blowout in one and spit up on another, you’ll have plenty left to get you through the day without having to do the wash.
What is the difference between a receiving blanket and a baby blanket?
A baby blanket is more of a comfort item or a blanket used for warmth. While a receiving blanket has a lot of different uses, and can also be used as a swaddle, which baby blankets usually aren’t made for. Baby blankets also tend to be thicker than receiving blankets that are generally made of thinner lightweight materials like muslin.
Do I need to bring receiving blankets to the hospital?
You don’t need to. Unless they tell you otherwise, hospitals have tons of receiving blankets for you and your baby to use while you’re there. In fact, many hospitals want you to take them home with you too!
If you have specific preferences or needs for you or your baby you can always bring your own too. Especially if you want something that’s a little more aesthetic than the hospital ones.
Receiving Blanket vs. Swaddle Blanket: Are receiving blankets and swaddle blankets the same?
Yes, and no. Receiving blankets can be used as swaddles, but many times when people talk about swaddles now, they are referring to something more like a sleep sack than a swaddling or receiving blanket.
Pampers Baby Dry vs Swaddlers: What’s the Difference?
Sharing is caring! Facebook Twitter Pinterest The diaper aisle is packed with different choices, how should new parents decide which is best for their little one? If you’re deciding between …
Pampers Baby Dry vs Swaddlers: What’s the Difference? Read More »
Pampers Swaddlers vs Cruisers: Which One is the Best Diaper for Your Little One?
There are so many choices you have to make as a new parent. Whether it’s diapers or formula vs. breast, each one feels like such a big deal, and with …
Pampers Swaddlers vs Cruisers: Which One is the Best Diaper for Your Little One? Read More »
The 10 Best Toddler Shampoo and Conditioner in 2021
Want to make sure your toddler has some gorgeous locks? Keep reading for all the best toddler shampoo and conditioner plus hair care products for easier do’s. Toddler hair can …
The 10 Best Toddler Shampoo and Conditioner in 2021 Read More »
What to Wear After Giving Birth: the Best Options According to Real Moms
Yay! You’re having a baby. Working on that hospital bag checklist and not sure what to wear after giving birth? I’ve got you covered. Postpartum is such a beautiful, messy, …
What to Wear After Giving Birth: the Best Options According to Real Moms Read More »
Supplies for Pumping at Work: 7 things You Truly Need
Going back to work after maternity leave can be so hard, but having the right supplies for pumping at work can help smooth the process a little. These 7 supplies …
Supplies for Pumping at Work: 7 things You Truly Need Read More »
Similac Advance vs. Pro Advance – What’s the Difference?
Similac Advance vs. Pro Advance… which formula should you choose? You’re in the right place. If you’ve narrowed your choices down to Similac Advance vs Pro Advance, but just can’t …
Similac Advance vs. Pro Advance – What’s the Difference? Read More »
Receiving Blankets and Its Uses for Babies
Home Baby What Is a Receiving Blanket and How to Use It?
What Is a Receiving Blanket?
Various Uses of a Receiving Blanket for Babies
What Else Can a Receiving Blanket Be Used For?
Receiving Blanket Safety Tips for Babies
How to Select the Right Receiving Blanket for Your Child
What Is the Difference Between Receiving Blanket and Swaddling Blanket?
DIY Receiving Blanket
As a mother, you’ll never forget the moment when you held your baby in your arms for the first time. You must have noticed, every little detail about your baby, his nose, his eyes, his tiny hands and fingers, and even the soft white blanket he was wrapped in. Now you must have folded up that receiving blanket neatly in a drawer and perhaps it will never see the light of the day, but do you know that your little munchkin’s first blanket can be used in so many ways? The very first blanket that many families receive their baby snuggled up in is called a receiving blanket. Read on to learn more about receiving blanket and how can you put one to good use once it has served its purpose!
What Is a Receiving Blanket?
A receiving blanket is a blanket that is used to snugly wrap a newborn before giving him to his family members. Normally it’s a thin, soft cotton blanket that is sold in packs of two or four and a staple at maternity wards. While they have the sentimental value of being the first-ever cloth wrapped around your baby, they are useful for a wide variety of applications from cleaning spit-ups to keeping a baby dirt-free. While hospitals usually provide one, most new mothers tend to buy standard off-the-shelf receiving blankets for their babies, as one can never have enough of receiving blankets for their babies. If you want to make it extra special, you can always make one yourself.
Various Uses of a Receiving Blanket for Babies
A receiving blanket can prove to be very useful if you know how to use it right. Let’s find out how you can use your little one’s first blanket over and over. You can also buy new receiving blankets if you would like. Receiving blankets can be used for the following:
1. Swaddling
The size of receiving blankets makes them the perfect first cloth to swaddle your wriggly baby. Once you learn how to swaddle your little one, you will have no trouble in calming him down!
2. Wrapping Up After A Bath
You can use your baby’s first blanket to wrap him up after a bath. The soft and familiar fabric of the receiving blanket will keep your little one comfortable.
3. As a Breastfeeding Cover-Up
If you prefer privacy while breastfeeding your baby, you can use a receiving blanket to cover up when you’re breastfeeding on the go. Its small size makes it easy to carry around in a diaper bag.
4. As a Stroller Shade
Your baby’s first blanket can be put to good use when you go for a stroll to the nearest park with your baby. Keep one in the stroller basket and use it to block the sunrays from hurting your baby’s eyes.
5. As a Diaper Changing Mat
A receiving blanket can be used as a diaper changing mat too. If you need to change your baby’s diaper in a public restroom, spread the blanket on the designated surface and change his diaper comfortably.
6. As a Play Mat
When visiting a friend’s place or the park for the evening, receiving blankets can pass for a perfect play mat if you forget to pack one.
7. As a Sleep Prop
If there’s anything that your baby will fall asleep in without throwing tantrums, then it’s the receiving blanket. The familiar scent and warmth will provide comfort to your baby and he will fall asleep in it in a matter of minutes.
8. As a Burp Cloth
If your little one is a messy eater, this amazing length of cloth can save you a lot of cleaning time!
What Else Can a Receiving Blanket Be Used For?
If you want to hold on to your baby’s first blanket, then you will always find a reason for it. And you’ve every right to keep it, after all, it will bring back the memories of your baby’s first day. If you tend to be on a creative side and don’t want to stuff the blanket at the back of your closet, you can always put it to good use. Find out how you can use your little one’s receiving blanket.
1. For Sentimental Value
You can make quilts, stuffed toys or pillows out of your baby’s first blanket and keep them in your baby’s room or living room for the years to come.
2. For Room Decoration
Once your baby turns 1 year of age and you feel he is too old for his first blanket, you can cut the blanket into different shapes to make banners or garlands. Being soft and thin, they are easy to cut through, so no hassle there!
3. To Make Aprons for Different Activities
Being easily washable, the blankets make excellent apron material for your child when they turn into little artists.
4. As Furniture Covers
You can use them as a quick furniture cover during your little one’s mealtimes or when your little one explores his creative side on a couch. Your little one’s first blanket will quickly absorb any spills and save your precious furniture.
5. For Cleaning Purpose
While most moms don’t prefer using their babies’ first blanket for cleaning purpose because of sentimental value attached to them, but if you don’t mind, you can use your little one’s first blanket for cleaning his spit-ups or to wipe liquid spills on the surface.
Receiving Blanket Safety Tips for Babies
You may be surprised on reading safety tips regarding the usage of receiving blanket for your baby, but you can never be too careful with babies. Follow these tips when using a blanket for your baby.
Never leave loose blankets in your baby’s crib.
Never cover your baby completely with a blanket in his first year.
Do not wrap the blanket around your baby’s head or neck.
Do not swaddle your baby when he starts rolling over.
How to Select the Right Receiving Blanket for Your Child
Typically a receiving blanket is made out of soft cotton and measures 30 inches by 30 inches. They come in a range of materials and designs. Ultimately it’s up to you and your preferences with colour and texture to buy the best one for your baby. Blankets made out of pure cotton are ideal as they are breathable and soak up moisture readily without making it uncomfortable for your baby. It also has excellent thermal properties, making it a great first choice.
What Is the Difference Between Receiving Blanket and Swaddling Blanket?
Many people tend to use receiving blankets and swaddle blankets interchangeably, but these two are different. While receiving blankets can be used to swaddle a baby, they can’t be used for long enough as babies quickly outgrow them as they grow up. The major difference between the two is their size. A receiving blanket is usually 30 inches by 30 inches while a swaddling blanket is usually 47 inches by 47 inches. Swaddling blankets are made out of a more elastic material to make it easier to wrap your baby. They also feature attachments such as Velcro or button clips to keep it in place while your baby is wrapped.
DIY Receiving Blanket
If you want to make a customised receiving blanket for your baby, here’s how you can make one. Follow the instructions given below to learn how to make a receiving blanket at home:
Supplies
Soft, washable fabric or flannel – 1 yard
A thread of matching colour
A pair of scissors and straight pins
A sewing machine or serger
Instructions
Start with preshrinking the fabric.
Trim off the selvedges from the fabric and cut it into a squared rectangle.
Using a sewing machine, make a rolled hemstitch along the perimeter covering all edges.
If you don’t have a sewing machine make a baby hem by turning the fabric to the wrong side along the edges about ¼ inch wide. Turn the 1/4th inch edge under a second time and enclose all the raw edges. Pin it in place and miter the corners.
Make a topstitch or hand-sew the hem to keep it in place.
Ensure the edges are secured and there are no raw edges as the blanket will be washed often.
If you’re using a decorative blanket, use a decorative topstitch for the hem.
Swaddling blankets not only carry with them the memory of your child’s birth but they are also a great source of comfort for the baby in his first year. Although their primary purpose is to wrap the baby, they can be used throughout your baby’s first year. So bring out that receiving blanket of your little one and put it to good use.
Also Read: When and How to Stop Swaddling Your Baby
Previous articleSimple and Fun Things to Do With a Toddler
Next articleWhen Can a Baby Sit in a High Chair?
Ruchelle Fernandes
Ruchelle has a vast experience working with clients in hospitality, health and wellness, entertainment, real estate, and retail. She aims to utilise her learnings to deliver quality content which will in turn help drive sales and customer engagement.
ADVERTISEMENT
POPULAR POSTS
ADVERTISEMENT
LATEST
What Do Breastfeeding Moms Really Want?
Ruchelle Fernandes –
Hands up if you thought breastfeeding would be easy – but then struggled! To mark World Breastfeeding Week in August this year, Australian breastfeeding. ..
Bad childhood habits: how to fight?
We call a habit an unconsciously repeated action that plays a certain role and also has its own reason. For a child, this is a ritual that is performed under the condition of the occurrence of certain life circumstances. Many habits are considered bad habits, although they really are not. However, they should be combated, because pathological habits have an undesirable effect on the development of the child. A bad habit develops into a necessary calming ritual that helps the baby distract from anxiety, fear, or compensate for a lack of communication. All this threatens to delay the mental development of the baby, and also distracts him from cognitive processes.
1 When a baby sucks on a blanket
2 Ways to solve the problem
3 When a child sucks his thumb
4 Thumb sucking at an early age
5 Thumb sucking at an older age
6 Ways to solve the problem
7 When a child bites his nails
8 Ways to solve the problem
When a baby sucks on a blanket
Some babies get used to holding the blanket close to them, holding it to their face, or even taking the end of the blanket in their mouth and sucking. Usually the child does this when getting ready for bed, and may become so attached to this item that he will flatly refuse to part with the blanket, even when it needs to be washed. Usually such a habit does not reveal any serious consequences for the child, although it can greatly annoy parents. The habit of sucking on a blanket remains until the age of 8-10, and then disappears without a trace. Why does this habit occur?
It often happens that a child is afraid of the dark, afraid to be alone in the dark when the parents turn off the light in his room, or simply afraid to be alone. In order to fight his fear, the child becomes attached to the things around him, transfers friendly feelings to them. An imaginary friend will protect, understand and always be there. The presence of a soft toy can bring similar comfort to a baby, but attachment to a blanket is possible. Sucking on the blanket or holding it close to him, the child seems to make sure that a friend is next to him. For children, suckling is a much more familiar way of warding off fears than talking. By his actions, the baby subconsciously signals that he is experiencing anxiety, inconvenience, that he is scared. Such a habitual action, like sucking on a blanket, stabilizes the state of mind of the baby. This is purely a childish habit, passing with age.
But even adults often behave like children. By remembering this more often, you will stop worrying about the child’s behavior in vain.
Ways to solve the problem
First of all, stop making a problem out of it (pun intended, but nonetheless). The habit of sucking on a blanket will go away on its own with age. If you want to do something, then heed the following advice:
Reward the child for his success, thereby encouraging maturation.
Give your baby more time, especially before putting him to bed – sit next to him, tell / read a story or just talk to the child.
Leave a night light on all night if your child likes it.
Don’t blame your baby for sucking on the blanket. Instead, show him your confidence that sooner or later the baby will stop doing this.
Do not bribe a child to make him forget about the blanket.
I must say that blanket sucking is not such a common habit, and is not so harmful – in a word, it is not more harmful than others. Some children suck their thumbs, some are tied to a blanket, others refuse to talk normally for a long time, preferring to babble. These habits only show us that the child does not want to leave a certain stage of childhood and move on to a new stage of development, even if he really wants to grow up quickly.
The task of parents is to help children, not scold them. Treat your child like an adult, and very soon you will see that the baby has broken with his habit.
When a child sucks his thumb
Thumb sucking is a fairly common habit in children. You shouldn’t worry too much about this, but you don’t need to let the situation take its course. We will try to prevent and, if necessary, eliminate this habit.
Parents quickly get bored when their comments do not bring the expected results. Then they begin to treat the child as if he were deliberately sucking his thumb. There are situations when parents, whenever they find that the child has put his thumb in his mouth, order him to take it out, but after a minute the finger returns to its original place. Desperate, adults can raise their voice at the child, punish him, accuse him of disobedience, humiliate him and remove his finger from his mouth by force. Bitter mixtures smeared on the finger or gloves are used.
To be fair, these methods sometimes work. But, unfortunately, for the psyche of the child, they are very harmful. Harsh, demanding and rude methods spoil the child’s relationship with his parents. A child will not have a better opinion of you after such pressure, and it is unlikely that he will love you stronger. On the contrary, the baby will consider you impatient, unpleasant and overly demanding people (even if he cannot yet formulate his opinion in words). To understand the feelings of the child, imagine that the boss behaves in a similar way with you.
But that’s not all. Weaning a child from thumb sucking does not solve the problem. The child can replace the finger with something else that is less visible to the parents. After all, it is we who are satisfied that the child has stopped sucking his thumb, and not the child himself! The main task facing parents is to understand what exactly they want to get rid of. Thumb sucking is harmless to the child’s psyche. But, nevertheless, from a psychological point of view, this habit should be eliminated, because it is an alarming symptom. It can indicate two reasons related to the age of the child.
Thumb sucking at an early age
Thumb sucking at an early age signals that the baby is not suckling enough. After all, sucking is his natural need.
At the age of 6-7 months the first teeth appear. Sucking helps soothe irritated gums.
The baby switches to semi-liquid food, the baby begins to eat from a spoon, and the parents forget his suckling needs.
Some parents start weaning their baby from the bottle long before the baby is ready.
Some parents encourage the baby to drink milk quickly, but the baby does not have time to satisfy his need to suckle.
Helping a child in this case is not difficult at all. Just let the baby suckle enough during meals. Get nipples with small holes so that the baby drinks the contents of the bottle slowly, over 20-30 minutes. In a month or even earlier, the baby will stop sucking his thumb.
Thumb sucking at an older age
What could be the reasons?
The previously acquired habit has been preserved.
The influence of the degree of immaturity, that is, the so-called return to an earlier stage of development. It happens that, having learned to use the potty, the child suddenly begins to dirty his pants again. Or, having learned to dress on his own, he begins to act up and demand that his parents dress him again. Similarly, once weaned or bottled, a baby may want to suckle again. If this continues for a long time, it signals that the child for some reason does not want to grow up (it is necessary to identify the reasons)
The child feels fear or powerlessness. Thumb sucking is pleasurable and pleasurable to the baby, as it is associated with infantile pleasurable sensations (sucking = hunger satisfaction).
Solutions
Do not remove your finger from your child’s mouth. You can give the baby caramel, sucking candy.
Don’t go back to the bottle.
Consider thumb sucking as one of the ways your child wants to stay small. Watch the child – he should show some other too childish habits, for example, excessive tearfulness, deliberately childish babble, unwillingness to eat or dress on his own, unwillingness to communicate with peers. By encouraging the child to grow too much, we retard his development. Be patient, be more affectionate and softer, show interest in adult moments in the child’s behavior. Approval and love give children courage and perseverance. In their absence, children become infantile and lost.
Try to rid the child of fear. It often happens that a child sucks his thumb when he is afraid of something (for example, he is afraid of big dogs, or is afraid when his mother raises his voice, or is afraid of the dark and falls asleep with his thumb in his mouth).
It is better to do nothing than to do something wrong. If you don’t understand why a baby sucks its thumb, don’t rack your brains. This habit in itself is not so terrible.
When a child bites his nails
Why does a child bite his nails? There may be several options.
The child is simply pleased, he receives physical satisfaction. In this case, to wean the child from this habit, offer him an activity that will bring a lot of pleasure to the baby.
This habit allows the child to return to an earlier stage of childhood. Putting a finger in the mouth, the child reproduces the movement familiar from infancy. The kid seems to say by this that he is not yet ready to grow up.
In this way, the child expresses his aggression – for example, he irritates his parents by showing hostility.
There is a strong impulse in the child’s soul that makes him bite his nails, thereby freeing himself from aggressive stimuli.
It is difficult to get rid of this habit because it arises easily. No threats, no punishments, no rewards are recommended here. You should not make comments to the child. First of all, you need to understand the reasons that gave rise to the habit of biting your nails. The reasons for this lie in the feelings of the baby. Biting his nails, the child tries to get rid of psychological discomfort, relieve tension, at the same time enjoys and releases the accumulated aggression.
Ways to solve the problem
Try to make the child’s life more pleasant and fun, eliminate the causes that create tension and oppress the baby. Think about whether you have been overly harsh and strict or nervous lately. Maybe you were punishing a child. It is also likely that you were too demanding of him. If the child accumulates irritation or excitement, but the opportunity to take the soul is not provided, he may bite his nails. Try to relieve nervous tension in the baby.
The child returns to childhood habits – it means that we could not engender in him the desire to grow up, to grow up. We encouraged him to grow up, but apparently something was not enough – for example, our approval. In this case, it is necessary to reward the child for adult behavior. Sometimes a kind word or a stroke is enough – the main thing is that the child sees that his actions are approved. At the same time, childishness should not be punished, just ignore such moments in the behavior of the baby.
If, by biting his nails, a child gives vent to aggression, let him sometimes freely express his hostility and his anger. Don’t worry about these outbursts. After all, adults also tend to take the soul. If you constantly suppress the free expression of feelings in a child, you will only achieve that aggression will accumulate in him and overwhelm him. Encourage acceptable forms of aggression in sports or team games.
It is easier to wean a child from the habit of nail biting when it first appeared, and not a couple of years later. But at the same time, you need to act correctly, calmly, without showing excessive zeal. Even out of love for a child, we cannot change ourselves, but we can moderate our tendency to punish. Parental pressure on a child almost always develops into reproaches and threats. Rejecting the unwanted impact on the baby, you will achieve excellent results, you can easily prevent or save the child from the bad habit of biting his nails.
Autism and sleep: helping your child
All children have to learn to sleep through the night. However, for children with autism, this can be a difficult (and sometimes seemingly impossible) process. This, in turn, can have a significant negative impact on the entire family. This guide explains what may be causing your child’s sleep problems and what you can do to ensure a restful night for both your child and yourself.
Helping a child overcome a sleep disorder is not an easy task. Most experts recommend seeking advice and support from someone outside the family in such cases. The ideal candidate is a sleep disorder specialist, such as a child psychiatrist or pediatrician. However, getting a referral to the right specialist is very difficult. To get started, you should talk to your doctor or social worker, or contact your local family or early development center.
It can also be helpful to contact the child’s caregivers or teachers to make sure they are aware of the problems and can provide adequate support to the child. They can help you keep a sleep diary, and you can check with them how sleepy or active your child was during the day.
How can sleep disorders be diagnosed?
By one year, most children should be sleeping through the night. If after this age your child regularly cannot fall asleep or sleeps normally for a while and then wakes up abruptly, then this is a sleep disorder. It is important to recognize that short-term sleep disturbances in children often occur after illness, during holidays, holidays such as Christmas, or during periods of acute stress, such as school exams or the illness of a loved one. After such events, the normal sleep pattern should be restored in the child within a few days.
It is also important that your own expectations are realistic: children cannot go to bed early and wake up late. They won’t sleep for more than a certain amount of time. There is no universal standard for how long your child should sleep – the need for sleep is individual for each person. On average, the amount of sleep a child needs per night drops by a quarter of an hour per year until age sixteen. Thus, if a five-year-old child needs eleven hours of sleep per night, then a 16-year-old child will get eight and a half hours of sleep. However, these are not hard numbers, and it is possible that some 16-year-old child needs 10 hours of sleep per night, and some five-year-old child needs seven hours.
If you suspect a sleep disorder in your child and want to determine the level of the problem, keeping a sleep diary may be a first step.
Why keep a sleep diary?
Sleep diaries are useful for several reasons.
They can help establish an unusual sleep pattern. In the example below, Joe sleeps seven hours a day, but he also sleeps when he comes home from school, which then prevents him from falling asleep at night. If this becomes a stable pattern over time, then parents may consider ways to stimulate him after returning from school. By then, he may begin to sleep more at night and less during the day. It is also apparent from the diary that he has the hardest time falling asleep after spending time with his grandmother. This suggests that consistency and routine are very important to Joe.
If you decide to make routine changes or behavior modifications to help your child sleep better, a sleep diary will help you keep track of whether these actions are producing consistent results, sporadic or not.
You can show the sleep diary to professionals who care for your child, including teachers, doctors, or social workers, so they can better understand how your child’s sleep patterns affect his behavior, you, and your family. Often people feel like you’re exaggerating when you say you only get two hours of sleep a night, but you can show them clear sleep records and they’ll be more likely to listen to you.
On some disability claims, you must describe how your child sleeps and how often you need to wake up at night to help them. You may include a copy of the sleep diary with your application.
Some children with autism are able to use a sleep diary as a visual reminder of their sleep problems. You can use it to set rules about when to go to bed and try to sleep, such as giving your child a gold star for every night they stay in bed, plus a small reward if the child stays in bed for three nights in a row.
The sleep diary does not need to follow the format shown here. You can modify the form below to suit your needs. If you don’t have time to write down the details of the baby’s routines, then you can use a twenty-four hour chart and just paint over the entire time the baby sleeps. This will easily demonstrate how much sleep the baby is getting.
What causes sleep disorders?
Problems with going to bed and waking up
The answer depends on the individual. Unfortunately, it seems that almost all children with autism, without exception, suffer from disturbances in their sleep patterns at some point in their lives. Sleep problems can be divided into two main groups: bedtime problems, where the child has difficulty going to bed at the right time, and waking problems, where the child often wakes up in the middle of the night. This section addresses both types of these problems.
We don’t know why children with autism are so vulnerable to sleep disturbances. However, Donna Williams, who has detailed her experience of living with an autism spectrum disorder, speaks in her autobiography about her fear of falling asleep:
“Sleep is not a safe place. Sleep is a place where the darkness will eat you alive. Sleep is a place without color and light. In the dark, you can’t see your own reflection. You can’t afford to get lost in a dream. Sleep will just come and steal your control over yourself. Anything that completely deprives me of control over myself cannot be my friend “- Donna Williams” Someone somewhere.
“I was afraid to fall asleep, I was always afraid. I fell asleep with my eyes open, and this went on for years. It probably didn’t seem very normal. The adjectives “intrusive” and “hunted” are more appropriate. I was afraid of the dark, although I loved the early dawn and sunset ” , – Donna Williams “Nobody in Nowhere”.
These descriptions are subjective and do not necessarily refer to everyone’s experience. However, they suggest that Donna had more trouble getting to bed than waking up. We do not know which problems children with autism most often suffer from, although we do know children who have problems with both.
In Donna’s case, her fear of the unknown kept her from sleeping, and this may be true for some other children with autism. For most children with autism, this is unlikely to be the only explanation. Many children experience restless sleep as a result of several underlying causes.
Problems waking up can in some cases be an extension of problems getting to bed. For example, a child wakes up to go to the toilet, but then finds it difficult to get back to sleep. In young children, problems waking up may indicate that they have not yet developed an adult sleep pattern. Babies wake up every couple of hours to feed, and this pattern may not change immediately. In older children with autism, this may be a manifestation of restless sleep. It can be severe anxiety – which prevents children from deep sleep – or acute nightmares.
Many experts suggest approaches to solving problems with waking up, such as reducing the time at the bedside – when you check if the child is awake, but spend less time on it so that he or she does not start to attract your attention in this way. However, we assume that children with autism rarely have such a motive as attracting the attention of an adult. Instead, awakening problems may require consistent comfort on your part and creativity in meeting your child’s needs.
Social meaning
Children with autism may find it difficult to understand why and when they need to sleep. Problems with social cues (learning what to do and in what order) are very common in autism, and this may mean that your child simply does not see the connection between the fact that the whole family is going to bed and his own need for sleep. .
Some children have difficulty transitioning from sleeping in their parents’ room to sleeping in their own room. This may be due to difficulty with change, but also because the child needs external support regarding bedtime and sleep times.
Melatonin
This is a hormone secreted by the pineal gland and has been shown to regulate sleep patterns in animals. Some studies have shown that taking melatonin supplements can help prevent sleep disturbances after long journeys. Some believe that children with autism produce melatonin at an irregular rate, so that although they produce melatonin, it is produced at the wrong time of day.
In the UK, melatonin products are available on prescription only. For further information on the use of melatonin, you should consult with a specialist. Some foods are rich in melatonin, including: oats, rice, sweet corn, tomatoes, plums, bananas, and Brazil nuts. However, there is still no scientific evidence on whether a melatonin-rich diet can help children sleep better.
Too much information
Children with autism may have serious problems with hypersensitivity to touch, visual stimuli or sounds. This can be both distracting and stressful, which can make falling asleep extremely difficult.
Allergies and food sensitivities
It is possible that, compared to their peers, children with autism may be more sensitive to foods such as sugar, caffeine, and flavors that stimulate the nervous system. If your child often eats sweets or drinks containing caffeine and other foods before going to bed, then you should check if this can interfere with his sleep.
What can we do?
Removing stimulants from the diet
If you already keep a sleep diary, then you will have no problem keeping track of this aspect. If this is not the case, then it is recommended that you at least record when your baby sleeps so that you can reliably identify possible changes.
Changing the bedtime routine can cause a lot of stress for a child, and if he is used to certain drinks or snacks before bed, then a sudden change to something else can do more harm than good. However, you can try switching to decaffeinated drinks, replacing regular chocolate with sugar-free chocolate from a health food store, using plant-based chocolate and cocoa substitutes, switching to sugar-free drinks, or replacing sugar in drinks with fructose or sugar substitutes, which can help some kids.
Or you can try to carefully reduce the dosage of certain foods over days or weeks so that the child consumes less and less sugar and caffeine in general without taking away the usual foods. For example, offer him one cookie instead of two, put half a spoonful of sugar instead of one in his tea, mix drinks with and without caffeine. It will also gradually reduce your child’s sweet taste habit, which will help improve oral hygiene.
Some people advocate radical changes to a child’s diet, such as eliminating sugar and caffeine entirely. We would rather recommend this only if you have already tried the moderate approach. We would suggest that you visit a dietitian before making major dietary changes to ensure your child continues to receive a balanced diet.
Using relaxation techniques
We all find it difficult to fall asleep if we get too excited before going to bed. If a lot happens in life, or our emotions are at their peak, then going to bed will become difficult for us too. Children with autism are often unable to articulate their need to de-stress and relax. In addition, when they go to bed, they may experience great anxiety and confusion.
Relaxation techniques can be started with the most elementary techniques that will not interfere with the normal course of family life. The following are examples of such techniques:
Adding a few drops of lavender oil to baby’s bath. This has been shown to have a sedative effect.
Baby massage. Direct skin contact may be uncomfortable for some children with autism, but some massages, such as shiatsu, can be done through clothing. Gently massaging the feet, hands, or head in the right setting can help calm the baby before going to bed.
An hour of quiet time before the child goes to bed can do two things at once. A quiet and peaceful activity, perhaps involving you or the child’s sibling, will help the child relieve stress and also become an important social sign. If everyone in the house becomes quiet and relaxed, then the child receives a stable message that it is time for bed, which disappears if the house remains noisy and full of life, and the child is expected to sleep. Obviously, the introduction of a quiet period is easier said than done, but you can start small: for example, turn off the TV and computer for an hour. It should take some time before it becomes a routine, but if you succeed, then the effect will not be long in coming. It is also worth introducing this quiet time into the daily routine so that the child knows what to expect and gets used to such a routine.
Many experts warn that formal relaxation techniques can backfire on people with autism, making them stressed rather than relaxed. Some people advocate exercise as a way to relieve stress, and this idea may have some benefits. Physical fatigue of a child is a good way to ensure that he falls asleep! Many children with autism enjoy physical activity and very active play, and while this seems to contradict what has been written above about quiet time at the end of the day, some children may benefit from this approach. It is best for you to know which group your child falls under.
Some parents have found that formal relaxation aids such as music and exercise (eg yoga) are very helpful for their children. These remedies are widely available, and you can judge for yourself what your child responds best to.
Some parents report that installing nightlights in their child’s bedroom has helped.
It may be worth introducing a time in your daily routine when you sit down with your child at the scheduled time and discuss his day or what worries him. Sometimes it is even helpful to have a “worry notebook” or diary to keep next to the bed so that the child can write down or draw any fears and worries in it. Then they need to be discussed before going to bed. Or the child may have a worry box so that he writes down all his worries and locks them in the box.
Establishing a routine
Children with autism respond very well to rigid routines and structure because it makes them feel safe and in control. While sticking to a routine can be annoying throughout the day, setting up a routine that suits your family’s needs and helps your child feel calmer can be extremely beneficial. To do this as effectively as possible, you need to carefully analyze the regime that your family is following at the moment. The following should be taken into account:
Is it possible to have dinner at the same time every evening?
Are you already doing this?
Is it late in the evening or quite early?
Is it possible for a child with autism to take a bath at the same time every night?
Is there anything in your child’s routine that can only be done at home? It can be a wall bars or your own space for time out in the evenings.
Ultimately, the routine should be as simple as possible, but with the potential for flexibility built into it. This means that if you leave, if the child leaves, then the main mode can still be saved. You can try something like:
18.30: dinner
19.00: quiet time
19.15: drink and piece of fruit
19.45: bath
20.25: brush your teeth
20. 30: bedtime/sleep time
7:30 am: wake up/wake up.
In the end, whichever mode you choose, it should be something comfortable for your whole family. It can take several weeks for a child’s sleep pattern to change. It’s best to present the new routine to your child visually, using a timed to-do list, so the child can always figure out what to expect, including getting up in the morning. If it is necessary to change the routine, then this should also be explained visually. It is possible that your child’s schedule needs to be made more detailed so that the child knows with absolute certainty that when you need to go to bed, you need to – draw the curtains, crawl under the covers, turn off the lights, lie down, cover yourself with a blanket.
It may be worth setting aside some time to prepare your child for the next day and his schedule. This may include packing a school bag or making a detailed list/schedule of what needs to be done for tomorrow.
How to make your sleep more comfortable
Donna Williams’ description of sleep sounds like something extremely uncomfortable. If that’s your child’s experience, it’s no surprise if he looks excited when it’s time for bed. However, you can work on the child’s fears to help him.
Some children are very sensitive to light, so even very dim light will prevent them from falling asleep. You can use very thick curtains that will block the maximum amount of light in the child’s room.
Likewise, some parents have found that their children can be awakened by even the slightest noise at night. In addition to general advice, such as thick carpet in the room and tight doors, some parents try a more specific approach. One family found that when their child with autism gets into bed, she is woken up by the sound of clothes as people change in the next room. To solve this problem, they moved her bed to the other side of the room and built shelves and cabinets against the wall between the two rooms to block out the noise. Sometimes even the sound of a computer being turned on is enough to disturb sleep. You can use earplugs or music headphones to block out noise if your child is comfortable wearing them.
Touch sensitivity is extremely common in autism. Some children perceive certain types of touch as physical pain. Temple Grandin (a woman with autism) describes that she was unable to sleep if one of her legs touched the other, and therefore she always wore pajama bottoms, even in the hottest weather. Labels on sleepwear and some fabrics can also cause discomfort. Some children respond well to a weighted blanket that you can make yourself. For example, you can sew a patchwork quilt with pockets that are filled with grain instead of cotton. Blanket pressure can be soothing and works in a similar way to the “squeezing machine” that Temple Grandin invented to learn to tolerate being touched.
It is also worth considering whether the smells in the room, from the street or neighboring rooms can affect people with a heightened sense of smell.
The environment in the room should also be made as comfortable as possible. While some children find it comforting to have a lot of their stuff around them, for others it can only be a distraction. Even the colors of the room or the pictures on the wall can disturb sleep.
Explaining sleep
As mentioned above, it is often difficult for children to understand the need for sleep. The following is a social story (developed by Carol Gray) intended to explain the dream. Please see Social Stories and Comics for more details. Visual aids, such as charts, can be used to explain sleep, as can children’s books containing the biological rationale for the need for sleep.
Here is an example of a social story by Carol Gray (from My Social Stories, 2002):
What does it mean when people say “Bedtime”?
All people are asleep. Most people sleep on Mondays, Tuesdays, Wednesdays, Thursdays, Fridays, Saturdays and Sundays. They wake up every morning.
I sleep in a bed. Usually mom or dad says “It’s time for bed.” This means that you need to go to bed and fall asleep.
Medicines
