






Salivating baby: Understanding Your Drooling Baby – Playtime Pediatric Dentistry
Facts About Your Drooling Baby. Is it natural?
Facts About Your Drooling Baby. Is it natural?
Babies drool. Sometimes you may feel that your baby drools more than other babies. That may be true, or it may just be because at times babies drool A LOT. Most of the time babies drooling excessively isn’t a concern but occasionally, it’s indicative of a problem that needs to be addressed.
LOOKING FOR INFANT CARE? START YOUR FREE SEARCH NOW TO FIND THE BEST DAYCARE NEAR YOU
How do you know when your baby drooling excessively is an issue you need to follow up on or when it’s just typical development? Read on to find out some great facts about why babies drool and how much is too much.
Why Does My Baby Drool Anyway?
Drooling occurs when excess saliva is produced and not swallowed. Humans have six salivary glands which are located in the bottom of the mouth, the cheeks, and near the front teeth. It’s typical to produce two to four pints of saliva daily (that’s about 1-2 liters for our metric friends). There are two primary reasons babies produce excess saliva and two primary reasons they drool.
DOES YOUR BABY CRY WHEN YOU PUT HER DOWN? FIND OUT THE REASON WHY HERE.
The reasons babies produce excess saliva
1. Development of the digestive system
When your baby is born, she or he does not have a fully developed digestive system. As their digestive system develops, babies drool. You might feel like drool is icky and drippy, but it does serve a purpose, which is to help your baby break down food and nutrients on the way to the stomach.
2. Teething
When your baby is teething, you might find she or he is putting more things in their mouth and gnawing at them. Often babies do this as a way to soothe sore gums when a new tooth is breaking through. This increased mouth activity signals the brain to increase saliva production and you’ll notice your baby drooling more.
The reasons why babies drool
1. Underdeveloped muscles
Underdeveloped muscles
As nearly everyone knows, muscles and coordination develop when you use them. As adults, swallowing is easy – we’ve had years of practice. But for babies, the muscles used to swallow haven’t yet had time to gain strength. In fact, the muscles around your babies mouth and their swallowing muscles aren’t fully developed until they are between 18 and 24 months old! Babies aren’t able to swallow their saliva fast enough, so drool occurs.
2. Teeth (or lack thereof)
Your teeth act like a dam for your saliva, helping it pool in the bottom of your mouth before you swallow it. While babies are still getting their chompers, there’s little to prevent the saliva from spilling out and becoming drool.
What Can I Do to Keep My Baby’s Clothes and Face Dry?
As you can probably guess, bibs are the best defense against wet clothing from your baby’s drool. Choosing bibs for your baby seems simple – pick one out with a cute pattern and you’re done with it. But some bibs are great for drool and some are great for feeding.
But some bibs are great for drool and some are great for feeding.
For babies who drool a lot, an absorbent terry cloth bib will soak up the most saliva. It’s important that the bib has multiple layers or you’ll find your child’s shirt still will get quite wet.
To keep your baby’s face dry and prevent drool rash, wipe with the bib or another soft cloth. Make sure you dry the folds of your baby’s neck as well when drool is excessive. If your child has eczema or sensitive skin, a terry cloth bib may be too rough on them. In that case, opt for a 100% cotton bib, which will be gentler. Again, look for multiple layers.
It’s critical that you never put your baby to sleep while wearing a bib, and you should remove it promptly if your baby falls asleep. Bibs pose a strangulation risk and don’t fall within safe baby sleep practices.
How Can I Prevent and Treat Drool Rash?
Sometimes, especially in winter months, your baby may develop a rash on his or her cheeks, chin, or even neck from the combination of drool, dry weather, and wiping. This can be uncomfortable for your child, but don’t worry – there are a few things you can do a few things to keep the rash away and treat drool rash if it appears.
This can be uncomfortable for your child, but don’t worry – there are a few things you can do a few things to keep the rash away and treat drool rash if it appears.
1. Keep skin dry
Try to keep the skin dry and use soft cloths to wipe away drool. You may need to experiment with fabrics so they don’t irritate her or his skin.
2. Help prevent drool rash with a barrier cream
Check with your pediatrician first, but barrier products like Aquafor and Vaseline can prevent rash from occurring and soothe your baby’s skin if drool rash is present. if you don’t want to use a petroleum-based emollient, alternatives do exist, however you can expect a higher price tag and finding a fragrance-free version may be difficult.