Medical interventions are normally considered the last resort in treating sleep disorders in children because they can be addictive and they do not treat the underlying cause of the problem. As a general rule, it is best to minimize the use of drugs by the child, but in some cases a mild sedative should be available. For example, if you are going on a trip and are afraid of problems with jet lag, or you are afraid that your child’s overall health is suffering because of poor sleep. Most physicians are willing to prescribe drugs in such circumstances.
Some parents have also found that medications used in tandem with a behavioral approach can restore a good sleep pattern. This combination is critical because, without behavioral intervention, once the child stops taking the medication, they will most likely revert to the old sleep pattern.
Common problems and possible strategies
David Bramble is a consultant psychiatrist who works with CAMHS and specializes in the mental health of children with learning disabilities. He has a long history of interest in children’s sleep issues and has worked with children with autism and their families. He suggests that the following strategies can be tried for the following sleep problems:
Children who insist on parental presence
Gradual abandonment:
Lie next to the child on the bed for three nights
Lie down on a mattress next to your bed for three nights
Move the mattress closer to the door for three nights
Sit on a chair by the bedroom door with the door open for three nights
Sit outside the door, but where the child can see you, for three nights
Sit outside the door, but in such a way that the child cannot see you, for three nights
Sit behind a closed bedroom door for three nights
You can also use social stories to reassure your child that he is safe when he is sleeping or when he is alone in bed.
Night waking
Scheduled waking:
Use a sleep diary to see when your child wakes up at night
Set an alarm for 30 minutes before
Wake up the child and let him go back to sleep
4. If the child does not fall asleep, try to wake him up the next night for 45 minutes, and experiment until you find the optimal time.
Keeping your child awake when it’s time for bed
Sleep restriction:
Use a sleep diary to look at the average number of hours of sleep per night
Calculate 90% of this time, and make it your new sleep time (postpone bedtime and/or wake up time), but never limit sleep to less than five hours
If the child is awake, take him to another room and keep him busy
Avoid daytime/excessive weekend sleep
After a week, start increasing your sleep schedule by 15 minutes at a time – continue this until your desired sleep pattern is achieved.
None of these offers guarantee success. You can combine some of them to get the best results. Tracking your child’s sleep with a sleep diary will likely help you better understand what is causing your child’s sleep problems and help you choose the best solution. If you take advantage of any suggestion, then the problem may get worse before the situation gets better. However, it is important to consistently stick to the chosen method. It is also important to reward and praise your child for improving sleep at night to provide positive reinforcement.
Get enough sleep by yourself
Experts often suggest sleeping at the same time as the child sleeps. However, anyone who cares for a child with a sleep disorder knows how hard it can be in reality. We cannot turn our body on and off like a light bulb. By the time you finally calm your child down to go to bed on your own, you may be too overexcited to fall asleep. Your child may fall asleep at an inconvenient time for you, and if there are other children in the family, they may require your attention when the child with autism falls asleep.
It is very important to be persistent in your need for sleep. Sleep deprivation is an extremely dangerous condition (for example, falling asleep while driving is responsible for 20% of road accidents) and can negatively affect your health and mental well-being. So getting a good night’s sleep is essential, but sometimes it’s easier said than done.
Safety
If your child’s room is safe, your own sleep will also improve. If you go to sleep knowing that nothing will harm your child if he wakes up, then you have already increased your chances of not being disturbed.
In The Parent’s Guide to Survival, Eric Schopler quotes several parents who have approached this issue creatively. One parent installed a double door on a child’s bedroom. If in the evening the child went to bed, but did not sleep, then the parents left the upper part of the door open and the lower part closed.
The child remained in the room, but could easily call his parents. This meant that parents could relax in the evening before going to bed, could check on their child without disturbing them, and could react quickly in an emergency.
My child sleeps too much
If you start keeping a sleep diary, you may find that your child does not sleep too much, but at inappropriate times, such as sleeping in the morning or not wanting to get out of bed on weekends. However, you may also find that your baby actually sleeps longer than you might expect. This condition is called hypersomnia.
There has been very little research into the causes of hypersomnia or how it may affect children with special needs. Medical treatment for this disorder is limited to stimulants such as Ritalin, which is not always effective. We recommend talking to your doctor and asking for advice or a referral to a pediatrician who has experience working with children on the autism spectrum.
However, in the case of children with autism, there may be other reasons why they seem to sleep too much. For example, it may be difficult for a child to get out of bed, but in fact he is not sleeping. Perhaps the bed or bedroom is a place where the child can relax, or it evokes pleasant associations. We all hate to get out of bed at times. However, children with autism may lack the motivation to do so. Potential approaches you can take with this child are similar to those for children who sleep too little:
Try to make your awakening as soft and relaxing as possible. One family began to wake up their son by sending a cat into his bedroom. This meant that the son would get up in a good mood. You can do the same with your child’s favorite toy or hand puppets.
Try playing soft music when your child wakes up.
Use breakfast or another reward to motivate you.
Stick to a rigid routine every day.
However, these are not suitable methods for older children and adolescents, and these young people are more likely to have motivational difficulties in the morning. It is possible, especially in the case of high-functioning autism, that they are afraid of what awaits them today. On the other hand, they may suffer from depression, which affects their motivation. Excessive sleep in this age group can indicate serious psychological problems, and you need to consider this possibility, and not just write off excessive sleep as laziness. Again, sleep monitoring can help establish patterns that indicate potential problems.
What other options are there?
We acknowledge that many of the approaches proposed are not appropriate for all children with autism for a variety of reasons. We also recognize that long-term sleep deprivation may be too bad for parents to effectively implement a behavior modification program if they only think about getting back to bed. For this reason, we would suggest trying to find someone to support you during this period. There are too few professionals who can help parents of children with autism who have sleep disorders. However, you can try to find them through a doctor, a social worker or the child’s school.
You may also find that other parents have been in the same situation and can offer you their own advice and experiences.
All information is taken from open sources. If you believe your copyright has been infringed, please contact
write in the chat on this site, attaching a scan of a document confirming your right. We will verify this and immediately remove the publication.
How to choose a baby pillow and blanket. Our child.
Baby blanket and pillow: down, wool or silk?
Contents:
How to choose a pillow for a crib
Which baby blanket should I buy?
A wonderful time of childhood, new discoveries and the joy of daily knowledge of the world! The task of parents is to make this time cloudless, filled with comfort, coziness, convenience and, of course, health.
Children’s room is a place where a small person spends a significant part of the day playing and relaxing. Young children and preschoolers spend 12-14 hours in bed, including night and daytime sleep. What is needed for a child to sleep soundly, and his sleep to be healthy and of high quality?
The two most important ingredients for good sleep are a pillow and a blanket. It is worth carefully approaching the choice of these products, as there are a lot of nuances that parents should consider.
How to choose a pillow for a crib
Size. Newborn babies do not need a pillow, but older children already need support for the spine in the neck area. There are a number of criteria that a pillow purchased for a small child must meet. Firstly, it is recommended to buy a rectangular product, low and small, corresponding to a narrow bed. Usually, the standard size of models for children offered by manufacturers is 40 × 60 cm. Keep in mind that high and too soft products are not suitable for children, the child’s head should not “fall through” into the pillow.
Fabric and filling. You should pay attention to the material of the cover and pillow fillers. Both must be of high quality and must be from trusted, well-known manufacturers. Don’t skimp on baby sleep accessories.
The fabric of the cover must be chosen very carefully, because only high-quality materials will not irritate the baby’s delicate skin and prevent the baby’s head from sweating. Good options would be natural fabrics: silk or high-quality cotton. These materials are pleasant to the touch, environmentally friendly, hypoallergenic, have good breathability and wear resistance.
Fillers should also be considered taking into account the characteristics of the child’s body. Natural ingredients – down, wool and silk – will be a good choice. However, if the child is prone to allergic diseases, discard downy products and opt for silk pillows. They are completely hypoallergenic, microorganisms and bacteria do not develop in silk. An additional advantage of pillows with silk fibers as a filler is that they are quite low and elastic.
If you need to wash your products frequently, you can consider pillows based on high quality artificial fibers, such as microfiber. Models with this filler can be machine washed at a sufficiently high temperature as often as desired, which solves the issue of hygiene of children’s underwear and accessories.
Please note that the baby pillow needs to be cleaned frequently and should not be used for more than two years.
Which baby blanket should I buy?
Before purchasing a blanket, consider whether it is cold in the children’s room and whether you need to buy a separate warm blanket for the winter, or can you get by with an all-season option at a comfortable indoor temperature throughout the year?
If you really want to be warm in winter, a high-quality duvet in soft white goose down is the best choice. Such a product – warm, airy, softest – is guaranteed to warm at any temperature.
Wool-filled duvets are a versatile option for winter and summer. Wool is good because it has a beneficial effect on the state of the body, has healing properties, and gives dry warmth. Such blankets can be attributed to comfortable all-weather products.
But wool, like down, is loved by dust mites, so you should be careful with such a product if your child suffers from allergic diseases. Wool blankets, like duvets, need to be cleaned and aired more often or subjected to anti-mite impregnation. By the way, leading manufacturers of sleep accessories offer duvets with a special treatment that protects products for several years.
A variant for summer – a duvet with silk filling. Silk has the function of climate control, cools the body of a sleeping child in the heat, creates a comfortable temperature when the room is cool. Those who are prone to allergic manifestations should also take a closer look at such a product, because silk never causes allergies, does not attract dust mites, microorganisms do not multiply in this fiber.
Pay attention to the fabric of the duvet cover. The material must be of high quality, the quality of tailoring must also be on top. Rough seams will cause discomfort to the baby, and in case of dishonest sewing, the filler will begin to crawl out through the holes, the integrity of the product will be broken.
The natural materials used for the covers provide good air circulation and excellent moisture absorption. Cotton, silk and linen do not accumulate static electricity, which poses a significant threat to the health of a modern person and especially to the nervous system of a child.
— Discover a safe space for women to meet, listen and share valuable advice!
The Mothers Community is a safe online community sharing advice on fertility, pregnancy and motherhood through to menopause. Join Community Here —
Why do babies like to sleep on your chest?
Your little one being close to your heartbeat is one of the best feelings in the world.
It’s likely that your infant still associates your heartbeat with comfort, so they wish to sleep on your chest.
These young ones want the familiarity of your breath, voice, and heart in the world just like they had in their mother’s womb.
Take your time and enjoy it, as it won’t last forever. After a while, the babies become more accustomed to the outside world.
The more you bond with your little one during wakeful times through cooing, talking, and singing, the easier the transition will be.
Additionally, babies can feel calmer when they sleep on their parents’ chests.
An experimental study to analyze the sleeping patterns of 16 infants proved that skin-to-skin touching is beneficial.
When babies sleep in cots rather than on their mothers, their hearts were subjected to three times more stress.
Why Do Babies Like To Sleep On Your Chest?
One of the many tough decisions new parents face is whether or not to let their baby sleep in their bed.
Some babies will insist on sleeping with you even if you have already chosen their sleep place!
It is heartwarming to feel the tiny hearts of our babies beating in tandem with ours.
It’s impossible to see social media feeds without an adorable picture of a new-parent couple snoozing chest-to-chest.
The act of holding your arms is sacred but is it safe? It’s sacred, but let’s examine the common questions to help you make the best choice.
1. Is It Safe To Sleep With My Baby On My Chest?
Most studies recommend holding your newborn baby skin-to-skin for at least one hour after birth as a powerful bonding experience.
With one exception – you have to be awake for the rest of the day. SIDS risk increases when you fall asleep while your baby sleeps on you.
According to the American Academy of Pediatrics, newborns should sleep on a firm surface.
They are all recommended if they are free from soft objects such as bedding, bumpers, blankets, toys, cribs, bassinets, and portable cribs.
Infants should always be placed on their backs to sleep to prevent SIDS.
2. When Your Baby Wants To Sleep On Your Chest, What Is The Best Way To Handle It?
#1 Swaddling
Swaddling your baby is an excellent idea if you haven’t already done so.
He has grown accustomed to the snug and comfortable feeling of being in your womb for so many months.
A baby wrapped in a swaddle will recreate that incredible sensation, which will help the child sleep better.
Learn more about swaddling: How Tight Should a Swaddle Be
#2 In bed Co-sleeping
The crib may be “vast” for some babies, so they have difficulty sleeping.
Many families have options for bed-sharing or co-sleeping, using the Dock-A-Tot, a co-sleeper that allows you to sleep with you.
You will feel more secure sharing a bed if your baby sleeps in their bed.
#3 Zip A Dee Zip Is Worth A Try.
A swaddle transition product such as Zipadee-Zip may be able to help swaddle your baby if they are older than four months.
Swaddling your baby when their Moro reflex is still active is a good option.
#4 Be Playful & Rock & Roll Them
It is common for families to use this ‘Rock-N-Play’ method when their children are young.
This technique might be of great use to you if the baby is under four years of age.
Although your baby will become accustomed to sleeping with a rock-n-play, there is a possibility that he will experience problems later.
The only drawback to this method is that it does not have an even and solid surface, so it is not considered the safest of them all.
Consult your doctor if you think the baby isn’t getting enough space to sleep.
#5 Comforting Heart Beating Sounds
Perhaps your baby likes the sound of your heartbeat when they sleep on your chest.
If the baby is sleeping on the mom’s chest, it’s her heartbeat you listened to for many months.
In that case, you might consider using a white noise machine that produces the sound of a heartbeat.
The solution might not be the ultimate miracle, but it may help in some situations.
#6 The Importance Of Sleep Training
When your baby reaches the age of four months, you should start sleep training him.
If there is something wrong with the surface your baby is sleeping on, he will be able to sleep on another surface because he can’t tell the difference between the two.
Babies often need to learn how to fall asleep independently for the first time in another place.
Your baby should not sleep on your chest or co-sleep with you if you smoke or consume alcohol.
Even if the baby was born prematurely or if you are exhausted, you should avoid performing this task.
It is advisable to place him in a crib without blankets or pillows to prevent him from suffocating.
Sleeping in the same room as the baby is the best way to decrease the chance of SIDS.
You can do this by placing the crib beside you so that he is close to you.
Summary
You can feel like you are driving a car without a license when parenting a newborn.
Accidentally falling asleep, though, is a potential danger. Snap a picture to remember those dreamy days and savor those newborn cuddles when you know you won’t nod off!
How do we decide what’s essential and what’s not?
Frequently Asked Questions
Is It Safe For My Baby To Sleep On His Belly If I Watch Him?
Whenever your baby is awake, and someone is watching them, they should have plenty of Tummy Time.
The benefits of supervised tummy time include:
Strengthening your baby’s neck and shoulder muscles.
Building motor skills.
Preventing flat spots on the head.
Is It Possible To Sleep On Your Chest With Newborns On Their Stomachs?
As long as you are awake and alert while your child is napping, letting them sleep on your chest isn’t inherently harmful.
There is no risk of falling asleep or otherwise distracting yourself, ensuring from, to, ensure a safe situation.
Is Sleeping On Their Side A Good Option For Babies?
Once your baby has reached the age of four to six months and has rolled over on its own after being placed on its back, side sleeping is usually safe.
Until your baby is a year old, make sure you put them to sleep on their back.
During the first three months of your baby’s life, tell your pediatrician if you notice a preference for side sleeping.
Iesha Mulla
Iesha is a loving mother of 2 beautiful children. She’s an active parent who enjoys indoor and outdoor adventures with her family. Her mission is to share practical and realistic parenting advice to help the parenting community becoming stronger.
A safe space for women to meet and find support!
The Mothers Community is a place to connect with women who are at a similar stages in life–from fertility, pregnancy and motherhood through to menopause.
Join a community who are there to listen, share information and offer valuable advice. Join Community
Take matters into your own hands! Expert advice for Fertility, Pregnancy and Motherhood! Discover More Here
Is it safe for babies to sleep on your chest?
Decision-making is a crucial aspect of becoming a parent. New parents have to deal with numerous tough decisions, and one of them would be whether or not to let your baby sleep with you. You might have already decided your baby’s place of sleep, but some babies might insist on sleeping with you!
Scroll through any social media feed, and you’re bound to come across at least one adorable pic of a newborn-parent duo snoozing chest-to-chest. As a new mom, we love holding my babes close, feeling their tiny hearts beating in tandem with ours. There’s no doubt this creates a sacred bond with your baby—but is it safe?
There’s a lot of confusion about sleep safety when it comes to newborns. Let’s go over the most common questions so you can make the best choice for your family.
Looking for baby nursery chairs? Look no further. My Baby Nursery have an extensive list to choose from.
Should Infants Be Allowed to Sleep on Your Chest?
Newborn babies should not be allowed to sleep on your chest because this increases the chances of tragedies like SIDS. It is best to establish a rule of not letting your baby sleep on your chest. Letting your baby sleep on your chest, or co-sleeping might seem like a very good way for you to bond with your child, but it can be dangerous. You might be rocking the baby to sleep, but as soon as you lay him, he might wake up. This is why many people let them fall asleep on their chest or co-sleep, but it can be really dangerous for the baby. Apart from increasing the risk of Sudden Infant Death Syndrome (SIDS), it also increases the risk of accidents or suffocation.
Is it Safe to Sleep With My Baby on My Chest?
Holding your baby skin-to-skin is such a powerful bonding experience that it’s recommended by the American Academy of Pediatrics (AAP) for up to an hour after birth. Beyond this time, it’s still considered safe with one exception—you must be awake. The AAP warns that falling asleep while your baby is sleeping on you greatly increases the risk of sudden infant death syndrome (SIDS).
How and Where Should a Newborn Sleep?
According to the AAP, the safest place for newborns to sleep is on a firm surface in their parent’s bedroom. To reduce the risk of SIDS, babies should always be placed on their backs to sleep. Cribs, bassinets, portable cribs, and play yards are all recommended as long as they are free from soft objects like bedding, bumpers, blankets, and toys.
What Can You Do If Your Baby Wants to Sleep on Your Chest?
Swaddling
You should try swaddling your baby if you had not already done this before. He was living in your womb for so many months that he is used to the snug and comforting feeling. Wrapping your baby or swaddling him will help replicate that amazing feeling, which will help your baby sleep well.
Dock-a-Tot
Some babies find the crib to be ‘vast’ to sleep properly. This could be another reason why infants prefer sleeping on their parent’s chest. For many families, bed-sharing or co-sleeping might is an option, and you can use a Dock-A-Tot, an in-bed co-sleeper to help your baby sleep with you safely. This way, you will be able to share your bed safely with your baby.
Zip a dee-Zip
If your baby is more than four months old or if swaddling the baby is not working, then you could try using a swaddle transition product like Zipadee-Zip. This is useful when the baby’s Moro reflex is still strong.
Rock-N-Play
Many families try this ‘Rock-N-Play’ method when their babies are young. If the baby is younger than four years old, then this method might be really helpful for you. However, there are chances that your baby might face problems later since he will be accustomed to sleeping using the Rock-N-Play technique. But note that this method is not considered to be the safest of all the other sleep surfaces since it is not flat and firm. You should check with your doctor if you feel like there is not enough space for the baby to sleep.
Heartbeat While Noise
The sound of your heartbeat might be one of the reasons your baby might like to sleep on your chest. If it is the mom’s chest the baby is sleeping on, then it was your heartbeat the baby listened to for many months. So, you could consider using the white noise machine that has the heartbeat sound. This might not be the ultimate miracle solution, but it might help to a certain extent.
Sleep Training
If your baby is older than four months, then you could try sleep training him. You baby will be capable of sleeping on another surface since he does not know the difference or that there is something wrong with it. Many babies need to learn how to sleep well independently in other spaces.
It is advised not to co-sleep or let your baby sleep on your chest if either you or your partner smoke or consume alcohol. You should not do it even when you are extremely tired or if the baby was born prematurely. It is best to make him sleep in a crib without any blankets or pillows, so the risk of suffocation is reduced. The best way for parents who want to be with their babies while sleeping is to sleep in the same room with them. Place the crib beside you so that he is near you, and this way, you are also decreasing the chances of SIDS.
Helping Babies Sleep Safely
Are you expecting or caring for a baby? Take these steps to help baby sleep safely and reduce the risk of sleep-related infant deaths, including sudden infant death syndrome (SIDS).
There are about 3,500 sleep-related deaths among US babies each year. CDC supports the updated 2016 recommendations for external icon issued by the American Academy of Pediatrics (AAP) to reduce the risk of all sleep-related infant deaths, including SIDS. See How to Keep Your Sleeping Baby Safe: AAP Policy Explained External icon to learn more about these and other actions.
Parents and caregivers can help create a safe sleep area for babies by taking the following steps:
Place your baby on his or her back for all sleep times—naps and at night. Even if a baby spits up during sleep, babies’ anatomy external icon and gag reflex help prevent them from choking while sleeping on their backs. Babies who sleep on their backs are much less likely to die of SIDS than babies who sleep on their sides or stomachs.
Use a firm, flat sleep surface, such as a mattress in a safety-approved crib external icon covered only by a fitted sheet. Some parents and caretakers might feel they should place their baby on a soft surface to help them be more comfortable while sleeping. However, soft surfaces can increase the risk of sleep-related death. A firm sleep surface helps reduce the risk of SIDS and suffocation.
Keep your baby’s sleep area (for example, a crib or bassinet) in the same room where you sleep until your baby is at least six months old, or ideally until your baby is one year old. Accidental suffocation or strangulation can happen when a baby is sleeping in an adult bed or other unsafe sleep surfaces. Sharing a room with your baby is much safer than bed sharing and may decrease the risk of SIDS by as much as 50%. Placing the crib close to your bed so that the baby is within view and reach can also help make it easier to feed, comfort, and monitor your baby.
Keep soft bedding such as blankets, pillows, bumper pads, and soft toys out of your baby’s sleep area. Additionally, do not cover your baby’s head or allow your baby to get too hot. Some parents may feel they should add sheets or blankets to their baby’s crib to help keep their baby warm and comfortable while sleeping. However, sheets, comforters, and blankets can increase the risk of suffocation or overheat your baby. If you’re worried about your baby getting cold during sleep, you can dress them in sleep clothing, like a wearable blanket. In a recent Pediatrics report external icon, CDC scientists and colleagues found that infant suffocation deaths during sleep were most frequently due to soft bedding, such as blankets and pillows.
Babies should sleep in a bare crib.
An astounding 73 per cent of moms in our survey say they have placed at least one item inside the crib with their baby. A blanket was most common (59 per cent), followed by bumpers (35 per cent), stuffed animals (23 per cent), and pillows (8 per cent). All are suffocation hazards for babies one and younger and can increase the risk of SIDS up to five times, regardless of Baby’s sleep position, reports the American Academy of Pediatrics (AAP).
Moms sometimes get a mixed message. “When women walk through a baby store or flip through a catalogue or magazine, they see bumpers, blankets, and stuffed animals, and they think they need to buy them to be good parents.
When setting up your little one’s crib, always remember that bare is best. The only thing you should have in the crib is a fitted sheet. No pillows, no stuffed animals, no sleep positioners or sleep wedges (they pose the same suffocation hazards as pillows), and no crib bumpers, which have been linked to suffocation and strangling of infants.
Always put your baby down to sleep on her back.
Twenty-eight per cent of moms say they have put their baby to sleep on his stomach, a practice that leaves babies at increased risk for SIDS. And of those who take this risk, 47 per cent do it before their baby turns three months old. That’s when the risk of SIDS is highest, in the first four months, associate director of the Sleep Center at the Children’s Hospital of Philadelphia and author of Sleeping Through the Night.
Many of these parents are what we’d call “conscientious objectors. They think that what they’re doing is somehow better or safer than what their pediatrician is telling them.” Parents who are desperate not to hear their baby cry, for example, may find ways to rationalize stomach-sleeping. It’s true, and babies do wake up more easily when they’re on their back. But that may protect them from SIDS. Infants who sleep on their stomach don’t arouse as well, which means they can get in trouble with their oxygen levels and never wake up. ”
Another common justification for stomach-sleeping (for 10 per cent of the rule-breakers) was worry that Baby would choke from reflux. No evidence supports this. Stomach-sleeping is riskier than back-sleeping when it comes to choking concerns.
To ensure safe sleep for babies, make back-sleeping non-negotiable. “The only way you’re going to teach your baby to sleep on his back is to teach your baby to sleep on his back. It’s the same thing as an infant who hates to be in his car seat. He has to be in his car seat.
Finding the right nursing chair for your baby nursery is an important decision. Check out our range of the best nursing chairs at My Baby Nursery.
Be careful with co-sleeping.
Co-sleeping, defined as sleeping on the same surface with Baby, is common, Dr Mindell says. Sixty-five per cent of the moms we polled have slept in bed with their infant, and of those, 38 per cent do so regularly. The majority of these bedsharing moms worry about their baby’s risk of accidental suffocation, but they do it anyway. Why? To help their child sleep, to make nursing easier, to bond with Baby, and because Baby won’t sleep anywhere else, they say.
But bed-sharing is perilous. Studies show that about half of all suffocation deaths among infants happen in an adult bed. Compared with sleeping in a crib, the overall death rate is more than 40 times higher for babies who sleep with a parent. There are multiple dangers in an adult bed that can suffocate Baby, from a less-firm mattress and big pillows to fluffy comforters and extra blankets. Parents also mistakenly believe they’re light sleepers and would wake up if they rolled over on their baby, but that’s not the case in so many tragic instances.
The safest option is putting Baby to sleep in a portable crib in your room. Then, when she’s used to that, move her to a crib in her room. Not only will she be safe, she’ll snooze more deeply. “In one study I conducted, we found that babies who sleep with Mom and Dad wake up twice as often than when they sleep alone. They don’t learn to soothe themselves, and that’s what keeps them up.
Never sleep on the couch with your baby.
A staggering 53 per cent of moms in our poll report they share the couch with their infant, a number that astonished our experts. It’s by far the most dangerous choice because couches can be softer and plusher than an adult bed, and Mom or Dad could accidentally roll over and suffocate Baby. Ironically, some parents think couch-sharing is relatively safe because if they put Baby between their body and the back of the couch, she can’t fall off as she could in a bed. In reality, the child can become trapped between the parent’s body and the couch, and that can be much more dangerous.
As a safety upgrade, bond with your baby before bed, and then put her in her crib. When you’re wiped out or if it’s nighttime, avoid nursing or feeding your baby on the couch. You’re more apt to doze off there than in a less comfy spot. If your sweetie falls asleep and you’re tempted to snuggle her while you browse your Netflix queue, think twice.
Finally, never place a sleeping baby on a couch. About 18 per cent of moms say their baby has slept on a couch alone, but even if you’re awake, it’s never safe. It takes only a minute for suffocation to occur.
Follow these sleep guidelines for naps, too.
As we pored through the comments in our study, one thread stood out: Many moms who wouldn’t dream of putting their baby on his stomach at nighttime do so at naptime. “Parents think that since they’re up and about, they’re watching their baby. But the reality is, you’re in the kitchen, you’re on the computer, and if your baby is having a hard time breathing, it’s silence.”
Research also shows that a baby who is used to sleeping on his back but is periodically put on his belly to snooze is 18 times more likely to die from SIDS. Experts aren’t sure why, but one theory is that babies who nod off on their back most of the time develop motor skills differently and can’t lift their head as easily when they’re on their stomach, which puts them at risk for asphyxiation.
Where’s the Safest Place for Your Baby to Sleep?
Ask anyone how much sleep you’re likely to get after your baby is born, and they’ll all tell you the same thing: “Not much.” But ask where your baby should sleep, and you’ll probably get several different answers. Even professionals can’t agree. The American Academy of Pediatrics (AAP) advises parents not to take their babies with them to sleep at night on the same sleeping surface (called “bed-sharing”) due to the belief that this increases the risk of sudden infant death syndrome (SIDS). The AAP recommends that babies have a separate but nearby place to sleep, such as a crib or bassinet in the parents’ bedroom for at least the first six months and, optimally, for the first year. No research is available to support the notion that it’s safer for babies to sleep alone, or that those who do become more independent than babies who sleep with their parents.
Skin-to-Skin & Rooming In
Since the beginning of time, parents have needed and wanted their new babies close to them. Today we know that this yearning for closeness is a physiological need shared by you and your baby. Studies have shown that newborns who are placed skin-to-skin on your chest right after birth will adjust more easily to life outside the womb, stay warmer, cry less and breastfeed sooner than if your baby is separated from you.
The AAP and Lamaze recommend skin-to-skin care immediately following birth for at least an hour as soon as you are medically stable and awake. Your baby must stay as close to you as possible in the days following birth also. Rooming-in with your baby on a separate sleeping surface, such as a bassinet or crib, allows you to learn your newborn’s needs as well as how to best care for, soothe and comfort them. Rooming-in also offers the best start for breastfeeding. The nearer your baby is to you, the sooner you will make more milk and the more likely you are to breastfeed longer and exclusively. (Experts recommend exclusive breastfeeding—no other foods or liquids—during the first six months of life. )
Check out our range of baby nursery rocking chairs at My Baby Nursery.
Safe Sleep
It’s newborn sleep safety that should concern you most. Always put your baby on their back when you lay them down on a firm surface. This is the best-known SIDS prevention tactic. Keep the bedroom at a temperature you find comfortable when lightly clothed, and dress your baby for sleep the same way. Overheating can be dangerous. Their crib, bassinet or cradle should meet current safety standards and be free of soft bedding, crib bumpers, blankets and plush toys, which are suffocation hazards.
The safest place for your baby to sleep? A place near you. What’s most important is that you and your baby are near each other and get some sleep.
Why Babies (and Parents) Love Cosleeping
We often forget to listen to our intuition. To our gut feeling. We ignore what should come naturally. And nowhere is this truer than when we consider where and how most babies sleep in the Western world.
But, when we trust our evolutionary blueprint and bring our children into our cave to sleep, incredible things can happen. With that in mind, 18 months in, I’d like to share some of my favourite things about why co-sleeping has forever changed the way I parent, for the better.
1. IT FEELS GOOD
Co-sleeping is giving me some of the greatest memories I will have as a mother. Watching my baby sleep curled up in my arms. Waking to his morning smiles and laughter. Hearing “Dada” at 6am. Cinching in and spooning with him in the wee hours of the morning. Absolutely priceless.
2. IT FEELS SAFE
Having co-slept for 18 months, I have never had any concerns for my baby’s safety. I feel reassured knowing that I am next to him if anything happens during the night. When I was pregnant I read about a mother and baby’s natural ability to share sleep cycles. Totally true. I still wake just before my little guy during the night to nurse.
If there was ever an issue with my son’s breathing I’d be far quicker to respond with him lying next to me. Studies have shown that just sharing a room with babies reduces the risk of death due to SIDs or accidents by 50%.
External dangers pose another risk to sleeping babies. From an evolutionary perspective it is one of the top reasons we have evolved to co-sleep as a species. While being attacked by a sabre tooth tiger in the middle of the night may no longer pose a threat, our babies don’t know that. They don’t know they were born in 2014.
And we do have very real dangers in our modern homes which co-sleeping can help to safeguard against. House fires, carbon monoxide and home intruders just to name a few.
3. NO MORE TEARS
A baby’s cry is an alarm. It is supposed to be used for emergencies only. To signal that they are in danger or have a desperate need. When babies are close to their mothers they can use more subtle communication in order to get their needs met. On the rare occasion that my son does cry I know that there is something genuinely wrong and that he needs my attention quickly.
4. IT’S FUN!
Pillow fights, hide and seek, blowing raspberries, climbing all over mum and dad, sucking on dad’s nose and giggles in the dark… we just have so much fun with our little guy in bed with us!
5. IT FEELS NATURAL
The first night we slept in the hospital there was the universal hard clear plastic bassinet next to my bed. I knew that at home I would co-sleep but in the hospital, faced with “Co-sleeping is dangerous!” warnings I felt I should toe the line and place our baby in the bassinet rather than co-sleep.
So I did it and he drifted off to sleep. But I couldn’t sleep. I just lay there watching him, touching his chest to check if he was still breathing. More than anything, after carrying this little guy inside of me for 42 weeks he just felt so far away from me. I felt like part of me was missing… which it was. It lasted less than five minutes before I brought him into bed with me and he hasn’t left yet.
6. IT MAKES BREASTFEEDING EASIER
Co-sleeping has made night nursing SO much easier. When my son is hungry we both half wake up together, he latches on to nurse and we both fall back to sleep. No need to get up. No need to turn the lights on. We both stay warm in bed together, nurse and nod off.
Co-sleeping babies consume on average twice as much breast milk as crib sleeping babies at night. And while I might prefer to nurse more during the day, night time breast milk is different. Night time breast milk contains twice as much growth hormone and significantly more melatonin (a hormone needed to develop circadian rhythms). Breastfeeding and co-sleeping go hand in hand.Most of the time nature can’t be improved on, right?
7. WE ALL GET MORE SLEEP
With no need for our baby to cry and being able to breastfeed so easily in bed we all get more sleep. Granted, my sleep is interrupted, but for me my baby’s needs are more important than a solid eight hour sleep. My husband gets a lot more sleep as my little guy and I barely make a sound as we nurse in the wee hours of the morning.
I am also acutely aware that this time is passing so quickly and that in a blink of an eye my baby won’t be a baby anymore and he won’t want to cuddle up next to me at 2am, so I am savouring every precious moment while I can.
8. I CAN SEE THE RESULTS ALREADY
Our little boy started smiling at 2 weeks, laughing at 4 weeks and hasn’t stopped. He lights up the room and he draws people to him. I am constantly playing second fiddle to him when we are out and about, with strangers talking to him and getting such a buzz out of him smiling and laughing with them.
Even mothers with their own babies love my little guy and ask me why he is so happy all the time. He is an absolute joy, so bright, inquisitive, content and confident.
And, he is growing like a trooper. He was 9lbs 4oz at birth and by 6 weeks he was 14lbs. I will never forget our Scottish midwife saying he is the biggest baby they’ve had in 35 years of practice at 6 weeks.
He may just naturally be a happy baby and he may just naturally gain weight well but as his mum I firmly believe co-sleeping plays a part. He doesn’t need to waste energy crying to get our attention so he can put it directly into growing. And body contact is well known to be even more important than milk in determining growth rates.
9. I FEEL MORE ATTACHED TO MY BABY
Co-sleeping is giving us an extra 12 hours a day to form a secure attachment. An extra 12 hours to make our little guy feel like he is so precious that we hold him as close as we can.
I have read countless articles, books and studies on co-sleeping and they all say that what we are seeing with our son are the expected benefits of co-sleeping.
And I am excited for the future. I want to have a close family. I want my son to trust me. To feel he can come to me with any problem. To know that he is loved and valued and special and for us, co-sleeping is helping us get there. Afterall, it is easier to build strong boys than to fix broken men.
10. I DON’T MIND BEING DIFFERENT
Socially it would be so much easier to follow the crowd. To use a crib. A pacifier. An exersaucer. A walker. To let my baby cry. It sure would make for far easier conversations at mummy groups! But that’s not for me. My only important parenting critic is my son.