3. Use fragrance-free detergent
Often a baby’s skin is sensitive to fragrances in laundry detergent and drool rash can be irritated by harsh chemicals. Wash bedding, clothing – including yours – and bibs in a baby-friendly fragrance-free detergent.
IS BREAST REALLY BEST? ENDING THE DEBATE
4. Monitor pacifier use
Every baby is different. Some babies drool more when they use pacifiers and some actually drool less. If your baby uses a pacifier you can watch to see what happens and limit pacifier use while they have a drool rash.
5. Check bottles for irritants
If formula leaks out of a bottle while your baby is feeding, it may irritate her or his drool rash, so makes sure that’s not occurring. The exterior of the bottle may also rub against your baby’s face and irritate the space or introduce germs to the drool rash if the bottle is not sterile.
6. Put breastmilk on it
Liquid gold! Breast milk has so many nutrients and restorative properties. There are moms everywhere who swear by its ability to soothe a drool rash.
7. Treat with creams
There are many different moisturizing creams on the market that may help soothe your baby’s drool rash and speed up healing. Check with your pediatrician to determine what’s safe for your baby.
Check with your pediatrician to determine what’s safe for your baby.
As they say, an ounce of prevention is worth a pound of cure, but sometimes, drool rash happens regardless. If it does, you can expect it to clear up relatively quickly.
THE FASCINATING HISTORY OF SLEEP TRAINING
Should I Ever Be Concerned About Drooling?
There are a few times that your baby’s drool may be a sign of something else going on that has to be monitored or addressed.
1. Dehydration
If the weather is hot and your baby is drinking less than she or he typically does, drool can become thick. Thick drool is a sign of dehydration so you should immediately increase your child’s liquid intake and monitor their diapers. If your baby isn’t producing enough wet diapers or you’re unable to hydrate him or her, contact your pediatrician to determine the best course of action.
2. Illness
At times, drooling can also be a sign of illness. If your baby’s drool increases and he or she is fussy, you might assume teething is the culprit, but look for signs of a sore throat as well. Your body produces extra saliva when your throat is irritated to soothe it. Since babies have limited ways of communicating, keep an eye on her or him grabbing at their ears or neck.
If your baby’s drool increases and he or she is fussy, you might assume teething is the culprit, but look for signs of a sore throat as well. Your body produces extra saliva when your throat is irritated to soothe it. Since babies have limited ways of communicating, keep an eye on her or him grabbing at their ears or neck.
3. Allergies
Allergies can cause excessive saliva production and drooling, as the body is trying to flush out toxins. Watch for signs of allergic reactions to foods once your baby has started solids and observe if excessive drooling occurs after exposure to animals or certain environments. Most allergic reactions can be safely treated at home but check with your doctor before giving your child antihistamines or other allergy medications. Call 911 if your child has an anaphylactic reaction, which generally occurs within minutes of being exposed to an allergen.
4. Choking
Any signs of choking while drooling should be taken seriously. Check for obstructions and call 911 or your local emergency number. Do not hesitate to get your baby immediate attention if something appears to be wrong or if she or he is having difficulty breathing.
Check for obstructions and call 911 or your local emergency number. Do not hesitate to get your baby immediate attention if something appears to be wrong or if she or he is having difficulty breathing.
5. Stroke, neurological disease, facial paralysis
While very rare in babies and children, strokes, neurological diseases, and paralysis from diseases like Bell’s palsy can occasionally occur. They’re not things to worry about on a day-to-day basis but shouldn’t be completely ruled out if your baby has other symptoms that indicate a problem. Rest assured, however, that your baby’s drool is unlikely to be from something serious.
Final Thoughts
Drooling is a natural response to growth and development and some babies naturally drool more than others. By around age two, most children have stopped drooling, since their digestive system is fully developed, and they have most of their baby teeth.
Use soft cloths and bibs to keep your baby’s face and clothes dry, do your best to prevent drool rash, and treat drool rash appropriately if it occurs. Check with your pediatrician for specific treatments she or he recommends. While most often drooling is simply from teething or development, watch for signs of something more serious and contact your doctor or call emergency services if you have more significant concerns.
Check with your pediatrician for specific treatments she or he recommends. While most often drooling is simply from teething or development, watch for signs of something more serious and contact your doctor or call emergency services if you have more significant concerns.
Paper Pinecone is the #1 most trusted childcare directory giving parents access to the best preschools and best daycares near you. Parents always search free and childcare providers always list free. Send inquiries about the best daycares and preschools to [email protected].
This post may contain affiliate links.
Study shows ‘saliva sharing’ shapes babies’ view of close relationships
In the Lab
By Andrew Joseph Jan. 20, 2022
Reprints
A young child’s exposure to family members’ spit plays a crucial role in how we make sense of the world around us, a new study shows.
Adobe
Raising a young child can be a bit … messy. There’s the drool to be wiped, the slobbery feeding and sharing of utensils — and plenty of kisses.
But it turns out that all that exposure to family members’ spit — what, in academic parlance, is known as “saliva sharing” — plays a crucial role in how we make sense of the world around us, a new study shows. It helps shape our discernment of social relationships, starting from our first months of life.
The study — with infants, toddlers, and young children as participants — found that we use saliva sharing as a cue to help distinguish “thick” relationships. These are connections in which people have strong attachments and feel a sense of obligation for the other — and in which someone is expected to respond when the other is in trouble. They are distinct from other close relationships, like certain friendships; often, though not always, they are with family.
advertisement
Moreover, the study, published Thursday in the journal Science, determined that saliva sharing wasn’t just how the participants defined who was close to themselves: When they saw saliva sharing among another adult and another child (well, really, in the case of the study, a puppet), they expected that adult to provide comfort when the puppet signaled it was in distress.
“We’re asking how they think about relationships,” and not just their own, said developmental psychologist Ashley Thomas of Massachusetts Institute of Technology, the lead author of the paper.
advertisement
Other factors beyond saliva sharing certainly inform our categorization of relationships and degrees of intimacy, Thomas said. But there’s something specific about spit. The study didn’t just include normal instances of saliva sharing, like licking the same ice cream cone or using the same straw. In one experiment, participants watched as an adult wiped the inside of her own mouth with her finger, then the inside of the puppet’s mouth, and then her own mouth again. That’s not an everyday behavior babies see — and yet they still understood it as a sign of a thick bond.
“One question developmental psychologists have been trying to answer is how infants and young children begin to parse the world into a structure that they can effectively use in order to make important decisions like whom to learn from,” Zoe Liberman, an assistant professor of psychological and brain sciences at the University of California, Santa Barbara, wrote in an email.
Liberman, who was not involved in the new study, wrote that studies have shown children pick up on close versus distant relationships, but haven’t been as clear about whether they differentiate among varying degrees of close relationship. “This work is exciting because it clearly shows at least one domain in which really young children, and even infants, are making different inferences about ‘thick’ relationships, like family members, compared to other close relationships.”
The study doesn’t address the question of whether recognizing saliva sharing as a proxy for thick relationships is something we innately know or we figure out. But some study participants were quite young, so “at the very least, they’re able to rapidly learn this connection,” Thomas said.
We’re typically turned off by others’ saliva, perhaps because we’ve evolved to be concerned about pathogens (as if we needed a reminder after two years of physical distancing). But perhaps we put that fear aside when we are dealing with those closest to us.
“Humans may have adaptations that lead them to only engage in saliva sharing with people in these ‘thick’ relationships,” Liberman wrote. That could be why it’s such an important signal to babies — they associate the people who expose themselves to their saliva (those who wipe their drool or feed them) as their caregivers.
In an editorial also published Thursday in Science, Christine Fawcett of the Uppsala Child and Baby Lab in Sweden raised a similar point.
“It has been proposed that the emotion of disgust evolved to protect us from contamination, such as can occur when coming into contact with the bodily fluids of another person,” she wrote. “Yet taking care of an infant, for example, requires such contact, so we may have also evolved an exception to the rule: Those in our closest, thickest relationships do not elicit disgust in us, no matter the amount of drool or dirty diapers they produce.”
As an example, Fawcett pointed to one study that showed parents find the smell of their own kids’ dirty diapers less disgusting than those soiled by other children.
For the new study, Thomas and developmental psychologist colleagues at Harvard and MIT had a hunch that babies might be cued by saliva sharing to determine thick relationships, a notion backed by other fields like anthropology that have found that the sharing of fluids like saliva or breast milk is a sign of intimate bonds in some cultures. The researchers then designed a series of experiments to test that hypothesis.
In one experiment, for example, children from 5 to 7 years old looking at cartoons were more likely to predict that saliva sharing actions (like drinking from the same straw) would occur with nuclear family members than with friends, whereas actions like sharing toys would happen with both family and friends.