All my life I have questioned the status quo, I believe every choice should be made consciously, with knowledge and conviction. I’ve done my research and I’ve experienced co-sleeping first hand and know that for me and my family it is right for us.
While the statistics show that over 50% of families bedshare for at least for part of the night, very few dare admit to it. I’ve had hushed conversations with other mums where they’ve told me their baby sleeps with them, only to be met with sighs of relief when I say we do it all the time and that we recently sold our unused crib on Craigslist.
I used to be selective about who I told we cosleep. I didn’t want to ruffle too many feathers. Maybe I wasn’t 100% confident in my choice, maybe it’s just hard to be the odd one out all the time.
But now that I’m reaping the benefits and know, just know deep down that what we are doing feels right, I am proud to cosleep and I love to share my experiences with others. I hope that in doing so it may give others the courage to try something a little different too.
Do you co-sleep? I’d love to hear your thoughts, comments or experiences.
Sleeping with a baby: pros and cons
Komsomolskaya Pravda
House. FamilyMom and babyMom and baby: Upbringing and development
Anna GERASIMENKO
February 3, 2016 8:00
Discussing whether to put the child in the parental bed
Photo: GLOBAL LOOK PRESS
Nurses warn with undisguised experience in the maternity hospital Accustom to the bed right away! Do not lay next to you, otherwise it will get used! ”
(Indeed, suddenly the child will get used to being close to his mother and sleeping peacefully in safety).
In fact, mother nature dictates the opposite – all newborns at first sleep next to their mother. They eat, sleep, feel calm precisely from the presence of their mother in the immediate vicinity. Where have you seen a cat that puts kittens in a “separate basket”, for example? It’s not just that. The child needs to sleep next to his mother, so as not to worry, to grow and develop calmly.
But the pediatrics of our childhood once, on behalf of Nadezhda Konstantinovna Krupskaya, declared that children should have separate beds. And if he yells and asks for hands – let him yell. Pooret – stop.
To be honest, I couldn’t watch him yelling. I took it in my hands. I laid it on my side. I fed on demand, sometimes midnight. It seemed to me that a child should sleep sweetly at night, and not yell hysterically. Yes, and I myself was easier and more peaceful to sleep together.
After 9 months of quiet life in your belly, the baby feels lonely and restless when his mother is not around. His physiological need is to smell his mother, to hear her voice and the sound of her heartbeat, to which he is so used. Therefore, in your arms the baby is comfortable, warm, he is safe. Many parents have noticed that their child sleeps much better, wakes up less often and cries when they put him under their wing for the night. Psychologists have proven that not only the baby needs co-sleeping. Moms also sleep soundly and sweetly when the baby hugs them with her arms and sniffs on her chest.
However, there are children who sleep well in their own beds and do not even think about their parents. Different kids? Different parents? Let’s discuss all the pros and cons of co-sleeping with children.
PROS
– If you are breastfeeding, sleeping next to your baby will make life easier for you. At night, you can breastfeed your baby without getting up. So the baby will not wake up, and you will not need to make unnecessary movements.
– You rock the child in your arms, put it to bed, and after half an hour he wakes up from fear, finding that his mother is not around. And you have to get up and rock again. If you sleep together, you won’t have to jump up and check how your bunny is doing, is it sleeping, breathing, why is it “quacking”?
– Under your “wing” the child will never freeze.
– When the baby is near, the mother is comfortable and calm, the hormone “prolactin” helps to produce milk, so “sleeping together” will not have problems with lactation. – The baby whimpered, lost the pacifier, threw off the blanket … If you sleep nearby, you will quickly calm him down, without waiting for loud crying or waking up.
– Psychological studies have shown that babies who slept next to their mothers in early childhood have higher self-esteem and fewer fears, they do not experience a deficit of parental love.
Photo: GLOBAL LOOK PRESS
– A child sleeps better next to his mother, because he can smell her, because babies have a very developed sense of smell. And if it smells like mom, then there is no reason to worry!
– In a dream, babies experience everything that happened to them during the day – new rattles, a bird outside the window, mother taught them to take a toy in their hands. And if a child is comfortable in a dream and has nothing to worry about, he has time and an opportunity to comprehend everything new, to “digest”, without being distracted by anything. Therefore, psychologists believe that children who sleep with their parents develop faster.
CONS
– Some mothers are afraid that they will crush the baby in their sleep.
Most likely, their fears are unfounded, because the sleep of a nursing woman is very sensitive, and as soon as the baby squeaks or moves, the mother is already awake! But dad does not have maternal instincts, and he can hurt the baby, turning over in his sleep.
– A baby in a parent’s bed can interfere with the sexual life of spouses, which is why many dads are ardent opponents of heirs on their pillow.
– When the child learns to roll over, he can easily roll off the bed onto the floor, the crib is more secure in this case.
Photo: GLOBAL LOOK PRESS
– Parents are afraid that the child, getting used to sleeping with them, will not want to go to his bed later.
USEFUL ADVICE
If you want to wean your child from sleeping with you, remove one wall from the crib and move the crib close to yours. Gradually begin to accustom the child to sleep there, but at the first request, allow him to crawl to you. Over time, the baby will like to sleep in his bed, because you are still there. And when the baby gets used to it, you can return the wall to its place and gradually move the children’s bed further and further away from your own.
Specialist’s comment
Child psychologist, senior researcher at the Institute of Sociology of the Russian Academy of Sciences Natalya Grishaeva:
– All children are different, and some need to sleep with their mother for a long time, others just need to cuddle up to her in a dream for several months, and still others calmly fall asleep in a separate bed from the first day. Mom needs to try: she put her to bed – she doesn’t sleep, then put her next to her, but you shouldn’t “educate” the baby – she will cry alone in bed and fall asleep! He will fall asleep, he will fall asleep, from fatigue, but the need to be near his mother will not go anywhere and will still soon declare itself in the form of long nightly sobs. But the children, whom their parents put next to them on demand, calmly “leave” to their bed over time, because their “need for a mother” was successfully satisfied.
Age category of the site 18+
Online publication (website) registered by Roskomnadzor, certificate El No. FS77-80505 dated March 15, 2021
Messages and comments from site readers are posted without
preliminary editing. The editors reserve
the right to remove them from the site or edit them if the specified
messages and comments are an abuse of freedom
mass media or violation of other requirements of the law.
JSC “Publishing House “Komsomolskaya Pravda”. TIN: 7714037217 PSRN: 1027739295781
127015, Moscow, Novodmitrovskaya d. 2B, Tel. +7 (495) 777-02-82.
Exclusive rights to materials posted on the website
www.kp.ru, in accordance with the legislation of the Russian
Federation for the Protection of the Results of Intellectual Activity
belong to JSC Publishing House Komsomolskaya Pravda, and do not
be used by others in any way
form without the written permission of the copyright holder.
Acquisition of copyright and contact with the editors: [email protected]
My child does not sleep well – Caring alpha
For a long time I suffered with this topic. Before giving birth, I read everything, and it was written there how much the baby should sleep. Well, when it turned out that everything is completely, completely different with us, I began to read literature, forums, LJ and interview my friends.
And it turned out – there is a quiet, imperceptible to a childless look, a very serious war ! Two completely different positions exist and prove their right to life. Both are defended by mothers very violently. In general, it is known that all discussions of children’s topics are usually very acute.
The first, most common position is that the child should be TEACHED to sleep. The child does not know how to fall asleep on his own, and the training is cruel, with crying, but this is done for the good of the child, and if you do not teach him to fall asleep on his own, then the child will be bad, bad.
At first, I was just surprised when I read the techniques “leave crying for 10 minutes – enter the room, without looking into the eyes of the child, hiss “quiet-quiet-time to sleep” and go out for another 10 minutes”. I firmly knew that this sadism would never affect me.
But Alice did not sleep in the wheelchair, and from the age of three or four she generally began to sleep only with her breast in her mouth. It was very hard to endure, she slept 3-4 sleeps either in my arms, or I lay with her on the bed. At night – constantly with breasts, I was numb, my joints hurt, horror …. But I endured, we fought for breastfeeding and the problem of sleep was the tenth thing.
Society put a lot of pressure on the topic of falling asleep with the breast: “It’s terrible, it’s an addiction, you taught her, someone else can’t put her to sleep!” My colleagues – young mothers – went to clubs and cafes, leaving the child with their grandmother, and I was breast-bound and at some point I myself believed that it was bad.
A neighbor in the dacha came in – a young mother visiting a SPA, with manicure, makeup and big eyes: “Are you holding her in your arms while she sleeps? This is absolutely not normal!”.
And even once I lost my temper: I tried to rock a baby in a backpack without giving a breast. The baby was screaming, I was crying. It was 30 minutes of hell that I will never forgive myself and never forget.
After that, I decided to close the topic and endure it, and wait until something changes on its own.
But when the child grew up to a year old, and at night she still woke up every 40 minutes in search of breasts, I again fell into anxiety – among our familiar children, no one slept like that, mothers were very surprised when they heard about our dream, and everyone repeated in chorus what is it is absolutely not normal that I will soon end up in a psychiatric hospital due to lack of sleep and so on.
And I began to re-read the books again, more thoughtfully and seriously.
And so I read that a child who is used to falling asleep with a breast will search for this breast until school, waking up every change of the sleep cycle, and their cycles are short: 40 minutes in the first year of life, and then a little longer. So it was with us…
And that the brain of such a child does not rest, he sleeps superficially, and the brain will get used to it, and the child will suffer childhood insomnia . And from this the child will grow poorly, because the growth hormone is released only when the child is fast asleep.
And so on and so forth. And it all sounds very convincing. And these books are written by doctors. And if I can still write a couple of them into a group of cruel and not very smart people, then somehow my hand does not rise. For example, Mr. Richard Ferber – really works at the sleep research center in Boston. In theory, the smartest person! Does this mean that everything is really bad with us, and I am harming the child?
And almost all such books/articles condemn co-sleeping. It is written about its danger, about the fact that the mother prevents the child from sleeping, and so on and so forth.
In America and Europe, this approach is practiced everywhere. There is an episode in Desperate Housewives about how a mother taught a little girl to sleep. She left her screaming, went to the neighbors and explained that it was for the good of the child.
A prerequisite for this approach is that the child should fall asleep alone in the room. Mom should say goodnight and leave. And the child – lie down and sleep. I read and could not understand in any way – how can a one-year-old child fall asleep on his own? For what? Is this really necessary? No other way? Otherwise, he will breastfeed until school and all sorts of terrible things will happen?
But when I read, for example, this (by the same Ferber):
“ What problems can arise? Some children are prone to vomiting and react with it to prolonged crying. If vomiting occurs during the self-sleep method, then go to the baby immediately, change his clothes, clean the room, change the bed linen and follow the plan further, as indicated. If you remain calm and confident, the child will quickly understand that vomiting does not affect your decision, and will learn to fall asleep on his own, ”then I felt bad – I could not imagine how I could bring my beloved, desired, tender manual girl to SUCH? Is it normal? It’s generally acceptable – so to scoff at someone who can not fight back, so depends on you? Or am I not understanding something?
Or another quote: “How long can your baby cry? Depends on the specific case. The most persistent, however, usually do not scream for more than 2 hours. Many give up after an hour.”
In LiveJournal this approach is popular in the community Kids . But in the community Lyalechka , on the contrary, there are supporters of the second approach – the child does not need to be taught to sleep, you need to let him fall asleep as he wants, it’s generally good with the breast – there is no need to lull, falls asleep quickly and easily.
But it seemed strange to me. Maybe they are suffering and now want to punish others? After all, this is a completely different life – when you are attached to a child, when you lie in one position all night, when your husband has already forgotten that he has a wife … And now they want the same for others, angry crazy mothers. 🙂
Bowlby’s attachment theory is known in this community. And also about the fact that a baby left without a mother falls into a state similar to sleep, only not very useful – into the so-called energy conservation mode. His heartbeat slows down, his breathing goes astray, etc., but it looks like the baby is sleeping perfectly.
And, of course, in Lyalechka everything is entirely for co-sleeping. For the fact that the child was created by nature to be close to his mother, and only next to her he adequately sleeps, stays awake, lives, and only feeling her close, he can relax and direct his strength to his development. And that separate sleep kills GW. And children really need breastfeeding at least up to a year, and preferably longer.
Two different worlds from which different children come out. Some sleep well and a lot from birth. Someone himself, there are those too! But this post is not about them and not about their happy parents. 🙂 And someone sleeps well in a couple of weeks. Someone screamed just one night, someone only three, and especially stubborn people screamed for two weeks. But this is quickly forgotten, the kids sleep all night without waking up, and their mothers write on the forums: “Everything is fine with us with sleep, which I wish you too! And yes, of course, feeding at night is harmful! It is necessary to replace it with some water, but it is better to wean it off drinking / eating at night. After all, this causes caries! You didn’t know?” (This, by the way, is not so, at the end of the post I will post links to information that refutes this statement).
These forums are read by a mother whose child sleeps badly, breastfeeding, little – and thinks: “What am I doing on this? Why are their children sleeping? And mine will also have caries!”
And he goes to look for articles on the topic “How to teach a child to sleep?”…
Our pediatrician came, whom I trust very much. Said, “Children have such a dream. They get enough sleep and provided breastfeeding every 40 minutes. There is no mother – they do not get enough sleep. This is normal. My 5-year-old son still comes to us every night.”
Another doctor came – my mother’s friend, a pediatric surgeon. Said, “This is absolutely not normal . The child should sleep soundly and for a long time without waking up. Otherwise it’s not normal. My son has slept alone since birth and is great.”
And, of course, the experience of other mothers. So it turns out that those whose children sleep well themselves usually don’t talk much about it, because it seems to be the norm and what to say about it, but we often don’t discuss the fact that the sky is blue.
But who had trouble sleeping , and then they disappeared or their were removed , they love, oh how they love to talk about the fact that before that there was hell, but now heaven. Moms do it with the best of intentions! They want to share their experience, to make life easier for those who are still suffering.
One of my livejournal friends weaned a baby, and he began to sleep a thousand times better, including 40 minutes (that is, waking up every 40 minutes and looking for a breast). And she happily shares this news (well, still, I would be terribly happy too! :)). He writes about this that, they say, the whole point is falling asleep with the breast: as soon as it is removed, the dream improves, the child can oversleep for an hour, and an hour and a half, and two, and even three.
And if my Alice was not absolutely the same age as the son of this friend and I would not see with my own eyes that 40 minutes were also gone for her, despite the fact that her breasts are freely available, what would I think!? Of course it’s in the chest. But that’s not the point. The fact is that the brain grows, the phases of sleep lengthen. And her son lengthened, and my daughter. Regardless of the chest.
However, it should be noted that all the same, a child with a breast wakes up many times more often than one without a breast. More on this later.
Or I was walking in the company of mothers and small children. And how do they feel that I have a dream – a difficult topic (or is it just me that looks simple :))? One came up and said that when her daughter was 14 months old, she left her with a nanny and flew away for 5 days to wean her and teach her to sleep. She arrived, the child is gold, she sleeps, she does not ask for breasts.
This story threw me into a fever. She stands there – such a beauty, well-groomed – and she tells me this. I look at her little girl and try to think of anything but what she went through when she was alone for 5 days. Bowlby has a book, Separation, about the fear of being separated from his mother. I hope that mom doesn’t read it. What now already?
In general, I could not understand in any way – how is it, why is there no consensus, “where is the truth, brother?! ” Are there no studies that provide definitive answers? I have a scientific-medical-psychological approach, and all these articles without references to research are unconvincing. I had to sit down and spend time looking for research.
I found quite a lot of things, including those articles that put everything in its place for me. For those who are interested, read on 🙂
First of all, I checked the names of the authors of the Great Books on sleep training in PubMed. After all, if they are really so great, they should have publications and quotes.
Of all the authors of books on sleep training, there is Richard Ferber. There are a lot of his articles, I rush to read abstracts in horror.
Although my English is bad, but I understand that yes, the man is studying sleep disorders, all sorts of severe cases.
John Bowlby, who studied attachment, of course there is. But who will read the theory of attachment when there are easy articles without links, they say, leave it to yell and you will be happy? Bowlby does not write separately about sleep, but reading from him about sucking seems to me important for any future and young mother.
Next, I found quite a few scientific papers on the subject of sleep. It is clear that there are heaps of them, but getting the entire texts and printing them out is a big job, I do not pretend to be scientific completeness, I was looking for answers for myself and I seem to have found them .
So, a lot of articles with a review of the literature, descriptions of cases of sleep disorders and a bunch of links. They write about the same thing:
This is a description of the sleep process: what it is, its stages.
These are the numbers, that is, the sleep norms for children at different ages.
These are the criteria for sleep disorders, its types and types.
The consequences of sleep disorders and the impact of these disorders on a child’s life.
In short, the situation is like this: the child must sleep a lot, the tables amaze with their numbers, my child has never slept so much. The numbers vary slightly between studies.
Here is a table that seems to be closest to reality (“Disturbances and features of sleep in children”, Medicine 1.2010).
Further, sleep disorders are considered as complex cases, such as apnea, narcolepsy, somnambulism, suffocation, etc., as well as DIFFICULTIES WITH FALLING AND SLEEP MAINTENANCE.
Data on 12-month-old children indicate that if a child wakes up twice during the night, then we can talk about a sleep disorder. (I’m in shock. It seems like complete nonsense. Read on).
I notice that the articles are similar to each other. Both ours and not ours. Actually, I know how these literature review articles are written. They write off each other, roughly speaking.
Next, I see that outdated diagnoses are being used, such as increased intracranial pressure. An article that uses such data ceases to interest me.
However, the picture is still serious. I’m trying to understand how Alice and I, as well as a bunch of moms who feed a child a hundred times a night, have gone so far from science and sleep norms.
I delve into the topic and read the description of specific cases of illness, sleep disorders of patients. I see that the anamnesis is not described anywhere. That is, maybe it is described somewhere, but not in those articles that I managed to dig up and download. That is, it is not indicated what type of feeding the child is on, how he sleeps at home, whether he was taught to sleep alone or not. But this is very important.
I see that the described cases are really severe cases, the child has a serious disease, neurological or mental. Well, like terrible nightmares, etc. The disease affects its development, and this is far from the only problem of such children.
I look at my chubby, happy baby and think something is wrong. Based on the results of such studies, smart uncles draw conclusions about how to sleep. They start from violations and draw a conclusion about the norm. And that’s not how it’s done at all. Sick kidneys cannot have a lot of protein, but healthy ones can. And so on.
Well, then I found two articles that put everything in its place.
One contains a detailed description of the method of sleep research, which is now used all over the world. Called polysomnography . Very good, everyone praises and admires. True: it allows you to take a lot of indicators, to study sleep from all sides, so to speak.
This method is carried out in the laboratory and looks like this (from the article “Polysomnography in the diagnosis of sleep disorders in children”, Russian Bulletin of Perinatology and Pediatrics, 5, 2008):
Of course, babies sleeping with their breasts in their mother’s arms are also examined by this method, I talked with those who had such experience. However, this is done in case of serious violations, and to investigate the norms of sleep in this way – why and who needs it when there are separately sleeping children?
A lot of questions immediately disappeared from me. Is it possible to examine my child in this way? Who has been sleeping with me since birth, who is constantly turning around, looking for breasts, pissing in a basin? No no and one more time no. So you can study someone who is already sleeping separately, who can wake up, drink a bottle and sleep further.
And according to this method of studying sleep, articles are then written about sick children, and who will bring a healthy one to the laboratory?
And mothers read this and become alarmed: my child sleeps differently.
Another article that dotted all the i’s is James J. McCann “Cultural Influence on Infant Sleep”.
The article presents data from statistical studies, indicating the number of subjects. Which makes her extremely attractive to me.
Since what was said in the article is fundamentally different from the heap of material I studied, I want to quote a few quotes (I took the liberty of highlighting a few phrases in bold):
“ studies of clinically “normal” infant sleep-wake cycles. This data continues to be the gold standard against which parents and professionals evaluate infant sleep development, despite significant contextual differences that may render such comparisons unwarranted. Any other organization of sleep, however healthy, is hardly considered.”
“The article presents new data from the field of psychology, which suggests that the need for solitary sleep for the development of “independence” of infants from parents is greatly overestimated. New evidence from the field of biology points to the fact that infant sleep researchers underestimate the importance of breastfeeding and maternal proximity in regulating infant sleep physiology and thus meeting the infant’s nighttime needs. ”
“Heron’s cross-sectional in-depth study (17) found the following trend: children who ‘never’ slept with their parents were less controllable, less happy, and more likely to throw tantrums. Moreover, the scientist found that those children who were never allowed to sleep with their parents were more shy than children who always slept in their parents’ bed all night long (17).”
“In a study of parents of 86 children treated in pediatric and child psychiatry clinics (aged 2-13 years) at military bases (children of military personnel), it was found that teachers rated children who slept with their parents more highly. The main group of psychiatric patients consisted of children who slept alone . “
“ The mother’s body stimulates or triggers mechanisms to regulate a month old baby’s body temperature, breathing, wake cycles, cortisol levels and sleep architecture. All of this is extremely important given that the baby is born neurologically immature and slowly matures outside the womb (38-41)”
In Western culture, as described above, medical practitioners continue to insist on the validity of only one form of sleep, i. e. solitary. All ways to manage children’s sleep come down to reducing contact with parents as early as possible and reducing feedings at night. There is widespread advice to “don’t let babies get used to falling asleep while eating, including while breastfeeding,” “don’t teach a baby to fall asleep when a parent soothes and caresses the baby.” These tips are fundamentally contrary to the very context of the evolution of infant sleep in relation to parental emotions. Today, more and more children are breastfeeding in the United States. If breastfeeding is so widespread, and proving to be biologically correct, according to cross-cultural studies, the current recommendations for sleep management will not only not work, but will even interfere with many mothers.”
“…the infant’s ability to fall asleep spontaneously after a brief awakening during sleep (self-soothing) and the ability to “sleep through the night” at the earliest possible age with minimal parental involvement is still a developmental milestone by which both infants and their parents are judged even in cases where the parents themselves do not consider the ability to “sleep through the night” something important. Using this kind of criteria to evaluate “developmental progress” can do more harm than good, especially if the actual sleep conditions differ from the sleep conditions for which such an assessment is intended.
– Infants sleep at night very differently from formula-fed infants. In turn, the sleep of children who were breastfed for a year or more develops differently than the sleep of children who were fed only for the first three months (15). Oberlander et al. (72) found that infants’ sleep immediately after feeding increased by 46% when they were fed cow’s milk formula alone and by 118% when compared with water or carbohydrates alone.
“In developed countries such as the US, UK and Australia, 35% of children (or one in three healthy children) have difficulty falling or staying asleep after being taught to sleep alone (17, 35, 87). Such a high percentage is an example of the fact that, perhaps, the confidence in the correctness of our expectations and ideas about how children should sleep is unreasonably overstated. This is not evidence of parental incompetence, but rather a lack of flexibility in interpreting and applying the advice given by health professionals.”
“Only a hundred years ago, in a relatively small number of cultures around the world, parents and health care workers were concerned about exactly how babies should be euthanized. And it is only in Western cultures that there is a notion that children need to “learn” to sleep, in this case, alone and without contact with a parent. In most cultures around the world, children’s sleep is something that happens on its own. Harkness et al. write: “…eventually, all normal children around the world will sleep through the night, sleep less as they get older, go to sleep and wake up around the same time as other family members, and…early or late they will learn to fall asleep and wake up without the help of their mothers and fathers. The four main stages of infant sleep behavior are determined by developmental stages” (64). ”
Co-sleeping does not lead to one predictable outcome – positive, harmless or negative. Likewise, there is no one predictable outcome of a solitary dream. The physiological and psychological effects depend on the age of the child, as well as the social, physical, and emotional circumstances surrounding co-sleeping.
The exaggerated fear of strangling or suffocating an infant in its sleep comes in part from the cultural history of the West. Over the past 500 years, many impoverished women in Paris, Brussels, Munich, and London (and many other cities) have confessed to Catholic priests that they strangled their babies in their sleep in order to somehow control family size (94, 95, 96). Led by priests who threatened excommunication, fines, and imprisonment (for murder), parents were forbidden to take their children to their bed. Such historical legacies of Western history probably merged with changing social mores and customs (the birth of such values as privacy, autonomy, individualism) and provided the basis for the philosophical justification of modern cultural beliefs. Based on established cultural beliefs, it is much easier to find the disadvantages of co-sleeping than to address its possible benefits.”
And of course, the chapter on sleep in my favorite book “The Art of Breastfeeding” is very good, there are also references to literature, I also used them. A must read!
In general, I answered my questions. I realized that the architecture of sleep differs in children on breastfeeding and not on breastfeeding, as well as in those sleeping with mom and not sleeping with mom. And this “normative” trajectory of sleep development is not represented by the traditional scientific paradigm. And from here, a bunch of terrible articles and tips for accustoming to sleep. And hence a bunch of moms who heeded this advice. As well as mothers who finished breastfeeding and saw that the child began to sleep better. And giving advice to others.
And that we are talking about sleep disorders only if the disorder really exists. If a child does not sleep enough, his nervous system suffers, if he cannot develop normally, if he is really sick! Here, visits to doctors and even medicines are justified – there are situations that are really serious. But in 99% (a figure from me, approximate) of cases, we are not talking about sleep disturbance. It’s about sleep patterns. And if the baby wakes up to suck on the breast – this is the norm! It is important for mom to get enough sleep, co-sleeping helps, as well as daytime sleep.
I also perfectly understand the force of habit , which also has its place in the topic of sleep. Of course, it is not necessary to teach a child to sleep in his arms if he sleeps himself in a cocoon or crib. No need to accustom to motion sickness (I hope everyone already knows that motion sickness is extremely harmful, and severe motion sickness can cause a stroke in a newborn). You can try to slowly remove the breast from the mouth of a sleeping child and crawl away, leaving your clothes nearby for the smell of your mother. In every possible way try to improve his sleep without a mother, resort to tricks and tricks. All this has its place. There is no place to be accustomed to a separate sleep, accustoming through tears, weaning in order for the child to finally “sleep normally”.
If a child whimpered at night, and his mother put her hand on him, hissed, and he fell asleep – great! (Unless we are talking about the first weeks of the formation of lactation). But if the child is on breastfeeding, he cries, and the mother does not give him breasts at night, but sticks water or cradles – this is a mockery! Because he smells milk, it asks for it, and my mother, having read the forums, does not give breasts. This is terrible: I read a joyful post of one mother who was proud that she weaned a five-month-old girl from falling asleep with her breast; at the same time, the girl gnawed through her mother’s T-shirt in the process of weaning. But we are humans, not animals!
I am very sorry that I was born and gave birth to myself at the turn of the epochs, which still found a huge influence of the approach to children imposed by the totalitarian regime of different countries, including Russia, whose goal was to put a woman into production as soon as possible, and for this not to give she is too attached to her own child. I am sorry that I spent so many nerves and strength worrying about why my child is not sleeping as soundly as I would like, why I cannot put him to bed and go about my business. I’m sorry that one of my grandmothers raised children on a schedule, and the second didn’t raise children at all, but worked, that my grandfather still exhorts me to put my daughter in a crib and accustom her to her, that my progressive mother in the first difficult months of my girl is so I was worried that this was “breast slavery”, that it was impossible to sleep with a breast, that it was too hard for me. I’m sorry that a bunch of kids around the world are doing all sorts of horrors like being left screaming and being taught to sleep.
But, on the other hand, how happy I am that now I have the freedom to choose how I raise my child. The freedom not to believe any nonsense on the net, and also not to believe pseudo-scientific articles. Freedom to access information. And that I have such a mother and such a husband who fully support me – my husband spent a lot of his time helping to research this topic, looking for articles and other information.
And that we spontaneously had a joint dream. I didn’t plan it, I didn’t read the studies. The child so wanted, and so it happened by itself. It seems to me that if it had turned out differently, I would have regretted it later. And my father was so surprised (the doctor, by the way), they say, you can’t sleep with her, it’s dangerous!
My daughter is now 15 months old. And I find it hard to believe that I was once so worried that she falls asleep only with her breast. My God, this is just wonderful! It’s insanely convenient! We don’t have any problems falling asleep.
After a year, she began to give me freedom in the evening – one and a half, or even two hours. Yes, I have never slept for more than two hours. And what of it? I see how important and necessary it is for her to apply at night to her breast.
At the same time, at the age of 15 months, she began to fall asleep at home with her grandmother or father, if I was not around. This happened! Even though it never seemed to happen. Well, in a wheelchair on the street – it’s easy. No nipples, thumb sucking, transient objects, etc.
She falls asleep at home with her breast for a daytime sleep, then sucks herself off and sleeps for an hour on her own – before I could only dream of this. And then you need to seize the moment and stick your chest in her. Then she – we – will sleep for another hour, and she will wake up very pleased and well-rested.
And of course, in general, breastfeeding after a year is a super convenient thing. I always have something that will calm the child, put him to sleep, cure 99% of illnesses. How can you voluntarily opt out?
I’m already silent that despite the fact that my child is very tame, our bodily communication with him is 90% co-sleeping, 8% breastfeeding, and only 2% hug-kissing, go catch her during the day!
Everything goes on as usual, and it just took a lot of time to understand this topic. Of course, in the first months I was simply not up to it. And it would be nice if there was an experienced person nearby, some old woman who remembers how it was in the villages. Where the children all slept together, and in general everyone slept together, the children were carried in their arms, breastfeeding was as normal as sneezing, and no one bothered about accustoming to sleep (the woman just plowed like a horse, and the child grew by itself, holding on to her skirt, and then running barefoot through the dung).
If you have similar problems, if it seems to you that your child will NEVER learn to fall asleep without a breast – let me become that person for you)))
I am not a fan or a masochist, I also want to sleep someday. I will catch the moment when it seems to me that my daughter is no longer so important to breastfeeding. At the same time, I will remember that WHO recommends feeding up to 2 years, and in pre-revolutionary Russia they fed up to 5-7. Someday we will finish with GV and get some sleep (and I will finally smoke a hookah 🙂 ). But for now from 80-90 years (I am an optimist) of my life, I am ready not to get enough sleep for a couple of years in order to give my daughter the most important thing that she needs – breastfeeding and my mother’s carcass nearby. 🙂
And, of course, I’m terribly jealous of those mothers whose babies sleep well from birth, wake up at night to suck once every three hours and sleep on. For me, in this version, it is generally a paradise: for both the child and the mother. Maybe someday heaven or someone there will send me a sleeping baby.
Alexandra Anykina blumavolfovna .
Photo by the author
How do you know if your baby is getting enough sleep? — Dream of a child
All children are different, and therefore it is impossible to attach the same norms to all. Each child needs their own approach, and their own standards. Some children like to sleep more, while others, on the contrary, refuse the next daytime sleep early. So how do you know your baby is getting enough sleep if the sleep rations don’t match the amount of sleep your baby sleeps?
Even if you don’t see the sleep norms and don’t count how much your baby sleeps during the day, but all the criteria that I will describe below coincide with your baby’s behavior – this means that the amount of sleep that he gets is suitable for him. Provided that the baby is getting enough food and is healthy, his behavior during wakefulness and sleep can indicate that he is getting or not getting enough sleep.
Baby is awake according to his age . For each age of babies up to a year there are wakefulness norms. At the same time, at the age of up to 6 months, the range of fluctuations is quite small, because babies still need sleep very much. After this age, the frames are already wider. How does the baby feel while awake? A healthy baby (over 3 months old), who sleeps well day and night, behaves calmly for a significant part of his wakefulness, does not cry all the time he is awake, is able to observe what is happening and concentrate on an interesting subject or activity for a short time. Older babies, who can crawl and/or sit on their own, can keep themselves occupied for a while if their mother is nearby or even sometimes without her presence. If the baby, on the contrary, is very capricious, calm only in his mother’s arms, if she constantly distracts him with something, cannot fix her attention on objects, quickly starts to cry, fidget and get nervous, then this may mean that he does not get enough sleep. Although this criterion is very relative, and it is necessary to study the situation in more detail.
Before a night’s sleep, the baby behaves calmly. Are you familiar with the expression “evening crying”? It is very often confused with evening “colic”, which actually occurs in 5-15% of children. And for the rest, evening whims are associated with the fact that there was too little daytime sleep and / or nighttime sleep. And from this by the evening the child becomes overtired and capricious. Small children can even cry very loudly and for a long time. Therefore, before claiming that the baby has colic, check the number of naps, whether it is age-appropriate, and also make sure you put the baby to bed on time at night.
Baby sleeps well throughout the night . If the baby is overtired, then most likely he will wake you up in the first half of the night (1-2 hours after falling asleep). Such awakenings in the first half of the night are often confused by mothers with the fact that the baby has not been “walking” and are taken to pick it up and play with it, which is by no means necessary. On the contrary, you need to think about early bedtime or increase the time of daytime sleep if its amount is 2-3 times less than recommended for your baby’s age.
The baby has a good appetite, he is gaining weight well . This is a very controversial criterion, since there are many reasons for poor appetite, but poor sleep cannot be ruled out as one of the main ones. If the baby often wakes up at night, sleeps short dreams throughout the day, then he does not have time to “enter” the deep phase of sleep, and his body does not get enough rest, the level of growth hormone in the blood decreases, simply put – it grows more slowly. Because of this, appetite can theoretically decrease, and weight can grow more slowly. Therefore, if the baby does not eat well, you need to think not only about how to increase physical activity, or stimulate his activity more, but also take into account whether he sleeps enough.
Baby sleeps well day and night. If the baby sleeps little, but nevertheless falls asleep for a very long time (more than 30 minutes), or constantly “struggles” with sleep – cries, breaks out, arches his back, turns his head, or actively shows signs of fatigue – yawns, rubs his eyes, and can’t fall asleep – all this may indicate that the baby has already accumulated fatigue or has switched to the so-called hyper-fatigue cycle.