In another experiment, infants and toddlers ranging from 8 to 18 months watched as a puppet “ate” from the same orange slice as one actress and played ball with a different actress. When the puppet then started signaling distress, the infants and toddlers looked to the orange-slice-sharing actress first and longest, “as though expecting the actress to react to the puppet’s distress,” the researchers wrote. (The experiment was modeled on prior studies that have shown that when a vervet monkey is in distress, other monkeys look to its mother to respond.)
(The experiment was modeled on prior studies that have shown that when a vervet monkey is in distress, other monkeys look to its mother to respond.)
When that puppet was swapped out for a different puppet that then expressed distress, the infants and toddlers didn’t look to the orange-slice-sharing actress first or longer compared to the ball-playing actress. These findings suggest that the children’s expectations about who would respond were tied to the saliva-sharing relationship, not whether they viewed the person as simply nice, Thomas said.
“Saliva-sharing interactions provide externally observable cues of thick relationships, and young humans can use these cues to make predictions about subsequent social interactions,” the researchers wrote.
The whole series of experiments included different participants, but as the study went on, the researchers recruited a more geographically, racially, and economically representative cohort. All the participants, however, came from the United States. While saliva sharing could be a universal cue, Thomas noted that norms around saliva and who is considered family are different around the world — and so might be what seeing a saliva-sharing relationship means.
While saliva sharing could be a universal cue, Thomas noted that norms around saliva and who is considered family are different around the world — and so might be what seeing a saliva-sharing relationship means.
“It could be that variation in parenting practices across, or within, cultures leads to variation in children’s expectations about thick relationships,” Fawcett wrote in the editorial.
About the Author
Reprints
Create a display name to comment
This name will appear with your comment
Babies can tell who has close relationships based on one clue: saliva | MIT News
Learning to navigate social relationships is a skill that is critical for surviving in human societies. For babies and young children, that means learning who they can count on to take care of them.
MIT neuroscientists have now identified a specific signal that young children and even babies use to determine whether two people have a strong relationship and a mutual obligation to help each other: whether those two people kiss, share food, or have other interactions that involve sharing saliva.
In a new study, the researchers showed that babies expect people who share saliva to come to one another’s aid when one person is in distress, much more so than when people share toys or interact in other ways that do not involve saliva exchange. The findings suggest that babies can use these cues to try to figure out who around them is most likely to offer help, the researchers say.
“Babies don’t know in advance which relationships are the close and morally obligating ones, so they have to have some way of learning this by looking at what happens around them,” says Rebecca Saxe, the John W. Jarve Professor of Brain and Cognitive Sciences, a member of MIT’s McGovern Institute for Brain Research and the Center for Brains, Minds, and Machines (CBMM), and the senior author of the new study.
MIT postdoc Ashley Thomas, who is also affiliated with the CBMM, is the lead author of the study, which appears today in Science. Brandon Woo, a Harvard University graduate student; Daniel Nettle, a professor of behavioral science at Newcastle University; and Elizabeth Spelke, a professor of psychology at Harvard and CBMM member, are also authors of the paper.
Sharing saliva
In human societies, people typically distinguish between “thick” and “thin” relationships. Thick relationships, usually found between family members, feature strong levels of attachment, obligation, and mutual responsiveness. Anthropologists have also observed that people in thick relationships are more willing to share bodily fluids such as saliva.
“That inspired both the question of whether infants distinguish between those types of relationships, and whether saliva sharing might be a really good cue they could use to recognize them,” Thomas says.
To study those questions, the researchers observed toddlers (16.5 to 18.5 months) and babies (8.5 to 10 months) as they watched interactions between human actors and puppets. In the first set of experiments, a puppet shared an orange with one actor, then tossed a ball back and forth with a different actor.
After the children watched these initial interactions, the researchers observed the children’s reactions when the puppet showed distress while sitting between the two actors. Based on an earlier study of nonhuman primates, the researchers hypothesized that babies would look first at the person whom they expected to help. That study showed that when baby monkeys cry, other members of the troop look to the baby’s parents, as if expecting them to step in.
Based on an earlier study of nonhuman primates, the researchers hypothesized that babies would look first at the person whom they expected to help. That study showed that when baby monkeys cry, other members of the troop look to the baby’s parents, as if expecting them to step in.
The MIT team found that the children were more likely to look toward the actor who had shared food with the puppet, not the one who had shared a toy, when the puppet was in distress.
In a second set of experiments, designed to focus more specifically on saliva, the actor either placed her finger in her mouth and then into the mouth of the puppet, or placed her finger on her forehead and then onto the forehead of the puppet. Later, when the actor expressed distress while standing between the two puppets, children watching the video were more likely to look toward the puppet with whom she had shared saliva.
Social cues
The findings suggest that saliva sharing is likely an important cue that helps infants to learn about their own social relationships and those of people around them, the researchers say.
“The general skill of learning about social relationships is very useful,” Thomas says. “One reason why this distinction between thick and thin might be important for infants in particular, especially human infants, who depend on adults for longer than many other species, is that it might be a good way to figure out who else can provide the support that they depend on to survive.”
The researchers did their first set of studies shortly before Covid-19 lockdowns began, with babies who came to the lab with their families. Later experiments were done over Zoom. The results that the researchers saw were similar before and after the pandemic, confirming that pandemic-related hygiene concerns did not affect the outcome.
“We actually know the results would have been similar if it hadn’t been for the pandemic,” Saxe says. “You might wonder, did kids start to think very differently about sharing saliva when suddenly everybody was talking about hygiene all the time? So, for that question, it’s very useful that we had an initial data set collected before the pandemic. ”
”
Doing the second set of studies on Zoom also allowed the researchers to recruit a much more diverse group of children because the subjects were not limited to families who could come to the lab in Cambridge during normal working hours.
In future work, the researchers hope to perform similar studies with infants in cultures that have different types of family structures. In adult subjects, they plan to use functional magnetic resonance imaging (fMRI) to study what parts of the brain are involved in making saliva-based assessments about social relationships.
The research was funded by the National Institutes of Health; the Patrick J. McGovern Foundation; the Guggenheim Foundation; a Social Sciences and Humanities Research Council Doctoral Fellowship; MIT’s Center for Brains, Minds, and Machines; and the Siegel Foundation.
What Is a Drool Rash? Learn about symptoms, treatment, and more
Written by Victoria Hamilton
In this Article
- Symptoms of a Drool Rash
- Causes of a Drool Rash
- Treating a Drool Rash
- Preventing a Drool Rash
- Drool Rash vs.
 Eczema
Eczema - Other Common Rashes in Newborns
- When to See a Doctor for Drool Rash
 Eczema
Eczema Drooling is common in babies, whether they’re teething or not. Continual drooling, though, means that there is constantly saliva on your baby’s cheeks, chin, neck, and chest. This is not good for the skin and often results in a drool rash.
Symptoms of a Drool Rash
Your baby’s new skin is sensitive – it’s not uncommon for them to develop a rash. Drool rashes, also known as newborn rashes, appear on the face and neck area. Drool rash symptoms include small patches of raised, red bumps, and the skin may look dry and chapped.
The drool rash might not always be present. It’s normal for this condition to come and go.
Causes of a Drool Rash
The cause of drool rashes is straightforward: Saliva settles on your baby’s skin, and over time, the drool irritates their delicate chin, cheeks, mouth, neck, and more. Pacifiers and teething rings are connected with drool rashes because it promotes close contact between saliva and the skin.
Newborn rashes are typical for babies who are teething because excessive drool is a symptom of cutting new teeth. Drooling is certainly a sign of new teeth coming in, but your baby’s salivary glands will continuously develop when they’re only a few months old. From this point on, they may drool excessively whether they’re getting teeth or not.
Be mindful of the food that you give to your baby if they are teething or if they naturally salivate a lot. Some foods are irritating to the skin and can worsen the rash. After your child is done eating, make sure to clean their skin gently but thoroughly. If you use scented baby wipes, lotions, or body washes, opt for an alternative with less irritating ingredients.
Treating a Drool Rash
Drool rash is treatable at home. The best thing you can do is limit the amount of contact between saliva and your baby’s skin. Consider the following options if you need a drool rash treatment:
- Use bibs to absorb saliva, and remember to change the bibs regularly.
- Wash your baby’s face gently with warm water and a soft cloth a few times a day to remove saliva or leftover food. Pat the face dry.
- Avoid rubbing the area excessively and using harsh ingredients that could irritate the rash further.
- Apply a healing ointment, like Aquaphor or petroleum jelly, to completely dry skin.
- Adjust what you put on your own skin. Your body wash, perfume, or laundry detergent could irritate your child as you come into contact with them.

Above all else, keep your baby’s comfort in mind. If you use a bib or cloth that’s too rough, wash the area too frequently, etc., you will only worsen their condition.