 Most importantly, I had my arms back, in some form or another.
Most importantly, I had my arms back, in some form or another. Note when he woke up, and don’t let him be awake after a certain time period.
Note when he woke up, and don’t let him be awake after a certain time period.


 If you can, you might even want to lightly keep your chest touching hers, as if you’re still hugging and holding her lying down.
If you can, you might even want to lightly keep your chest touching hers, as if you’re still hugging and holding her lying down. But if you notice him squirming once more (or you think he’s about to wake up), use the pacifier again:
But if you notice him squirming once more (or you think he’s about to wake up), use the pacifier again: Then, keep the music on as you put him down and let him sleep. Hopefully, he’ll stay asleep with the music still playing nearby.
Then, keep the music on as you put him down and let him sleep. Hopefully, he’ll stay asleep with the music still playing nearby.

 If you have ever muttered the words through tired lips “My baby will only sleep in my arms “… you can breath a sigh of relief today. We have some time-tested baby sleep solutions that actually work.
If you have ever muttered the words through tired lips “My baby will only sleep in my arms “… you can breath a sigh of relief today. We have some time-tested baby sleep solutions that actually work. When you try to stop, your baby cries and cries.
When you try to stop, your baby cries and cries. 
 Positioning Baby for Success
Positioning Baby for Success
”~Sherry McQuay
 ”~Sherry McQuay
”~Sherry McQuay Place your baby in the swing until eyelids get heavy. Then start removing him earlier and earlier in that process to eliminate the association of sitting up and swinging with sleep.
Place your baby in the swing until eyelids get heavy. Then start removing him earlier and earlier in that process to eliminate the association of sitting up and swinging with sleep. This is a bit controversial since many moms have swaddled for up to 4-5 months as did I. The concern is that your baby would become entangled in the swaddling and not be able to move to breathe. So look at what is happening and what supervision you can give to make your decision.
This is a bit controversial since many moms have swaddled for up to 4-5 months as did I. The concern is that your baby would become entangled in the swaddling and not be able to move to breathe. So look at what is happening and what supervision you can give to make your decision.