Preventing a Drool Rash
Drooling is natural! It’s impossible to prevent saliva from coming into contact with your baby’s skin. Focus on keeping your baby’s skin clean and dry and minimizing the uncomfortable effects of a rash:
- Keep a dry, soft burp cloth on hand to continually absorb drool.
- Change your baby’s clothes if they become soaked with saliva.
- Apply a thin coat of petroleum jelly to potential problem areas (face, cheeks, neck, chest, etc.). This will protect the skin from drool, seal in moisture, and soothe dry skin.
- Take away your baby’s pacifier or teething toys to reduce the amount of time that saliva rests on your baby’s skin.
- Review the substances that come into contact with your baby’s skin. Avoid products with dyes and fragrances.
- Don’t wait too long to clean your baby’s face or chest area from food or drool.

Drool Rash vs. Eczema
A drool rash is often mistaken for eczema, and vice versa. Eczema, also known as atopic dermatitis, manifests as red, irritated, dry skin and looks similar to a drool rash. If the eczema is severe, your baby may also develop sores that ooze and cracked skin. It’s common for babies to develop eczema at some point in the first few months of life!
Atopic dermatitis is likely to show up on your baby’s face, scalp, knees, and elbows. Essentially, you could find eczema anywhere on their body except for the diaper area due to increased moisture levels here. Meanwhile, studies show that 75% of babies that develop eczema also have hay fever symptoms, like ear pressure, a runny nose, or itchy eyes.
Meanwhile, studies show that 75% of babies that develop eczema also have hay fever symptoms, like ear pressure, a runny nose, or itchy eyes.
It’s unknown what causes eczema, but babies with a family history of hay fever or eczema are more likely to develop this skin condition. It’s also possible that eczema is the body’s response to allergens. If your baby is allergic to something in their food or environment, they may get eczema as a result.
Drool rashes share a few similarities with eczema, but the causes and treatments are different. Learning what is a drool rash will be helpful so you can quickly diagnose your child’s skin irritation and begin treatment.
Other Common Rashes in Newborns
There are many kinds of rashes common to new babies. As your baby’s delicate skin adjusts to its new environment and you do your best to care for it, keep these rashes and birthmarks in mind:
- Newborn acne
- Erythema toxicum
- Bruising or scrapes from birthing
- Milia
- Mongolian spots
- Stork bites
After their first bath, your newborn will develop a ruddy complexion because of an increased number of red blood cells. Similarly, if they get too cold they’ll start to look a little pale or blue. As time goes on, their skin will likely dry out and start to flake, followed by the appearance of any number of rashes or birthmarks.
Similarly, if they get too cold they’ll start to look a little pale or blue. As time goes on, their skin will likely dry out and start to flake, followed by the appearance of any number of rashes or birthmarks.
When to See a Doctor for Drool Rash
If your baby has developed a drool rash, try to treat it at home before consulting your child’s doctor. If symptoms worsen or include the following, reach out to their healthcare provider as soon as possible:
- Rash that cracks and causes pain
- Sores or blisters that ooze
- Lack of appetite
- Fevers
If the rash doesn’t appear to be getting better after a week or so, contact their healthcare provider. If your baby has a rash and it is accompanied by difficulty breathing, they are likely having an allergic reaction to food or their environment. Seek medical help immediately.
Why Does My Baby Drool Too Much?
Blog search
Blog categories
Latest Comments
No comments
Posted on07/12/2021
47494
Love1
It’s no secret that infants drool. While adults’ drooling is typically regarded as odd and uncivilized, infant drool is adorable and reassuring. Few people ponder about why their lovely newborns are drooling, but most just let it happen without question. It’s just one of those unattractive things that come with infancy, like spit-up, filled diapers, and snot.
While adults’ drooling is typically regarded as odd and uncivilized, infant drool is adorable and reassuring. Few people ponder about why their lovely newborns are drooling, but most just let it happen without question. It’s just one of those unattractive things that come with infancy, like spit-up, filled diapers, and snot.
By the time your child is two months old, you may have accumulated an increasing number of damp blankets, drool rags, and onesies. Sure, constant drooling might be a nuisance, but it isn’t simply a slick, slippery annoyance—infant saliva performs several crucial functions in your child’s growth. Here are some of the most often asked questions regarding drool, along with their simple, ahem, answers:
Is Babies’ Drooling Common?