 Here’s a breakdown of a few positions that are often very comfortable for babies to sleep in.
Here’s a breakdown of a few positions that are often very comfortable for babies to sleep in. They’ll be able to stay close to you, but you’ll be able to do other things while your baby rests.
They’ll be able to stay close to you, but you’ll be able to do other things while your baby rests.
 As your baby starts to inch into infanthood you may no longer have a baby who wants to be held all night.
As your baby starts to inch into infanthood you may no longer have a baby who wants to be held all night. Plus, it helps your baby adjust during the more difficult sleep cycles and helps them stay asleep longer. A device like the Letsfit White Noise Machine provides an effective option when your newborn won’t sleep unless held.
Plus, it helps your baby adjust during the more difficult sleep cycles and helps them stay asleep longer. A device like the Letsfit White Noise Machine provides an effective option when your newborn won’t sleep unless held. Nils Bergman, a professor of pediatrics at the University of Cape Town, came to this conclusion by tracing the relationship between the joint sleep of a newborn with his mother and his further physical development. The results of the study were published in Daily Mail .
Nils Bergman, a professor of pediatrics at the University of Cape Town, came to this conclusion by tracing the relationship between the joint sleep of a newborn with his mother and his further physical development. The results of the study were published in Daily Mail . 

 Therefore, I would like to urge parents, first of all, to listen to their hearts. If you are a mother, sit under the door of the room where the child is crying, while you are crying yourself – spit on the advisers, hug the child to you and give him your best. Childhood will pass very quickly. You only need to listen to your mother’s heart, ”says the psychologist.
Therefore, I would like to urge parents, first of all, to listen to their hearts. If you are a mother, sit under the door of the room where the child is crying, while you are crying yourself – spit on the advisers, hug the child to you and give him your best. Childhood will pass very quickly. You only need to listen to your mother’s heart, ”says the psychologist.  The first time it happens usually at the age of 9-10 months. The child begins the phase of deep sleep, and joint sleep during this period can play a negative role, since the mother has already developed anxiety. For a child, this is the age at which he is already ready to sleep in his own bed, but not in a separate room. If you see that the baby has longer periods of deep sleep, when he does not wake up for a long time, when he eats less often, then you can already safely transfer him to a separate bed, ”Surkova comments.
The first time it happens usually at the age of 9-10 months. The child begins the phase of deep sleep, and joint sleep during this period can play a negative role, since the mother has already developed anxiety. For a child, this is the age at which he is already ready to sleep in his own bed, but not in a separate room. If you see that the baby has longer periods of deep sleep, when he does not wake up for a long time, when he eats less often, then you can already safely transfer him to a separate bed, ”Surkova comments.  For example, a mother is waiting for the second, say, she will give birth tomorrow, and suddenly she decides that it is time for a two-year-old child to sleep separately. The child immediately moves to the next room through tears and stress. Sometimes it happens that the child slept in a side bed, but suddenly he is told that now he has grown up and this bed is no longer his, but a new brother, and now he needs to sleep on a bunk bed in the next room. In this case, the child has two stresses at once – the appearance of a new child and the selected position that is familiar to him. And sleep is very important. Sleep and food are basic human needs, so it is very important that in childhood they are carried out in a calm environment so that nothing injures the child. It is important to do everything very gradually, ”the psychologist shares his advice.
For example, a mother is waiting for the second, say, she will give birth tomorrow, and suddenly she decides that it is time for a two-year-old child to sleep separately. The child immediately moves to the next room through tears and stress. Sometimes it happens that the child slept in a side bed, but suddenly he is told that now he has grown up and this bed is no longer his, but a new brother, and now he needs to sleep on a bunk bed in the next room. In this case, the child has two stresses at once – the appearance of a new child and the selected position that is familiar to him. And sleep is very important. Sleep and food are basic human needs, so it is very important that in childhood they are carried out in a calm environment so that nothing injures the child. It is important to do everything very gradually, ”the psychologist shares his advice. 
 But the expectation of a beautiful fairy tale of serene parenthood is very often replaced by a harsh reality with sleepless nights, children’s crying and the hope that the colic will soon pass and it will soon become easier. Colic passes, and restless children’s sleep with long bedtimes and frequent awakenings often remains the main problem of young parents. What prevents the child from sleeping at night and how to fix it? Authoritative experts answered this question.
But the expectation of a beautiful fairy tale of serene parenthood is very often replaced by a harsh reality with sleepless nights, children’s crying and the hope that the colic will soon pass and it will soon become easier. Colic passes, and restless children’s sleep with long bedtimes and frequent awakenings often remains the main problem of young parents. What prevents the child from sleeping at night and how to fix it? Authoritative experts answered this question. 

 But there are some general recommendations on how to make a child’s sleep sound and parents’ nights calm.
But there are some general recommendations on how to make a child’s sleep sound and parents’ nights calm. 
 From this age, the baby may wake up suddenly, with anxiety and crying. This is the so-called physiological crying, it is preceded by a shallow sleep. Often the child thus tries to call his parents, without whom he is uncomfortable and anxious. The baby needs to be made clear that the parents are nearby, they will come and calm him down, but without feeding, playing, without taking him out of the crib. Smooth stroking, repetition of ritual elements, soft humming in most cases return the child to sleep. Perhaps some thing in the crib that the baby saw at the parents and which smells of them will help him with this.
From this age, the baby may wake up suddenly, with anxiety and crying. This is the so-called physiological crying, it is preceded by a shallow sleep. Often the child thus tries to call his parents, without whom he is uncomfortable and anxious. The baby needs to be made clear that the parents are nearby, they will come and calm him down, but without feeding, playing, without taking him out of the crib. Smooth stroking, repetition of ritual elements, soft humming in most cases return the child to sleep. Perhaps some thing in the crib that the baby saw at the parents and which smells of them will help him with this.  “Intermediaries” in the form of night toys are effective here, as well as firm beliefs like “See you in the morning, baby.” Nightmares can also be the cause of awakenings. Parents should agree on what strategy to follow when the child wakes up and comes to bed with them.
“Intermediaries” in the form of night toys are effective here, as well as firm beliefs like “See you in the morning, baby.” Nightmares can also be the cause of awakenings. Parents should agree on what strategy to follow when the child wakes up and comes to bed with them.  This is a constant exam of parents for ingenuity and balance for the sake of deep sleep of the baby – the key to the production of somatotropic hormone, which is essential for the growth and harmonious development of the child’s body.
This is a constant exam of parents for ingenuity and balance for the sake of deep sleep of the baby – the key to the production of somatotropic hormone, which is essential for the growth and harmonious development of the child’s body.  It’s hard for these kids to relax. The transition from wakefulness to sleep is difficult for them. As a rule, they sleep restlessly, often waking up.
It’s hard for these kids to relax. The transition from wakefulness to sleep is difficult for them. As a rule, they sleep restlessly, often waking up.  At this temperature, children’s sleep is most profound. If the mother is afraid that the baby will freeze, you can cover the baby with an extra diaper, but do not raise the temperature in the room. Humidity should be 50-70%. High temperature and low humidity of the room lead to the drying of the nasal mucosa, a decrease in immunological protection, the appearance of thirst, which provokes frequent nocturnal awakenings.
At this temperature, children’s sleep is most profound. If the mother is afraid that the baby will freeze, you can cover the baby with an extra diaper, but do not raise the temperature in the room. Humidity should be 50-70%. High temperature and low humidity of the room lead to the drying of the nasal mucosa, a decrease in immunological protection, the appearance of thirst, which provokes frequent nocturnal awakenings.  She is currently researching the biochemical and physiological aspects of breast milk synthesis and release in search of scientific information to help mothers breastfeed longer.
She is currently researching the biochemical and physiological aspects of breast milk synthesis and release in search of scientific information to help mothers breastfeed longer.  1
1  1
1  In other words, the baby does not have to consume more and more milk as they grow older. On the contrary, feedings become shorter and less frequent, but at the same time the child receives the same amount of milk, because he suckles better.
In other words, the baby does not have to consume more and more milk as they grow older. On the contrary, feedings become shorter and less frequent, but at the same time the child receives the same amount of milk, because he suckles better.  Often mothers also worry about sore nipples. The main thing is to find the right position for feeding from the very beginning and ensure that the baby is latching on correctly. Practice shows that this significantly affects the flow of milk and the convenience of feeding.
Often mothers also worry about sore nipples. The main thing is to find the right position for feeding from the very beginning and ensure that the baby is latching on correctly. Practice shows that this significantly affects the flow of milk and the convenience of feeding. 

 If a small child is busy playing they may not always remember to swallow, causing saliva build up.
If a small child is busy playing they may not always remember to swallow, causing saliva build up.  This tongue tie may not have been seen at birth, but as a child ages, it can cause a restriction in movement, leading to difficulty with managing saliva and concurrent speech issues. Tongue ties are not always obvious and a preferred provider in tongue tie can rule assist the speech pathologist in ruling out a restriction.
This tongue tie may not have been seen at birth, but as a child ages, it can cause a restriction in movement, leading to difficulty with managing saliva and concurrent speech issues. Tongue ties are not always obvious and a preferred provider in tongue tie can rule assist the speech pathologist in ruling out a restriction. If you have any questions or confusion feel free to reach out and ask me any questions at This email address is being protected from spambots. You need JavaScript enabled to view it.
If you have any questions or confusion feel free to reach out and ask me any questions at This email address is being protected from spambots. You need JavaScript enabled to view it.
 The doctor should be able to tell you if it’s normal or something of concern.
The doctor should be able to tell you if it’s normal or something of concern.

 Online recipes may look healthy and promise to be nutritionally complete, but they can have too little — or too much — of important nutrients and cause serious health problems for your baby.
Online recipes may look healthy and promise to be nutritionally complete, but they can have too little — or too much — of important nutrients and cause serious health problems for your baby.
 Usually the front bottom two teeth (lower central incisors) emerge first, accompanied by the front top two teeth (upper central incisors). Teething can be a painful and difficult process for both babies and parents, as infants may become especially fussy or cranky while their new teeth emerge. Quintessential signs and symptoms of teething include irritability or fussiness, drooling, chewing on firm solid objects, and sore or sensitive gums. Parents also commonly conclude that teething causes diarrhea and fever, but research has shown this to be untrue. Teething does produce signs and symptoms in the gums and mouth but does not generate constitutional or other extended bodily symptoms. In this baby dental topics article we cover stages of teething and helpful hints. Read more about other pediatric dental topics.
Usually the front bottom two teeth (lower central incisors) emerge first, accompanied by the front top two teeth (upper central incisors). Teething can be a painful and difficult process for both babies and parents, as infants may become especially fussy or cranky while their new teeth emerge. Quintessential signs and symptoms of teething include irritability or fussiness, drooling, chewing on firm solid objects, and sore or sensitive gums. Parents also commonly conclude that teething causes diarrhea and fever, but research has shown this to be untrue. Teething does produce signs and symptoms in the gums and mouth but does not generate constitutional or other extended bodily symptoms. In this baby dental topics article we cover stages of teething and helpful hints. Read more about other pediatric dental topics.
 This will help keep a rash from forming around the baby’s mouth and chin, which can add to the discomfort.
This will help keep a rash from forming around the baby’s mouth and chin, which can add to the discomfort. The same recommendations for stage 2 and 3 can be implemented during this period to keep the baby as comfortable as possible.
The same recommendations for stage 2 and 3 can be implemented during this period to keep the baby as comfortable as possible. The liquid filled kind can break as the baby chews.
The liquid filled kind can break as the baby chews. Before giving the baby any medicines, however, ask the pediatrician what is safe and appropriate for the child.
Before giving the baby any medicines, however, ask the pediatrician what is safe and appropriate for the child. Great!
Great!
 …
…



 Depending on the position of the tooth, some babies may even pull on their ear or rub their cheek when a new tooth is coming in.
Depending on the position of the tooth, some babies may even pull on their ear or rub their cheek when a new tooth is coming in.
 If the teething ring is punctured or cracked, you don’t want to worry about toxic materials.
If the teething ring is punctured or cracked, you don’t want to worry about toxic materials. Usually, the first dentist appointment will happen by 2 years of age.
Usually, the first dentist appointment will happen by 2 years of age. Or is it just me? Amusement aside, it is at this age where bibs and extra cloth wipes are indispensable in your baby essentials. Why? Because of drools.
Or is it just me? Amusement aside, it is at this age where bibs and extra cloth wipes are indispensable in your baby essentials. Why? Because of drools. It also keeps his mouth moistened and protects his teeth in the process.
It also keeps his mouth moistened and protects his teeth in the process. While it is indeed a common cause, it is only secondary to developmental reasons.
While it is indeed a common cause, it is only secondary to developmental reasons. To some parents, excessive drooling beyond infancy can get stigmatizing. When it happens in older children, it is sometimes due to neurological problems relating to low muscle tone.
To some parents, excessive drooling beyond infancy can get stigmatizing. When it happens in older children, it is sometimes due to neurological problems relating to low muscle tone. Salivation to food cues is no different with your developing baby. When you prompt him with food, and he increases drooling, it means he has established his sense of smell. It’s the brain that sends this reaction to help his body prepare for digestion.
Salivation to food cues is no different with your developing baby. When you prompt him with food, and he increases drooling, it means he has established his sense of smell. It’s the brain that sends this reaction to help his body prepare for digestion. So it is good to know that your baby is naturally protected. And it pays to continue breastfeeding and make the most out of its tons of benefits.
So it is good to know that your baby is naturally protected. And it pays to continue breastfeeding and make the most out of its tons of benefits. It prevents demineralization of the enamel once his teeth come out.
It prevents demineralization of the enamel once his teeth come out. Your pediatrician can help you out with the right product.
Your pediatrician can help you out with the right product. 
 Beginning of the functioning of the salivary glands.
Beginning of the functioning of the salivary glands.  They help to neutralize infections that enter the mouth. This is an extremely useful and necessary property of saliva. Starting from 2 months, a small child begins to put everything in his mouth.
They help to neutralize infections that enter the mouth. This is an extremely useful and necessary property of saliva. Starting from 2 months, a small child begins to put everything in his mouth. 

 If, nevertheless, irritation appears on the skin, then cracks and pimples should be lubricated with baby cream or sea buckthorn oil.
If, nevertheless, irritation appears on the skin, then cracks and pimples should be lubricated with baby cream or sea buckthorn oil.  And you will remember with nostalgia this “dribbling period” in the life of your child.
And you will remember with nostalgia this “dribbling period” in the life of your child.  Infants cannot swallow as well as adults
Infants cannot swallow as well as adults 
 Alternatively, you may consider applying an ointment to the affected area at night.
Alternatively, you may consider applying an ointment to the affected area at night.  The body begins to prepare them for this at the age of 2 to 6 months. It is recommended that parents begin offering solid foods to infants at six months of age.
The body begins to prepare them for this at the age of 2 to 6 months. It is recommended that parents begin offering solid foods to infants at six months of age.  However, just because your 3-month-old is drooling doesn’t mean you’ll soon see a tooth pop out. The first tooth usually appears around 6 months of age.
However, just because your 3-month-old is drooling doesn’t mean you’ll soon see a tooth pop out. The first tooth usually appears around 6 months of age.  But they can still have episodes of profuse salivation when they erupt, eat, or play. Salivation usually slows down by about two years of age.
But they can still have episodes of profuse salivation when they erupt, eat, or play. Salivation usually slows down by about two years of age.  Sometimes a sore throat causes a child to drool. If you ever worry about your child drooling, don’t hesitate to contact your pediatrician.
Sometimes a sore throat causes a child to drool. If you ever worry about your child drooling, don’t hesitate to contact your pediatrician. 
 This function is performed by saliva. Bacteria of various viruses can be found on all these numerous objects, and the protective functions of the child are not yet sufficiently formed. Therefore, a lot of saliva in the baby, maybe for a very understandable reason. This is a protective agent, because they have
This function is performed by saliva. Bacteria of various viruses can be found on all these numerous objects, and the protective functions of the child are not yet sufficiently formed. Therefore, a lot of saliva in the baby, maybe for a very understandable reason. This is a protective agent, because they have  Therefore, the appearance of profuse salivation is a normal phenomenon.
Therefore, the appearance of profuse salivation is a normal phenomenon.  They work constantly, producing up to two liters of fluid per day in an adult.
They work constantly, producing up to two liters of fluid per day in an adult. 
 They will determine whether drug therapy is needed in this case or whether this moment can be waited out.
They will determine whether drug therapy is needed in this case or whether this moment can be waited out.  In the oral cavity under the tongue, on the inside of the cheeks, behind the lower teeth are the salivary glands. They work constantly, producing up to two liters of fluid per day in an adult.
In the oral cavity under the tongue, on the inside of the cheeks, behind the lower teeth are the salivary glands. They work constantly, producing up to two liters of fluid per day in an adult. 
 Hence the complaints of parents about increased salivation in babies.
Hence the complaints of parents about increased salivation in babies. 
 This is due to the fact that the salivary glands in babies under the age of one year are still being formed. You should not worry about this, the baby is growing and soon the work of the salivary glands will be established, and the profuse salivation will stop.
This is due to the fact that the salivary glands in babies under the age of one year are still being formed. You should not worry about this, the baby is growing and soon the work of the salivary glands will be established, and the profuse salivation will stop. 

 This becomes the norm by the age of one and a half months, simultaneously with the increasing activity of the salivary glands. If the baby has profuse salivation and there is no other evidence that teeth are really climbing, the possibility of allergic rhinitis, infections of a bactericidal or viral nature, as well as birth defects cannot be ruled out. Then you need to consult a pediatrician.
This becomes the norm by the age of one and a half months, simultaneously with the increasing activity of the salivary glands. If the baby has profuse salivation and there is no other evidence that teeth are really climbing, the possibility of allergic rhinitis, infections of a bactericidal or viral nature, as well as birth defects cannot be ruled out. Then you need to consult a pediatrician.  However, the process of swallowing the child can only be carried out during feeding; in another state, he still does not know how to swallow saliva. So, if a baby at 3 months plentifully lets them in, you should not worry: he will soon learn to “communicate” with saliva.
However, the process of swallowing the child can only be carried out during feeding; in another state, he still does not know how to swallow saliva. So, if a baby at 3 months plentifully lets them in, you should not worry: he will soon learn to “communicate” with saliva.  Gradual increase in saliva production. It is characterized by constant secretion of transparent liquid saliva from the oral cavity.
Gradual increase in saliva production. It is characterized by constant secretion of transparent liquid saliva from the oral cavity. 
 Therefore, saliva flows out on its own.
Therefore, saliva flows out on its own. 
 Bibs will help even now: the fabric absorbs liquid, blouses remain dry, the skin on the neck and breast is also dry.
Bibs will help even now: the fabric absorbs liquid, blouses remain dry, the skin on the neck and breast is also dry.  But to provide proper hygienic care when the baby is drooling is necessary in order to prevent irritation of the baby’s delicate skin. Followed by:
But to provide proper hygienic care when the baby is drooling is necessary in order to prevent irritation of the baby’s delicate skin. Followed by: 
 See a doctor, eliminate the cause, and the amount of saliva returns to normal.
See a doctor, eliminate the cause, and the amount of saliva returns to normal.  If the crumbs have problems of an endocrine nature or in the adrenal cortex, saliva analysis will show the disease. To obtain accurate data, saliva is taken for analysis several times during the day. It is not difficult, painless, will show the right result.
If the crumbs have problems of an endocrine nature or in the adrenal cortex, saliva analysis will show the disease. To obtain accurate data, saliva is taken for analysis several times during the day. It is not difficult, painless, will show the right result. 
 If surgery or radiation is required, then you should be aware that this can lead to abnormalities in the form of caries and facial asymmetry. All decisions about treatment are always made deliberately, the most appropriate method is chosen based on the individual characteristics of the child and expediency.
If surgery or radiation is required, then you should be aware that this can lead to abnormalities in the form of caries and facial asymmetry. All decisions about treatment are always made deliberately, the most appropriate method is chosen based on the individual characteristics of the child and expediency.  As a rule, the baby does not know how to swallow saliva, so it seems to the mother that there are too many of them.
As a rule, the baby does not know how to swallow saliva, so it seems to the mother that there are too many of them. 
 5 (!!!) liters.
5 (!!!) liters.  This condition may be the cause of ptyalism;
This condition may be the cause of ptyalism;  In this case, salivation is accompanied by a number of other signs; when taking lithium-containing drugs, ptyalism is noted as a side effect.
In this case, salivation is accompanied by a number of other signs; when taking lithium-containing drugs, ptyalism is noted as a side effect.  Language becomes a kind of communication tool. Seeing that the baby stuck out his tongue, it can be assumed that he is hungry or wants to be paid attention to. Another reason is that the baby is sick and his health leaves much to be desired.
Language becomes a kind of communication tool. Seeing that the baby stuck out his tongue, it can be assumed that he is hungry or wants to be paid attention to. Another reason is that the baby is sick and his health leaves much to be desired.  The test is carried out in the hospital, a blood sample is taken from the baby from the heel.
The test is carried out in the hospital, a blood sample is taken from the baby from the heel. 

 In the process of treatment, the functions of blood circulation are improved. In addition, special gymnastics, a massage procedure and taking vitamins are prescribed.
In the process of treatment, the functions of blood circulation are improved. In addition, special gymnastics, a massage procedure and taking vitamins are prescribed.  Having found alarming signs, it is worth paying a visit to the pediatrician, who will make an accurate diagnosis and prescribe treatment.
Having found alarming signs, it is worth paying a visit to the pediatrician, who will make an accurate diagnosis and prescribe treatment. 
 Sincerely, the management of OOO “DDC”
Sincerely, the management of OOO “DDC”  on breastfeeding, on complementary foods (banana, apple, fruit puree) rarely goes for a long time, maybe 3-4 days or more, then we put a candle – we went, and then we wait again. Please tell me what to do?
on breastfeeding, on complementary foods (banana, apple, fruit puree) rarely goes for a long time, maybe 3-4 days or more, then we put a candle – we went, and then we wait again. Please tell me what to do? 
 Third day dark green stools. A little temperature. And drooling due to teething. Please tell me why a child can have green stools? And what to us analyzes to hand over?
Third day dark green stools. A little temperature. And drooling due to teething. Please tell me why a child can have green stools? And what to us analyzes to hand over?  When washed, it feels like particles of sand. Meals are separate, canned by age. A mixture of 600 ml per day. The chair is not hard, but decorated.
When washed, it feels like particles of sand. Meals are separate, canned by age. A mixture of 600 ml per day. The chair is not hard, but decorated.  More information is needed about the child, the disease, whether there has been such a situation for all 5 years, whether there have been episodes of remission, etc. Consultation with a gastroenterologist, neurologist, and also a psychiatrist is necessary.
More information is needed about the child, the disease, whether there has been such a situation for all 5 years, whether there have been episodes of remission, etc. Consultation with a gastroenterologist, neurologist, and also a psychiatrist is necessary.  At this age, it is extremely important to know how the pregnancy, childbirth, the presence of infection, hypoxia, etc. proceeded. At the same time, I will give some standards for 1.5-2 month old children. Lateral ventricles: anterior horns up to 4 mm, occipital horns up to 15 mm, body 2-4 mm. Third ventricle up to 5 mm, fourth ventricle up to 4 mm, interhemispheric fissure 2-4 mm, large cistern up to 6 mm, subarachnoid space up to 2 mm. Of course, it is important to note that individual sizing is possible.
At this age, it is extremely important to know how the pregnancy, childbirth, the presence of infection, hypoxia, etc. proceeded. At the same time, I will give some standards for 1.5-2 month old children. Lateral ventricles: anterior horns up to 4 mm, occipital horns up to 15 mm, body 2-4 mm. Third ventricle up to 5 mm, fourth ventricle up to 4 mm, interhemispheric fissure 2-4 mm, large cistern up to 6 mm, subarachnoid space up to 2 mm. Of course, it is important to note that individual sizing is possible.  For a young child, even minimal complaints can be the first signs of a serious bowel problem.
For a young child, even minimal complaints can be the first signs of a serious bowel problem. Studies show that a similar reaction occurs due to dreams. In addition, babies in this way check the presence of parents nearby, instinctively looking for your protection and support. And if he doesn’t find her, he starts to cry for real. Of course, this requires your intervention.
Studies show that a similar reaction occurs due to dreams. In addition, babies in this way check the presence of parents nearby, instinctively looking for your protection and support. And if he doesn’t find her, he starts to cry for real. Of course, this requires your intervention. 
 Primary – by adjusting behavior patterns during the period of falling asleep. Let’s see how to do it.
Primary – by adjusting behavior patterns during the period of falling asleep. Let’s see how to do it.  This is a certain item that is next to the baby during sleep. For babies, this is, for example, a diaper that keeps the mother’s smell, and for those who are older – a favorite toy. All this gives children a sense of comfort and suppresses the excitement during awakenings, and also allows you to feel your closeness.
This is a certain item that is next to the baby during sleep. For babies, this is, for example, a diaper that keeps the mother’s smell, and for those who are older – a favorite toy. All this gives children a sense of comfort and suppresses the excitement during awakenings, and also allows you to feel your closeness.  Feeding in the evening should occur clearly before bedtime. This will develop a certain reflex in the child.
Feeding in the evening should occur clearly before bedtime. This will develop a certain reflex in the child.  Petersburg. To make an appointment, please call 8(812)677-0-777. A professional sleep specialist will advise you on all your questions and select the most convenient time for your visit.
Petersburg. To make an appointment, please call 8(812)677-0-777. A professional sleep specialist will advise you on all your questions and select the most convenient time for your visit.  In order for lactose to be absorbed, the lactase enzyme must break it down, but if the child has little or no lactase enzyme, then lactose is not broken down and remains in the intestine. As a result, there is always a large amount of milk sugar in the intestines, which begins to ferment, and where there is fermentation, conditionally pathogenic flora actively reproduces. What we feel during fermentation: intestinal motility increases (it rumbles), plus gas formation increases (the stomach swells). But in an adult, this is usually a one-time situation due to some inaccuracies in nutrition, and it quickly passes. But in babies, everything is different, especially since they lack the enzyme not once, but constantly. What it looks like: The milk sugar lactose retains water, hence loose stools. In the child’s stomach, “rumbles and boils”, colic begins, the stool becomes frothy, greens, mucus and even blood may appear in it. If at first the stool was liquid, then constipation appears, and all this changes in a circle: yesterday there was diarrhea, today and tomorrow there is no stool at all, the day after tomorrow it is liquid again.
In order for lactose to be absorbed, the lactase enzyme must break it down, but if the child has little or no lactase enzyme, then lactose is not broken down and remains in the intestine. As a result, there is always a large amount of milk sugar in the intestines, which begins to ferment, and where there is fermentation, conditionally pathogenic flora actively reproduces. What we feel during fermentation: intestinal motility increases (it rumbles), plus gas formation increases (the stomach swells). But in an adult, this is usually a one-time situation due to some inaccuracies in nutrition, and it quickly passes. But in babies, everything is different, especially since they lack the enzyme not once, but constantly. What it looks like: The milk sugar lactose retains water, hence loose stools. In the child’s stomach, “rumbles and boils”, colic begins, the stool becomes frothy, greens, mucus and even blood may appear in it. If at first the stool was liquid, then constipation appears, and all this changes in a circle: yesterday there was diarrhea, today and tomorrow there is no stool at all, the day after tomorrow it is liquid again. And the most unpleasant thing is endless colic and endless crying, there is no rest for both the parents themselves and the baby. Mom at some point notices that the baby is crying just after feeding, and then a variety of advice falls upon her. “Your milk is bad, better give the mixture,” says the beloved mother-in-law. “Only breasts and nothing else!” – advise breastfeeding gurus. As a result, the mother tries one thing or the other, but neither breast milk nor artificial mixture gives relief to the child. Colic, crying and problems with the stomach and stool continue. The parents are in a panic because they don’t understand what is going on. In fact, this is a typical picture of bright lactase deficiency (LN), or insufficient production of the lactase enzyme.
And the most unpleasant thing is endless colic and endless crying, there is no rest for both the parents themselves and the baby. Mom at some point notices that the baby is crying just after feeding, and then a variety of advice falls upon her. “Your milk is bad, better give the mixture,” says the beloved mother-in-law. “Only breasts and nothing else!” – advise breastfeeding gurus. As a result, the mother tries one thing or the other, but neither breast milk nor artificial mixture gives relief to the child. Colic, crying and problems with the stomach and stool continue. The parents are in a panic because they don’t understand what is going on. In fact, this is a typical picture of bright lactase deficiency (LN), or insufficient production of the lactase enzyme. The diagnosis is made in the maternity hospital or in the first days after birth, the child does not have lactase at all, he quickly loses weight, he is immediately started to be fed intravenously or through a tube. Some experts (but not doctors) on breastfeeding read once that congenital lactase deficiency is an extremely rare disease, and that’s all – they further began to assure young mothers: “In fact, LN is extremely rare, you don’t have it, you don’t need to listen to doctors “, etc. Yes, congenital LN is a rare disease, but the key word here is “congenital”, and there are other types of lactase deficiency.
The diagnosis is made in the maternity hospital or in the first days after birth, the child does not have lactase at all, he quickly loses weight, he is immediately started to be fed intravenously or through a tube. Some experts (but not doctors) on breastfeeding read once that congenital lactase deficiency is an extremely rare disease, and that’s all – they further began to assure young mothers: “In fact, LN is extremely rare, you don’t have it, you don’t need to listen to doctors “, etc. Yes, congenital LN is a rare disease, but the key word here is “congenital”, and there are other types of lactase deficiency.  Therefore, such a LN is called “transient”, that is, temporary, or passing. It passes for someone a month after birth, for someone longer – after six to seven months, and there are children in whom lactase deficiency completely disappears only by the year.
Therefore, such a LN is called “transient”, that is, temporary, or passing. It passes for someone a month after birth, for someone longer – after six to seven months, and there are children in whom lactase deficiency completely disappears only by the year.  The symptoms are the same as in babies: he drank milk and after that the stomach rumbles, boils, and the stool is liquid. Sooner or later, a person realizes that milk is not his product, and simply stops drinking it in its pure form.
The symptoms are the same as in babies: he drank milk and after that the stomach rumbles, boils, and the stool is liquid. Sooner or later, a person realizes that milk is not his product, and simply stops drinking it in its pure form. Some children lack the enzyme quite a bit, so their colic is mild and children cry quite normally. Plus, the violation of the stool is also not very bright: there are a couple of times a slightly liquefied stool, but that’s all. In other children, the lack of lactase is more pronounced, the child does not cry, but simply yells after each feeding, if at first he gained weight well, then after two months the increase is minimal, problems with stools begin in parallel (day – constipation, day – diarrhea), stool sometimes green, sometimes with mucus. Atopic dermatitis appears on the skin (the skin is the first to react to problems with the gastrointestinal tract). Parents have no rest day or night: the baby cries – he is fed – he cries again, they try to calm him down in other ways. But nothing helps. Mom and dad are in a panic, and no one has the strength anymore.
Some children lack the enzyme quite a bit, so their colic is mild and children cry quite normally. Plus, the violation of the stool is also not very bright: there are a couple of times a slightly liquefied stool, but that’s all. In other children, the lack of lactase is more pronounced, the child does not cry, but simply yells after each feeding, if at first he gained weight well, then after two months the increase is minimal, problems with stools begin in parallel (day – constipation, day – diarrhea), stool sometimes green, sometimes with mucus. Atopic dermatitis appears on the skin (the skin is the first to react to problems with the gastrointestinal tract). Parents have no rest day or night: the baby cries – he is fed – he cries again, they try to calm him down in other ways. But nothing helps. Mom and dad are in a panic, and no one has the strength anymore.  Only an experienced pediatrician will be able to figure out why the baby has colic or green stools, what the numbers in the tests say, and what is the norm for one baby and the pathology for another. And of course, it is not necessary to cancel breastfeeding and immediately prescribe lactose-free or low-lactose artificial mixtures (even as a supplement). By itself, milk sugar lactose is very necessary for a child, when lactose is broken down, its components (glucose and galactose) go to the development of the brain, retina, for the life of normal intestinal microflora. So do not completely eliminate this sugar, you need to help it break down. With a strongly pronounced LN, the missing enzyme is given before each feeding (it has long been learned to produce and it is sold in pharmacies), with a dim clinic, its dose can be reduced. And it is also possible that there is lactase deficiency (even according to tests), but it does not need to be treated, there are almost no symptoms.
Only an experienced pediatrician will be able to figure out why the baby has colic or green stools, what the numbers in the tests say, and what is the norm for one baby and the pathology for another. And of course, it is not necessary to cancel breastfeeding and immediately prescribe lactose-free or low-lactose artificial mixtures (even as a supplement). By itself, milk sugar lactose is very necessary for a child, when lactose is broken down, its components (glucose and galactose) go to the development of the brain, retina, for the life of normal intestinal microflora. So do not completely eliminate this sugar, you need to help it break down. With a strongly pronounced LN, the missing enzyme is given before each feeding (it has long been learned to produce and it is sold in pharmacies), with a dim clinic, its dose can be reduced. And it is also possible that there is lactase deficiency (even according to tests), but it does not need to be treated, there are almost no symptoms.  They see the cause of all problems with the child’s stomach and stool either in the wrong technique of breastfeeding, or partially admit that there is immaturity of the enzyme, but this is natural and will pass by itself. Yes, for some, LN is expressed easily and will pass quickly, but what about those parents whose child yells day and night, covered with a crust from atopic dermatitis and stopped gaining weight? Wait for the time to come and the enzymes to mature? Alas, with pronounced lactase deficiency (even if transient), enterocytes (intestinal cells) often suffer, so it is simply necessary to help such a child.
They see the cause of all problems with the child’s stomach and stool either in the wrong technique of breastfeeding, or partially admit that there is immaturity of the enzyme, but this is natural and will pass by itself. Yes, for some, LN is expressed easily and will pass quickly, but what about those parents whose child yells day and night, covered with a crust from atopic dermatitis and stopped gaining weight? Wait for the time to come and the enzymes to mature? Alas, with pronounced lactase deficiency (even if transient), enterocytes (intestinal cells) often suffer, so it is simply necessary to help such a child.
 And of course, guests are expected to bring a shower-appropriate gift.
And of course, guests are expected to bring a shower-appropriate gift. Items such as diapers, baby clothes, toys, breast pumps, and luxury items for the mom are all common baby shower gifts.
Items such as diapers, baby clothes, toys, breast pumps, and luxury items for the mom are all common baby shower gifts. While traditional baby shower food may consist of dainty finger foods and pink and blue baby-themed treats, you may also want to have more substantial eats prepared at a co-ed baby shower.
While traditional baby shower food may consist of dainty finger foods and pink and blue baby-themed treats, you may also want to have more substantial eats prepared at a co-ed baby shower.

 ” But they sound so much better than the traditional one that it could be time to retire the classic baby shower.
” But they sound so much better than the traditional one that it could be time to retire the classic baby shower.
 It might be too hard to explain to Aunt Linda why all of your husband’s friends are drinking beer out of baby bottles. But with their surge in popularity it is likely you’ll be invited to one soon. RSVP “yes.”
It might be too hard to explain to Aunt Linda why all of your husband’s friends are drinking beer out of baby bottles. But with their surge in popularity it is likely you’ll be invited to one soon. RSVP “yes.” Every day the participants warmed up under warm water. The first group then took a 30-second cold shower. Participants from the second group stood under him for a minute, and from the third – 90 seconds. The fourth group (control) simply enjoyed the heat. The experiment lasted a month. All groups, except for the control group, were offered an optional extension of the practice for another 2 months. 64% of the subjects agreed because they liked it.
Every day the participants warmed up under warm water. The first group then took a 30-second cold shower. Participants from the second group stood under him for a minute, and from the third – 90 seconds. The fourth group (control) simply enjoyed the heat. The experiment lasted a month. All groups, except for the control group, were offered an optional extension of the practice for another 2 months. 64% of the subjects agreed because they liked it.  Cold water causes blood to flow more actively to the organs in order to warm them. In addition, cooling is stressful for the body, leading to the release of adrenaline. Warm water reverses the effect: blood rushes to the surface of the skin. This is how a kind of “gymnastics” takes place, which strengthens the heart and blood vessels.
Cold water causes blood to flow more actively to the organs in order to warm them. In addition, cooling is stressful for the body, leading to the release of adrenaline. Warm water reverses the effect: blood rushes to the surface of the skin. This is how a kind of “gymnastics” takes place, which strengthens the heart and blood vessels. 
 However, such a procedure will definitely become your faithful assistant in maintaining harmony.
However, such a procedure will definitely become your faithful assistant in maintaining harmony. 