If your kid has started drooling, you should anticipate it to last until he is 18 to 24 months old. Drooling is frequent throughout the teething stage, so plan on changing your baby’s clothing 5-6 times each day. Drooling is extremely frequent in babies. However, if a youngster drools after the age of four, it is not normal.
Drooling is extremely frequent in babies. However, if a youngster drools after the age of four, it is not normal.
Should I Be Worried About My Baby Excessively Drooling?
Excessive drooling does exist, but it can be difficult to determine if your baby’s drool is abnormal or not. Excessive drool, on the other hand, isn’t something you should be too concerned about because it’s probably benefiting your kid more than hurting him.
Saliva is generated in order to clean the gums and teeth of food and bacteria. More germs are wiped away when a newborn drools heavily. Saliva also aids in the breakdown of specific molecules in the meals your kid consumes, thus creating too much will benefit his stomach.
Excessive drooling is nothing to be alarmed about as long as your kid is making normal developmental growth in other areas, and you should only be concerned if the drool is creating other difficulties.
Is Excessive Drooling an Autism Symptom?
Along with developmental delays, one of the symptoms that children diagnosed with autism typically face is trouble with muscular control and sensitivity. Drooling is a pretty typical sign in children with autism because they have difficulties regulating their facial muscles.
Drooling is a pretty typical sign in children with autism because they have difficulties regulating their facial muscles.
Drooling therapy methods for autistic children must be individually adapted to the child.
What Should I Do If Drool Irritates Baby?
Sometimes drool can lead to a rash around the baby’s mouth, owing to irritation that arises from excess moisture.
If this occurs with your infant, attempt to gently wipe away the drool so it does not remain on the baby’s face for too long. You should also consider applying ointment to the afflicted area at night.
Finally, there is nothing you can do to stop your infant from drooling. It is, after all, a normal and healthy aspect of a baby’s growth!
Related products
Waterproof bib
JANABEBE
€23.00 (tax incl.)
New product! Protect your baby from saliva, liquids or food with this new waterproof bib. Choose the shape and print you like best.
Bib 100% waterproof cotton
JANABEBE
€15.00 (tax incl.)
New version of our 100% cotton waterproof bib for the little ones at home. Made of cotton and with a double waterproof layer. The pack contains the three prints: Pack 1: Zebra, African Sunset and Bloom. Pack 2:…
Curl Bib 3-pack
JANABEBE
€14.00 (tax incl.)
With this pack you can prevent your baby from dirt for a long time. The bibs are made of 100% cotton and with a double waterproof layer.
Baby chair cushion for Stokke Tripp Trapp
JANABEBE
€46.50 (tax incl.)
Janabebé Stokke Tripp Trapp highchair cushion, for your child to discover true softness and maximum comfort at mealtime. Available in a variety of our prints so you can choose the one that best suits your little one.
Cover for Ikea ANTILOP baby chair
JANABEBE
€36.50 (tax incl.)
Our Ikea highchair mattress is made of soft cotton fabric in contact with the skin of your little one and airconfort technical fabric on the back, which allows free circulation of air so that your baby is always cool. ..
Cushion for Highchair I-dea
JANABEBE
€39.00 (tax incl.)
In this new stage of great changes of the baby in which he already begins to be sitting in his highchair and sharing and interacting more with all members of the family, as it is mealtime, the baby has to feel…
Related articles
Previous article Next article
Leave a Comment
Leave a Reply
Please login to post a comment.
Parents’ Saliva On Pacifiers Could Ward Off Baby’s Allergies : Shots
Parents’ Saliva On Pacifiers Could Ward Off Baby’s Allergies : Shots – Health News Instead of rinsing off the pacifier when it falls out of your baby’s mouth, new research suggests that sucking it clean for them could help keep them from developing eczema and asthma. Researchers say the harmless bacteria in parents’ saliva works by stimulating the babies’ immune system.
The Human Microbiome: Guts And Glory
Heard on Morning Edition
Parents’ Saliva On Pacifiers Could Ward Off Baby’s Allergies
Sucking may be one of the most beneficial ways to clean a baby’s dirty pacifier, a study found
iStockphoto. com
com
hide caption
toggle caption
iStockphoto.com
Sucking may be one of the most beneficial ways to clean a baby’s dirty pacifier, a study found
iStockphoto.com
That word “microbiome” — describing the collection of bacteria that live in and on our bodies — keeps popping up. This time, researchers say that children whose parents clean their pacifiers by sucking them might be less likely to develop allergic conditions because of how their parents’ saliva changes their microbiomes.