 In gynecology, the ascending shower is used in the complex treatment of chronic inflammatory diseases of the female reproductive system, primary and secondary infertility, and menstrual dysfunction. In urology, the appointment of this type of balneotherapy is indicated for chronic prostatitis, impotence, neurological disorders with impaired sexual function. A course of treatment with an ascending shower is recommended for hemorrhoids, fissures in the anal region, inflammation of the rectum, chronic atonic constipation. For children, an ascending shower is prescribed for nighttime urinary incontinence.
In gynecology, the ascending shower is used in the complex treatment of chronic inflammatory diseases of the female reproductive system, primary and secondary infertility, and menstrual dysfunction. In urology, the appointment of this type of balneotherapy is indicated for chronic prostatitis, impotence, neurological disorders with impaired sexual function. A course of treatment with an ascending shower is recommended for hemorrhoids, fissures in the anal region, inflammation of the rectum, chronic atonic constipation. For children, an ascending shower is prescribed for nighttime urinary incontinence. 

 Getting little ones used to these practices when they’re young can mean a lifetime of better sleep habits.
Getting little ones used to these practices when they’re young can mean a lifetime of better sleep habits.



 This often occurs when a baby rolls into something that obstructs their breathing like loose bedding or plush toys that they can roll off of, but some babies are found after sleeping face down which adds another layer of danger.
This often occurs when a baby rolls into something that obstructs their breathing like loose bedding or plush toys that they can roll off of, but some babies are found after sleeping face down which adds another layer of danger. Sleeping face down increases the risk of sudden infant death syndrome (SIDS).
Sleeping face down increases the risk of sudden infant death syndrome (SIDS). If you have any questions please leave them in the comment section below and we will get back to you as soon as possible.
If you have any questions please leave them in the comment section below and we will get back to you as soon as possible. 1 Understand Your Baby’s Development
1 Understand Your Baby’s Development They exhale carbon dioxide into the space in which their faces rest and cannot take in oxygen. Experienced babies lift their heads and turn them, while babies who are new to stomach sleeping lift their heads up and put them right back down into the carbon dioxide. Without oxygen, they suffocate. This tragedy can be prevented with precaution and care.
They exhale carbon dioxide into the space in which their faces rest and cannot take in oxygen. Experienced babies lift their heads and turn them, while babies who are new to stomach sleeping lift their heads up and put them right back down into the carbon dioxide. Without oxygen, they suffocate. This tragedy can be prevented with precaution and care. More boys die from SIDS than do girls. About 75% of infants dying unexpectedly and suddenly do so while sleeping on the same furniture as someone else. This includes couches, armchairs, and beds. While SIDS is not identical to suffocation, both can occur during a baby’s sleep time; this is why it is often called crib death. The National Institutes of Health describe SIDS as a silent, sudden medical disorder that can occur in an infant who seems otherwise healthy.
More boys die from SIDS than do girls. About 75% of infants dying unexpectedly and suddenly do so while sleeping on the same furniture as someone else. This includes couches, armchairs, and beds. While SIDS is not identical to suffocation, both can occur during a baby’s sleep time; this is why it is often called crib death. The National Institutes of Health describe SIDS as a silent, sudden medical disorder that can occur in an infant who seems otherwise healthy. When infants can move their heads from side to side, you can safely leave your baby slumbering. If a baby is lying truly face down, with the face pressed into the mattress, there is a problem.
When infants can move their heads from side to side, you can safely leave your baby slumbering. If a baby is lying truly face down, with the face pressed into the mattress, there is a problem. All babies woke up after a span of about five minutes to try and reach air that was fresher. The experienced infants turned their heads from the stale air. Inexperienced infants nuzzled their bedding or bobbed their heads briefly up, returning them straight down into the problem area.
All babies woke up after a span of about five minutes to try and reach air that was fresher. The experienced infants turned their heads from the stale air. Inexperienced infants nuzzled their bedding or bobbed their heads briefly up, returning them straight down into the problem area.

 Share sleeping areas until the baby is six months old. You will be more alert to trouble this way. Only bring the baby into your bed for comfort or to feed; when you are ready to sleep, back into the crib with the baby. Keep soft objects like stuffed toys or loose bedding out of the sleeping area for the baby. Pillows, bumper pads, and quilts are included in this category. They increase the risk of suffocation, strangulation, and entrapment, as stated by healthychildren.org.
Share sleeping areas until the baby is six months old. You will be more alert to trouble this way. Only bring the baby into your bed for comfort or to feed; when you are ready to sleep, back into the crib with the baby. Keep soft objects like stuffed toys or loose bedding out of the sleeping area for the baby. Pillows, bumper pads, and quilts are included in this category. They increase the risk of suffocation, strangulation, and entrapment, as stated by healthychildren.org.

 And usually pediatricians brush aside questions like yours, they say, what trifles bother parents! However, child psychologists consider such questions to be far from trifling and even undertake to interpret these postures. And although I am not convinced of the correctness of their interpretations, try to look at your son’s usual sleeping position through the eyes of these psychologists.
And usually pediatricians brush aside questions like yours, they say, what trifles bother parents! However, child psychologists consider such questions to be far from trifling and even undertake to interpret these postures. And although I am not convinced of the correctness of their interpretations, try to look at your son’s usual sleeping position through the eyes of these psychologists. 

 As gas bubbles escape, they have an annoying tendency to bring the rest of the stomach’s contents up with them. To minimize the chances of this happening, burp not only after, but also during meals.
As gas bubbles escape, they have an annoying tendency to bring the rest of the stomach’s contents up with them. To minimize the chances of this happening, burp not only after, but also during meals. In either case, spitting up may serve as one of several cues your baby may give you that it’s time to discuss alternative formulas with your pediatrician. If your baby does have a true intolerance, a 1- or 2-week trial of hypoallergenic (hydrolyzed) formula designed to be better tolerated might be recommended by your baby’s provider.
In either case, spitting up may serve as one of several cues your baby may give you that it’s time to discuss alternative formulas with your pediatrician. If your baby does have a true intolerance, a 1- or 2-week trial of hypoallergenic (hydrolyzed) formula designed to be better tolerated might be recommended by your baby’s provider.




 It isn’t painful to your baby, and most babies don’t even realize they have done it.
It isn’t painful to your baby, and most babies don’t even realize they have done it. Laying them flat on a full stomach can lead to spit-up
Laying them flat on a full stomach can lead to spit-up  If your baby’s fussy and has not been fed in more than 2 hours, it is probably time for a feeding.
If your baby’s fussy and has not been fed in more than 2 hours, it is probably time for a feeding.  There are things you can do to help when your baby is ill. Replace the fluids your baby is losing by giving them small, frequent feedings. In some cases, an oral rehydration solution such as Pedialyte® may be recommended. Check with your healthcare provider for advice.
There are things you can do to help when your baby is ill. Replace the fluids your baby is losing by giving them small, frequent feedings. In some cases, an oral rehydration solution such as Pedialyte® may be recommended. Check with your healthcare provider for advice.  Contact your healthcare professional if your baby vomits repeatedly.
Contact your healthcare professional if your baby vomits repeatedly.  As you get accustomed to your child’s immediate needs — meals, changing diapers, learning to safely strap them into their car seat — it is easy to forget the importance of early initiation of tummy time.
As you get accustomed to your child’s immediate needs — meals, changing diapers, learning to safely strap them into their car seat — it is easy to forget the importance of early initiation of tummy time. Positioning your child on their stomach allows them to gain the strength and coordination they need for future motor skills like rolling, sitting, crawling and walking.
Positioning your child on their stomach allows them to gain the strength and coordination they need for future motor skills like rolling, sitting, crawling and walking. As soon as possible, transition to tummy time positioned on a firm surface, such as a mat on the floor.
As soon as possible, transition to tummy time positioned on a firm surface, such as a mat on the floor. 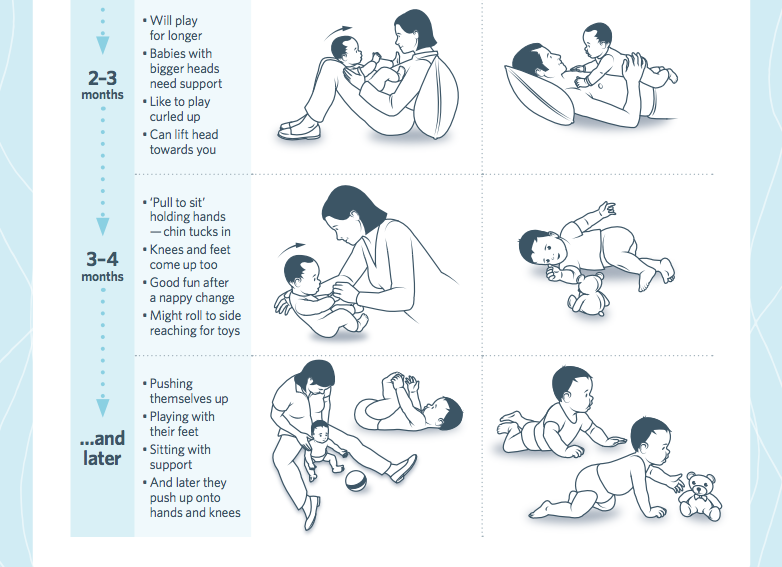 Allow them time to be soothed and reassured prior to resuming.
Allow them time to be soothed and reassured prior to resuming.  Allow them to play in that position for a few minutes before helping them roll to play while on their stomach.
Allow them to play in that position for a few minutes before helping them roll to play while on their stomach. Vomit may contain unchanged milk, mucus, blood or bile.
Vomit may contain unchanged milk, mucus, blood or bile.
 However, there are measures to help reduce the frequency of regurgitation.
However, there are measures to help reduce the frequency of regurgitation.
 After 10-15 minutes, the swallowed milk flows out unchanged, which is accompanied by a loud sound of air eructation.
After 10-15 minutes, the swallowed milk flows out unchanged, which is accompanied by a loud sound of air eructation.


 Due to this, the air that has entered the stomach will be able to go out. If nothing happened, then put the baby down and after a minute or two, lift him upright again.
Due to this, the air that has entered the stomach will be able to go out. If nothing happened, then put the baby down and after a minute or two, lift him upright again.

 Sometimes these fears are not unfounded, and regurgitation really has a pathological origin. What is its cause and when should you really consult a doctor about this?
Sometimes these fears are not unfounded, and regurgitation really has a pathological origin. What is its cause and when should you really consult a doctor about this? 
 The size of the opening in the nipple also matters – if it is too large, the newborn swallows a lot of air 3 .
The size of the opening in the nipple also matters – if it is too large, the newborn swallows a lot of air 3 . 
 With pathology, the problem manifests itself at any time of the day, regardless of when the baby was fed. Their number can reach 50 per day, and sometimes more 1 .
With pathology, the problem manifests itself at any time of the day, regardless of when the baby was fed. Their number can reach 50 per day, and sometimes more 1 .  A doctor’s consultation is necessary if the child is spitting up a lot (more than 15-30 ml at a time), with a frequency of more than 50 episodes per day 1.3 .
A doctor’s consultation is necessary if the child is spitting up a lot (more than 15-30 ml at a time), with a frequency of more than 50 episodes per day 1.3 .  To improve the situation, it is recommended to feed the baby more often, avoiding oversaturation, best of all – on demand 5 .
To improve the situation, it is recommended to feed the baby more often, avoiding oversaturation, best of all – on demand 5 . 
 No. 5 (48).
No. 5 (48). 
 In such a situation, you need to make sure that the gastrointestinal tract is functioning normally and consult a doctor.
In such a situation, you need to make sure that the gastrointestinal tract is functioning normally and consult a doctor.
 But if he still burps, you should not worry, this is a normal process. If in doubt, please contact our doctors. At a remote consultation, they will explain the causes of regurgitation, talk about pathologies. If necessary, they will tell you which specialists to go through.
But if he still burps, you should not worry, this is a normal process. If in doubt, please contact our doctors. At a remote consultation, they will explain the causes of regurgitation, talk about pathologies. If necessary, they will tell you which specialists to go through. 

 As a result, the surplus, of course, comes out.
As a result, the surplus, of course, comes out.
 This applies not only to the transition from breastfeeding to artificial feeding, but also from one type of mixture to another.
This applies not only to the transition from breastfeeding to artificial feeding, but also from one type of mixture to another.

 5 volume of food eaten
5 volume of food eaten


 If the child burped while lying on his back, you should lift him up and turn him face down.
If the child burped while lying on his back, you should lift him up and turn him face down.
 It is also necessary to make sure that the milk does not flow like a river, but slowly drips, that is, the hole in the nipple must have the appropriate diameter.
It is also necessary to make sure that the milk does not flow like a river, but slowly drips, that is, the hole in the nipple must have the appropriate diameter.





 com, a self-service online database of caregivers. Visit the HARVie Care.com page to learn about all of the services available through Care @ Work.
com, a self-service online database of caregivers. Visit the HARVie Care.com page to learn about all of the services available through Care @ Work. BNC nanny-placement services range from comprehensive placement packages to a-la-carte services such as in-depth consultation, thorough background checks, post-hire contract support, and other services. BNC offers Harvard affiliates 10% off any service. You can read more about BNC and their services by visiting their website, reading their description of services and reviewing their price list.
BNC nanny-placement services range from comprehensive placement packages to a-la-carte services such as in-depth consultation, thorough background checks, post-hire contract support, and other services. BNC offers Harvard affiliates 10% off any service. You can read more about BNC and their services by visiting their website, reading their description of services and reviewing their price list.
 com on a daily basis. Visit the HARVie Care.com page to learn more about services available through Care.com and for detailed instructions on how to register. Once you are pre-registered and have submitted the waiver, you will be directed to Harvard’s Care @ Work portal to register once using your Harvard email address. From there, you will be able to learn more and sign up for HomePay services.
com on a daily basis. Visit the HARVie Care.com page to learn more about services available through Care.com and for detailed instructions on how to register. Once you are pre-registered and have submitted the waiver, you will be directed to Harvard’s Care @ Work portal to register once using your Harvard email address. From there, you will be able to learn more and sign up for HomePay services.
 These centers are open year-round and care for children six weeks through school-age.
These centers are open year-round and care for children six weeks through school-age.  Referrals are provided so that parents can look into all of their options and find the child care arrangements that best meet the needs of their family. Parent Referral Specialists are available Monday through Friday, 8:00AM – 4:30PM by calling (855) 244-5301. Families can also conduct their own child care search online 24/7.
Referrals are provided so that parents can look into all of their options and find the child care arrangements that best meet the needs of their family. Parent Referral Specialists are available Monday through Friday, 8:00AM – 4:30PM by calling (855) 244-5301. Families can also conduct their own child care search online 24/7. com
com

 Shchorsa, 15
Shchorsa, 15  Polbina, 45A
Polbina, 45A 
 Petersburg, Rastrelli street, building 2, “Lit A”
Petersburg, Rastrelli street, building 2, “Lit A”  92″ Zvezdochka “
92″ Zvezdochka “
 Parents are encouraged to volunteer for events throughout the school year. Connections are made at Parent Night, Parent Get-togethers and Class Events, Field Trips, and Parent-Teacher conferences.
Parents are encouraged to volunteer for events throughout the school year. Connections are made at Parent Night, Parent Get-togethers and Class Events, Field Trips, and Parent-Teacher conferences. From safety units in the fall with visiting fire fighters to other special visitors children are engaged and stimulated.
From safety units in the fall with visiting fire fighters to other special visitors children are engaged and stimulated.




 Today, after so much time, during which everything would have changed 20 times for an ordinary child, having matured, but the same boy with even greater confidence reports that he dreams of treating people and becoming a surgeon.
Today, after so much time, during which everything would have changed 20 times for an ordinary child, having matured, but the same boy with even greater confidence reports that he dreams of treating people and becoming a surgeon.  He must have gotten bad grades.” Stas lived at home for about a year, went to first grade.
He must have gotten bad grades.” Stas lived at home for about a year, went to first grade.  Everything went well, I became an excellent student. I love to study, it’s interesting for me. As if something was missing, and once it appeared.
Everything went well, I became an excellent student. I love to study, it’s interesting for me. As if something was missing, and once it appeared.  “The very beginning of my life is like a fog, I just don’t remember anything. I think I saw my father once. I was standing in the entrance, and there was a man, he brought me something, he was wearing glasses. And this memory that I am small, and he is so big – it is very strong, so I think that it was not just a man.
“The very beginning of my life is like a fog, I just don’t remember anything. I think I saw my father once. I was standing in the entrance, and there was a man, he brought me something, he was wearing glasses. And this memory that I am small, and he is so big – it is very strong, so I think that it was not just a man.  For example, I have never been abroad. When I finish university and become a surgeon, I will go on my first trip. I’ll start with France, I want to visit Paris. I think it’s a good start for a famous doctor’s vacation!”
For example, I have never been abroad. When I finish university and become a surgeon, I will go on my first trip. I’ll start with France, I want to visit Paris. I think it’s a good start for a famous doctor’s vacation!”  It is very important for us that Stas remains in the program and has the opportunity to study remotely and further. And it depends on everyone who reads the article about this amazing boy from the Arkhangelsk region.
It is very important for us that Stas remains in the program and has the opportunity to study remotely and further. And it depends on everyone who reads the article about this amazing boy from the Arkhangelsk region. 



 I always argued with Kortatai, saying that he was of the old school, that now everything is not the same as before, and only now, from the height of the years I have lived (even though I am not old yet, but I am not twenty anymore), I understand that 99 percent of what he said was correct. I am grateful to him for every word and I use the experience passed on to me in my work. I am grateful to my grandfather and father for instilling in me not just a love for music and creativity, but real respect and devotion to this work. Therefore, no matter what situations in life may be, I have never turned off this path and I am going to follow it to the end.
I always argued with Kortatai, saying that he was of the old school, that now everything is not the same as before, and only now, from the height of the years I have lived (even though I am not old yet, but I am not twenty anymore), I understand that 99 percent of what he said was correct. I am grateful to him for every word and I use the experience passed on to me in my work. I am grateful to my grandfather and father for instilling in me not just a love for music and creativity, but real respect and devotion to this work. Therefore, no matter what situations in life may be, I have never turned off this path and I am going to follow it to the end.  Now everything is changing, and songs that have been lived are becoming popular: if this is lyrics, then this is a song of suffering – text, music, performance. I think if Gumer Abdulmanov were alive and young now, he would sing his songs, of course, in a modern interpretation, and would be a popular and respected artist. After all, what is happening around now, in general, repeats the time when he was just embarking on his musical path, says Murat Abdulmanov.
Now everything is changing, and songs that have been lived are becoming popular: if this is lyrics, then this is a song of suffering – text, music, performance. I think if Gumer Abdulmanov were alive and young now, he would sing his songs, of course, in a modern interpretation, and would be a popular and respected artist. After all, what is happening around now, in general, repeats the time when he was just embarking on his musical path, says Murat Abdulmanov.  I hope that my songs will remain after me and my children and grandchildren will be just as proud of me as I am proud of my kortatai,” says Murat Abdulmanov.
I hope that my songs will remain after me and my children and grandchildren will be just as proud of me as I am proud of my kortatai,” says Murat Abdulmanov. 

 Since I’ve been the biggest… Read More
Since I’ve been the biggest… Read More

 I a… Read More
I a… Read More

 .. Read More
.. Read More
 It would be my pleasure to help you with the care of your children.
It would be my pleasure to help you with the care of your children. 
 If anyone I’ve interacted with before has read…
If anyone I’ve interacted with before has read… pro
pro
 5 years old, with accommodation (2 nannies, a nanny is needed for the younger ones)
5 years old, with accommodation (2 nannies, a nanny is needed for the younger ones) WHO vaccination required to enter the US
WHO vaccination required to enter the US

 99
99 99
99 99
99 99
99 99
99 They are gorgeous and the softest baby blanket for swaddling and tons of other uses too. They’re definitely a unique style and color.
They are gorgeous and the softest baby blanket for swaddling and tons of other uses too. They’re definitely a unique style and color. They are highly popular with parents because they are big, soft, and have delightful animal patterns. They’d work great as baby receiving blankets.
They are highly popular with parents because they are big, soft, and have delightful animal patterns. They’d work great as baby receiving blankets. Reviewers love the high quality that makes these feel like luxury baby blankets and baby receiving blankets.
Reviewers love the high quality that makes these feel like luxury baby blankets and baby receiving blankets.
 But parens also love the ease with which you can swaddle up your babe in seconds. It’s made of organic material and is ranked the #1 swaddle by the New York Times.
But parens also love the ease with which you can swaddle up your babe in seconds. It’s made of organic material and is ranked the #1 swaddle by the New York Times. The best part of baby receiving blankets is they can be used for so many different things like a burp cloth, a swaddle, a blanket for warmth, a playmat, and more! They’ve been around for basically… ever… and with good reason. They’re so functional and inexpensive.
The best part of baby receiving blankets is they can be used for so many different things like a burp cloth, a swaddle, a blanket for warmth, a playmat, and more! They’ve been around for basically… ever… and with good reason. They’re so functional and inexpensive. 

 If you’ve narrowed your choices down to Similac Advance vs Pro Advance, but just can’t …
If you’ve narrowed your choices down to Similac Advance vs Pro Advance, but just can’t … You must have noticed, every little detail about your baby, his nose, his eyes, his tiny hands and fingers, and even the soft white blanket he was wrapped in. Now you must have folded up that receiving blanket neatly in a drawer and perhaps it will never see the light of the day, but do you know that your little munchkin’s first blanket can be used in so many ways? The very first blanket that many families receive their baby snuggled up in is called a receiving blanket. Read on to learn more about receiving blanket and how can you put one to good use once it has served its purpose!
You must have noticed, every little detail about your baby, his nose, his eyes, his tiny hands and fingers, and even the soft white blanket he was wrapped in. Now you must have folded up that receiving blanket neatly in a drawer and perhaps it will never see the light of the day, but do you know that your little munchkin’s first blanket can be used in so many ways? The very first blanket that many families receive their baby snuggled up in is called a receiving blanket. Read on to learn more about receiving blanket and how can you put one to good use once it has served its purpose! While hospitals usually provide one, most new mothers tend to buy standard off-the-shelf receiving blankets for their babies, as one can never have enough of receiving blankets for their babies. If you want to make it extra special, you can always make one yourself.
While hospitals usually provide one, most new mothers tend to buy standard off-the-shelf receiving blankets for their babies, as one can never have enough of receiving blankets for their babies. If you want to make it extra special, you can always make one yourself.
 The familiar scent and warmth will provide comfort to your baby and he will fall asleep in it in a matter of minutes.
The familiar scent and warmth will provide comfort to your baby and he will fall asleep in it in a matter of minutes. Being soft and thin, they are easy to cut through, so no hassle there!
Being soft and thin, they are easy to cut through, so no hassle there! While receiving blankets can be used to swaddle a baby, they can’t be used for long enough as babies quickly outgrow them as they grow up. The major difference between the two is their size. A receiving blanket is usually 30 inches by 30 inches while a swaddling blanket is usually 47 inches by 47 inches. Swaddling blankets are made out of a more elastic material to make it easier to wrap your baby. They also feature attachments such as Velcro or button clips to keep it in place while your baby is wrapped.
While receiving blankets can be used to swaddle a baby, they can’t be used for long enough as babies quickly outgrow them as they grow up. The major difference between the two is their size. A receiving blanket is usually 30 inches by 30 inches while a swaddling blanket is usually 47 inches by 47 inches. Swaddling blankets are made out of a more elastic material to make it easier to wrap your baby. They also feature attachments such as Velcro or button clips to keep it in place while your baby is wrapped.
 ..
.. Usually the child does this when getting ready for bed, and may become so attached to this item that he will flatly refuse to part with the blanket, even when it needs to be washed. Usually such a habit does not reveal any serious consequences for the child, although it can greatly annoy parents. The habit of sucking on a blanket remains until the age of 8-10, and then disappears without a trace. Why does this habit occur?
Usually the child does this when getting ready for bed, and may become so attached to this item that he will flatly refuse to part with the blanket, even when it needs to be washed. Usually such a habit does not reveal any serious consequences for the child, although it can greatly annoy parents. The habit of sucking on a blanket remains until the age of 8-10, and then disappears without a trace. Why does this habit occur?  For children, suckling is a much more familiar way of warding off fears than talking. By his actions, the baby subconsciously signals that he is experiencing anxiety, inconvenience, that he is scared. Such a habitual action, like sucking on a blanket, stabilizes the state of mind of the baby. This is purely a childish habit, passing with age.
For children, suckling is a much more familiar way of warding off fears than talking. By his actions, the baby subconsciously signals that he is experiencing anxiety, inconvenience, that he is scared. Such a habitual action, like sucking on a blanket, stabilizes the state of mind of the baby. This is purely a childish habit, passing with age. 
 We will try to prevent and, if necessary, eliminate this habit.
We will try to prevent and, if necessary, eliminate this habit. 
 Or, having learned to dress on his own, he begins to act up and demand that his parents dress him again. Similarly, once weaned or bottled, a baby may want to suckle again. If this continues for a long time, it signals that the child for some reason does not want to grow up (it is necessary to identify the reasons)
Or, having learned to dress on his own, he begins to act up and demand that his parents dress him again. Similarly, once weaned or bottled, a baby may want to suckle again. If this continues for a long time, it signals that the child for some reason does not want to grow up (it is necessary to identify the reasons)  Be patient, be more affectionate and softer, show interest in adult moments in the child’s behavior. Approval and love give children courage and perseverance. In their absence, children become infantile and lost.
Be patient, be more affectionate and softer, show interest in adult moments in the child’s behavior. Approval and love give children courage and perseverance. In their absence, children become infantile and lost. 
 Think about whether you have been overly harsh and strict or nervous lately. Maybe you were punishing a child. It is also likely that you were too demanding of him. If the child accumulates irritation or excitement, but the opportunity to take the soul is not provided, he may bite his nails. Try to relieve nervous tension in the baby.
Think about whether you have been overly harsh and strict or nervous lately. Maybe you were punishing a child. It is also likely that you were too demanding of him. If the child accumulates irritation or excitement, but the opportunity to take the soul is not provided, he may bite his nails. Try to relieve nervous tension in the baby.  Don’t worry about these outbursts. After all, adults also tend to take the soul. If you constantly suppress the free expression of feelings in a child, you will only achieve that aggression will accumulate in him and overwhelm him. Encourage acceptable forms of aggression in sports or team games.
Don’t worry about these outbursts. After all, adults also tend to take the soul. If you constantly suppress the free expression of feelings in a child, you will only achieve that aggression will accumulate in him and overwhelm him. Encourage acceptable forms of aggression in sports or team games.  This, in turn, can have a significant negative impact on the entire family. This guide explains what may be causing your child’s sleep problems and what you can do to ensure a restful night for both your child and yourself.
This, in turn, can have a significant negative impact on the entire family. This guide explains what may be causing your child’s sleep problems and what you can do to ensure a restful night for both your child and yourself.  If after this age your child regularly cannot fall asleep or sleeps normally for a while and then wakes up abruptly, then this is a sleep disorder. It is important to recognize that short-term sleep disturbances in children often occur after illness, during holidays, holidays such as Christmas, or during periods of acute stress, such as school exams or the illness of a loved one. After such events, the normal sleep pattern should be restored in the child within a few days.
If after this age your child regularly cannot fall asleep or sleeps normally for a while and then wakes up abruptly, then this is a sleep disorder. It is important to recognize that short-term sleep disturbances in children often occur after illness, during holidays, holidays such as Christmas, or during periods of acute stress, such as school exams or the illness of a loved one. After such events, the normal sleep pattern should be restored in the child within a few days.  However, these are not hard numbers, and it is possible that some 16-year-old child needs 10 hours of sleep per night, and some five-year-old child needs seven hours.
However, these are not hard numbers, and it is possible that some 16-year-old child needs 10 hours of sleep per night, and some five-year-old child needs seven hours. 

 However, Donna Williams, who has detailed her experience of living with an autism spectrum disorder, speaks in her autobiography about her fear of falling asleep:
However, Donna Williams, who has detailed her experience of living with an autism spectrum disorder, speaks in her autobiography about her fear of falling asleep:  However, they suggest that Donna had more trouble getting to bed than waking up. We do not know which problems children with autism most often suffer from, although we do know children who have problems with both.
However, they suggest that Donna had more trouble getting to bed than waking up. We do not know which problems children with autism most often suffer from, although we do know children who have problems with both. 



 Children with autism are often unable to articulate their need to de-stress and relax. In addition, when they go to bed, they may experience great anxiety and confusion.
Children with autism are often unable to articulate their need to de-stress and relax. In addition, when they go to bed, they may experience great anxiety and confusion.  Obviously, the introduction of a quiet period is easier said than done, but you can start small: for example, turn off the TV and computer for an hour. It should take some time before it becomes a routine, but if you succeed, then the effect will not be long in coming. It is also worth introducing this quiet time into the daily routine so that the child knows what to expect and gets used to such a routine.
Obviously, the introduction of a quiet period is easier said than done, but you can start small: for example, turn off the TV and computer for an hour. It should take some time before it becomes a routine, but if you succeed, then the effect will not be long in coming. It is also worth introducing this quiet time into the daily routine so that the child knows what to expect and gets used to such a routine.  30: bedtime/sleep time
30: bedtime/sleep time  If that’s your child’s experience, it’s no surprise if he looks excited when it’s time for bed. However, you can work on the child’s fears to help him.
If that’s your child’s experience, it’s no surprise if he looks excited when it’s time for bed. However, you can work on the child’s fears to help him. 
 Even the colors of the room or the pictures on the wall can disturb sleep.
Even the colors of the room or the pictures on the wall can disturb sleep.  As a general rule, it is best to minimize the use of drugs by the child, but in some cases a mild sedative should be available. For example, if you are going on a trip and are afraid of problems with jet lag, or you are afraid that your child’s overall health is suffering because of poor sleep. Most physicians are willing to prescribe drugs in such circumstances.
As a general rule, it is best to minimize the use of drugs by the child, but in some cases a mild sedative should be available. For example, if you are going on a trip and are afraid of problems with jet lag, or you are afraid that your child’s overall health is suffering because of poor sleep. Most physicians are willing to prescribe drugs in such circumstances. 



 Excessive sleep in this age group can indicate serious psychological problems, and you need to consider this possibility, and not just write off excessive sleep as laziness. Again, sleep monitoring can help establish patterns that indicate potential problems.
Excessive sleep in this age group can indicate serious psychological problems, and you need to consider this possibility, and not just write off excessive sleep as laziness. Again, sleep monitoring can help establish patterns that indicate potential problems. 
 It is worth carefully approaching the choice of these products, as there are a lot of nuances that parents should consider.
It is worth carefully approaching the choice of these products, as there are a lot of nuances that parents should consider.  Good options would be natural fabrics: silk or high-quality cotton. These materials are pleasant to the touch, environmentally friendly, hypoallergenic, have good breathability and wear resistance.
Good options would be natural fabrics: silk or high-quality cotton. These materials are pleasant to the touch, environmentally friendly, hypoallergenic, have good breathability and wear resistance. 




 She’s an active parent who enjoys indoor and outdoor adventures with her family. Her mission is to share practical and realistic parenting advice to help the parenting community becoming stronger.
She’s an active parent who enjoys indoor and outdoor adventures with her family. Her mission is to share practical and realistic parenting advice to help the parenting community becoming stronger. As a new mom, we love holding my babes close, feeling their tiny hearts beating in tandem with ours. There’s no doubt this creates a sacred bond with your baby—but is it safe?
As a new mom, we love holding my babes close, feeling their tiny hearts beating in tandem with ours. There’s no doubt this creates a sacred bond with your baby—but is it safe? Apart from increasing the risk of Sudden Infant Death Syndrome (SIDS), it also increases the risk of accidents or suffocation.
Apart from increasing the risk of Sudden Infant Death Syndrome (SIDS), it also increases the risk of accidents or suffocation. He was living in your womb for so many months that he is used to the snug and comforting feeling. Wrapping your baby or swaddling him will help replicate that amazing feeling, which will help your baby sleep well.
He was living in your womb for so many months that he is used to the snug and comforting feeling. Wrapping your baby or swaddling him will help replicate that amazing feeling, which will help your baby sleep well. However, there are chances that your baby might face problems later since he will be accustomed to sleeping using the Rock-N-Play technique. But note that this method is not considered to be the safest of all the other sleep surfaces since it is not flat and firm. You should check with your doctor if you feel like there is not enough space for the baby to sleep.
However, there are chances that your baby might face problems later since he will be accustomed to sleeping using the Rock-N-Play technique. But note that this method is not considered to be the safest of all the other sleep surfaces since it is not flat and firm. You should check with your doctor if you feel like there is not enough space for the baby to sleep. Many babies need to learn how to sleep well independently in other spaces.
Many babies need to learn how to sleep well independently in other spaces. See How to Keep Your Sleeping Baby Safe: AAP Policy Explained External icon to learn more about these and other actions.
See How to Keep Your Sleeping Baby Safe: AAP Policy Explained External icon to learn more about these and other actions.

 Why? To help their child sleep, to make nursing easier, to bond with Baby, and because Baby won’t sleep anywhere else, they say.
Why? To help their child sleep, to make nursing easier, to bond with Baby, and because Baby won’t sleep anywhere else, they say. They don’t learn to soothe themselves, and that’s what keeps them up.
They don’t learn to soothe themselves, and that’s what keeps them up.
 Today we know that this yearning for closeness is a physiological need shared by you and your baby. Studies have shown that newborns who are placed skin-to-skin on your chest right after birth will adjust more easily to life outside the womb, stay warmer, cry less and breastfeed sooner than if your baby is separated from you.
Today we know that this yearning for closeness is a physiological need shared by you and your baby. Studies have shown that newborns who are placed skin-to-skin on your chest right after birth will adjust more easily to life outside the womb, stay warmer, cry less and breastfeed sooner than if your baby is separated from you. )
)
 When my son is hungry we both half wake up together, he latches on to nurse and we both fall back to sleep. No need to get up. No need to turn the lights on. We both stay warm in bed together, nurse and nod off.
When my son is hungry we both half wake up together, he latches on to nurse and we both fall back to sleep. No need to get up. No need to turn the lights on. We both stay warm in bed together, nurse and nod off.
 He doesn’t need to waste energy crying to get our attention so he can put it directly into growing. And body contact is well known to be even more important than milk in determining growth rates.
He doesn’t need to waste energy crying to get our attention so he can put it directly into growing. And body contact is well known to be even more important than milk in determining growth rates. To use a crib. A pacifier. An exersaucer. A walker. To let my baby cry. It sure would make for far easier conversations at mummy groups! But that’s not for me. My only important parenting critic is my son.
To use a crib. A pacifier. An exersaucer. A walker. To let my baby cry. It sure would make for far easier conversations at mummy groups! But that’s not for me. My only important parenting critic is my son.
 They eat, sleep, feel calm precisely from the presence of their mother in the immediate vicinity. Where have you seen a cat that puts kittens in a “separate basket”, for example? It’s not just that. The child needs to sleep next to his mother, so as not to worry, to grow and develop calmly.
They eat, sleep, feel calm precisely from the presence of their mother in the immediate vicinity. Where have you seen a cat that puts kittens in a “separate basket”, for example? It’s not just that. The child needs to sleep next to his mother, so as not to worry, to grow and develop calmly.  Therefore, in your arms the baby is comfortable, warm, he is safe. Many parents have noticed that their child sleeps much better, wakes up less often and cries when they put him under their wing for the night. Psychologists have proven that not only the baby needs co-sleeping. Moms also sleep soundly and sweetly when the baby hugs them with her arms and sniffs on her chest.
Therefore, in your arms the baby is comfortable, warm, he is safe. Many parents have noticed that their child sleeps much better, wakes up less often and cries when they put him under their wing for the night. Psychologists have proven that not only the baby needs co-sleeping. Moms also sleep soundly and sweetly when the baby hugs them with her arms and sniffs on her chest.  And you have to get up and rock again. If you sleep together, you won’t have to jump up and check how your bunny is doing, is it sleeping, breathing, why is it “quacking”?
And you have to get up and rock again. If you sleep together, you won’t have to jump up and check how your bunny is doing, is it sleeping, breathing, why is it “quacking”?  And if a child is comfortable in a dream and has nothing to worry about, he has time and an opportunity to comprehend everything new, to “digest”, without being distracted by anything. Therefore, psychologists believe that children who sleep with their parents develop faster.
And if a child is comfortable in a dream and has nothing to worry about, he has time and an opportunity to comprehend everything new, to “digest”, without being distracted by anything. Therefore, psychologists believe that children who sleep with their parents develop faster. 
 But the children, whom their parents put next to them on demand, calmly “leave” to their bed over time, because their “need for a mother” was successfully satisfied.
But the children, whom their parents put next to them on demand, calmly “leave” to their bed over time, because their “need for a mother” was successfully satisfied. 



 It is written about its danger, about the fact that the mother prevents the child from sleeping, and so on and so forth.
It is written about its danger, about the fact that the mother prevents the child from sleeping, and so on and so forth.  If vomiting occurs during the self-sleep method, then go to the baby immediately, change his clothes, clean the room, change the bed linen and follow the plan further, as indicated. If you remain calm and confident, the child will quickly understand that vomiting does not affect your decision, and will learn to fall asleep on his own, ”then I felt bad – I could not imagine how I could bring my beloved, desired, tender manual girl to SUCH? Is it normal? It’s generally acceptable – so to scoff at someone who can not fight back, so depends on you? Or am I not understanding something?
If vomiting occurs during the self-sleep method, then go to the baby immediately, change his clothes, clean the room, change the bed linen and follow the plan further, as indicated. If you remain calm and confident, the child will quickly understand that vomiting does not affect your decision, and will learn to fall asleep on his own, ”then I felt bad – I could not imagine how I could bring my beloved, desired, tender manual girl to SUCH? Is it normal? It’s generally acceptable – so to scoff at someone who can not fight back, so depends on you? Or am I not understanding something? 
 And that separate sleep kills GW. And children really need breastfeeding at least up to a year, and preferably longer.
And that separate sleep kills GW. And children really need breastfeeding at least up to a year, and preferably longer. 

 But that’s not the point. The fact is that the brain grows, the phases of sleep lengthen. And her son lengthened, and my daughter. Regardless of the chest.
But that’s not the point. The fact is that the brain grows, the phases of sleep lengthen. And her son lengthened, and my daughter. Regardless of the chest. 

 Well, like terrible nightmares, etc. The disease affects its development, and this is far from the only problem of such children.
Well, like terrible nightmares, etc. The disease affects its development, and this is far from the only problem of such children.  However, this is done in case of serious violations, and to investigate the norms of sleep in this way – why and who needs it when there are separately sleeping children?
However, this is done in case of serious violations, and to investigate the norms of sleep in this way – why and who needs it when there are separately sleeping children?  Which makes her extremely attractive to me.
Which makes her extremely attractive to me.  ”
”  e. solitary. All ways to manage children’s sleep come down to reducing contact with parents as early as possible and reducing feedings at night. There is widespread advice to “don’t let babies get used to falling asleep while eating, including while breastfeeding,” “don’t teach a baby to fall asleep when a parent soothes and caresses the baby.” These tips are fundamentally contrary to the very context of the evolution of infant sleep in relation to parental emotions. Today, more and more children are breastfeeding in the United States. If breastfeeding is so widespread, and proving to be biologically correct, according to cross-cultural studies, the current recommendations for sleep management will not only not work, but will even interfere with many mothers.”
e. solitary. All ways to manage children’s sleep come down to reducing contact with parents as early as possible and reducing feedings at night. There is widespread advice to “don’t let babies get used to falling asleep while eating, including while breastfeeding,” “don’t teach a baby to fall asleep when a parent soothes and caresses the baby.” These tips are fundamentally contrary to the very context of the evolution of infant sleep in relation to parental emotions. Today, more and more children are breastfeeding in the United States. If breastfeeding is so widespread, and proving to be biologically correct, according to cross-cultural studies, the current recommendations for sleep management will not only not work, but will even interfere with many mothers.”  Using this kind of criteria to evaluate “developmental progress” can do more harm than good, especially if the actual sleep conditions differ from the sleep conditions for which such an assessment is intended.
Using this kind of criteria to evaluate “developmental progress” can do more harm than good, especially if the actual sleep conditions differ from the sleep conditions for which such an assessment is intended.  This is not evidence of parental incompetence, but rather a lack of flexibility in interpreting and applying the advice given by health professionals.”
This is not evidence of parental incompetence, but rather a lack of flexibility in interpreting and applying the advice given by health professionals.”  If a child does not sleep enough, his nervous system suffers, if he cannot develop normally, if he is really sick! Here, visits to doctors and even medicines are justified – there are situations that are really serious. But in 99% (a figure from me, approximate) of cases, we are not talking about sleep disturbance. It’s about sleep patterns. And if the baby wakes up to suck on the breast – this is the norm! It is important for mom to get enough sleep, co-sleeping helps, as well as daytime sleep.
If a child does not sleep enough, his nervous system suffers, if he cannot develop normally, if he is really sick! Here, visits to doctors and even medicines are justified – there are situations that are really serious. But in 99% (a figure from me, approximate) of cases, we are not talking about sleep disturbance. It’s about sleep patterns. And if the baby wakes up to suck on the breast – this is the norm! It is important for mom to get enough sleep, co-sleeping helps, as well as daytime sleep.  In every possible way try to improve his sleep without a mother, resort to tricks and tricks. All this has its place. There is no place to be accustomed to a separate sleep, accustoming through tears, weaning in order for the child to finally “sleep normally”.
In every possible way try to improve his sleep without a mother, resort to tricks and tricks. All this has its place. There is no place to be accustomed to a separate sleep, accustoming through tears, weaning in order for the child to finally “sleep normally”.  I am sorry that I spent so many nerves and strength worrying about why my child is not sleeping as soundly as I would like, why I cannot put him to bed and go about my business. I’m sorry that one of my grandmothers raised children on a schedule, and the second didn’t raise children at all, but worked, that my grandfather still exhorts me to put my daughter in a crib and accustom her to her, that my progressive mother in the first difficult months of my girl is so I was worried that this was “breast slavery”, that it was impossible to sleep with a breast, that it was too hard for me. I’m sorry that a bunch of kids around the world are doing all sorts of horrors like being left screaming and being taught to sleep.
I am sorry that I spent so many nerves and strength worrying about why my child is not sleeping as soundly as I would like, why I cannot put him to bed and go about my business. I’m sorry that one of my grandmothers raised children on a schedule, and the second didn’t raise children at all, but worked, that my grandfather still exhorts me to put my daughter in a crib and accustom her to her, that my progressive mother in the first difficult months of my girl is so I was worried that this was “breast slavery”, that it was impossible to sleep with a breast, that it was too hard for me. I’m sorry that a bunch of kids around the world are doing all sorts of horrors like being left screaming and being taught to sleep. 
 This happened! Even though it never seemed to happen. Well, in a wheelchair on the street – it’s easy. No nipples, thumb sucking, transient objects, etc.
This happened! Even though it never seemed to happen. Well, in a wheelchair on the street – it’s easy. No nipples, thumb sucking, transient objects, etc.  Someday we will finish with GV and get some sleep (and I will finally smoke a hookah 🙂 ). But for now from 80-90 years (I am an optimist) of my life, I am ready not to get enough sleep for a couple of years in order to give my daughter the most important thing that she needs – breastfeeding and my mother’s carcass nearby. 🙂
Someday we will finish with GV and get some sleep (and I will finally smoke a hookah 🙂 ). But for now from 80-90 years (I am an optimist) of my life, I am ready not to get enough sleep for a couple of years in order to give my daughter the most important thing that she needs – breastfeeding and my mother’s carcass nearby. 🙂  Each child needs their own approach, and their own standards. Some children like to sleep more, while others, on the contrary, refuse the next daytime sleep early. So how do you know your baby is getting enough sleep if the sleep rations don’t match the amount of sleep your baby sleeps?
Each child needs their own approach, and their own standards. Some children like to sleep more, while others, on the contrary, refuse the next daytime sleep early. So how do you know your baby is getting enough sleep if the sleep rations don’t match the amount of sleep your baby sleeps?  How does the baby feel while awake? A healthy baby (over 3 months old), who sleeps well day and night, behaves calmly for a significant part of his wakefulness, does not cry all the time he is awake, is able to observe what is happening and concentrate on an interesting subject or activity for a short time. Older babies, who can crawl and/or sit on their own, can keep themselves occupied for a while if their mother is nearby or even sometimes without her presence. If the baby, on the contrary, is very capricious, calm only in his mother’s arms, if she constantly distracts him with something, cannot fix her attention on objects, quickly starts to cry, fidget and get nervous, then this may mean that he does not get enough sleep. Although this criterion is very relative, and it is necessary to study the situation in more detail.
How does the baby feel while awake? A healthy baby (over 3 months old), who sleeps well day and night, behaves calmly for a significant part of his wakefulness, does not cry all the time he is awake, is able to observe what is happening and concentrate on an interesting subject or activity for a short time. Older babies, who can crawl and/or sit on their own, can keep themselves occupied for a while if their mother is nearby or even sometimes without her presence. If the baby, on the contrary, is very capricious, calm only in his mother’s arms, if she constantly distracts him with something, cannot fix her attention on objects, quickly starts to cry, fidget and get nervous, then this may mean that he does not get enough sleep. Although this criterion is very relative, and it is necessary to study the situation in more detail.  This is a very controversial criterion, since there are many reasons for poor appetite, but poor sleep cannot be ruled out as one of the main ones. If the baby often wakes up at night, sleeps short dreams throughout the day, then he does not have time to “enter” the deep phase of sleep, and his body does not get enough rest, the level of growth hormone in the blood decreases, simply put – it grows more slowly. Because of this, appetite can theoretically decrease, and weight can grow more slowly. Therefore, if the baby does not eat well, you need to think not only about how to increase physical activity, or stimulate his activity more, but also take into account whether he sleeps enough.
This is a very controversial criterion, since there are many reasons for poor appetite, but poor sleep cannot be ruled out as one of the main ones. If the baby often wakes up at night, sleeps short dreams throughout the day, then he does not have time to “enter” the deep phase of sleep, and his body does not get enough rest, the level of growth hormone in the blood decreases, simply put – it grows more slowly. Because of this, appetite can theoretically decrease, and weight can grow more slowly. Therefore, if the baby does not eat well, you need to think not only about how to increase physical activity, or stimulate his activity more, but also take into account whether he sleeps enough. 