That’s the word from a small study of 184 Swedish babies published in this week’s issue of the journal Pediatrics. The researchers found that the 65 babies whose mother or father sucked on their pacifiers to cleanse them were significantly less likely to get eczema and asthma, two conditions caused by allergic reactions, than babies whose parents did not use the cleaning technique.
“This is a really interesting and intriguing observation,” says Elizabeth Matsui of the Johns Hopkins Children’s Center, who was not involved in the research.
The findings add credence to a growing body of evidence that suggests that exposure, or the lack of exposure, to microbes early in life can affect a child’s health by influencing his or her microbiome.
“There’s recently been an explosion of interest in the microbiome and how it might influence many things — but in particular someone’s propensity to develop an allergic disease,” Matsui says.
To investigate the role of pacifier cleaning, Bill Hesselmar of the University of Gothenburg in Sweden and his colleagues analyzed data they had collected for a broader study about babies’ allergies. Among the questions the parents had answered was what they did when their child’s pacifier fell out of his or her mouth.
“We asked them how they cleaned the pacifier — if they rinsed them in water — and of course most of them did,” Hesselmar says. But a lot of the parents did something else.
But a lot of the parents did something else.
“They put it in their mouth, sucked on it and then gave it back to the children,” Hesselmar says. “It’s a quite common way to clean pacifier.”
When the researchers checked to see if there were any differences between the kids whose parents sucked their pacifiers clean and those who didn’t, they found there was. Those whose parents sucked the pacifiers clean were significantly less likely to have developed eczema at 18 and 36 months and less likely to have developed asthma at 18 months, the researchers say.
“Eczema is the best disease to choose [as a marker] if you want to see if a young child is becoming allergic,” Hesselmar says.
Scientists think that when parents suck their child’s pacifier clean, they transfer some of the harmless bacteria in their mouths to their child, Hesselmar says. In fact, the researchers found evidence supporting that when they analyzed the saliva of the babies in the study.
“We think that these bacteria . .. stimulate the immune system,” Hesselmar says. And that teaches it how to do its job properly, which includes not overreacting to things like peanuts, pollen and cats, he says.
.. stimulate the immune system,” Hesselmar says. And that teaches it how to do its job properly, which includes not overreacting to things like peanuts, pollen and cats, he says.
The study adds to a growing body of evidence that lots of kids these days may be growing up essentially too clean, Matsui says.
“We are much less likely to be exposed to organisms in water — parasites, for example — so the idea is there is much less for the immune system to fight off. So it starts reacting to things that perhaps it should be ignoring,” Matsui says.
Amanda Sauer, 35, of Washington, D.C., uses a pacifier when her 2-year-old son, Leo, gets fussy. When it falls to the ground she often washes it off.
Sauer’s not sure the new research will make her start licking Leo’s dirty pacifier.
“Probably not,” she says. “But it’s more for just the fact that I don’t really want to put a pacifier in my mouth. But sometimes the dog cleans it off for us, so maybe that’s just as good.”
Sponsor Message
Become an NPR sponsor
Sialorrhoea in patients with cerebral palsy: effectiveness of botulinum therapy | Klochkova
1. Bax M., Goldstein M., Rosenbaum P., Leviton A., Paneth N., Dan B., Jacobsson B., Damiano D. Proposed definition and classification of cerebral palsy. Dev Med Child Neurol. 2005; 47(8): 571–576.
Bax M., Goldstein M., Rosenbaum P., Leviton A., Paneth N., Dan B., Jacobsson B., Damiano D. Proposed definition and classification of cerebral palsy. Dev Med Child Neurol. 2005; 47(8): 571–576.
2. Johnson H., Scott A. Saliva Management. In Dysphagia: Foundation, Theory and Practice. Eds. Cichero J. A. Y., Murdoch B. F. Chichester: J Wiley & Sons, Ltd. 2006. 126 rubles.
3. Levitsky G. N., Alekhin A. V., Serdyuk A. V., Morgunova M. S., Koneva O. N., Skvortsova V. I. Possibilities of drug therapy of salivation in motor neuron disease. Journal of Neurology and Psychiatry. C. S. Korsakov. 2005; 105(3): 19–22.
4. Blasco P. A., Allaire J. H. Drooling in the developmentally disabled: management practices and recommendations. Consortium on Drooling. Dev Med Child Neurol. 1992; 34(10): 849–862.
5. Ber M., Frotscher M. Topical diagnosis in neurology according to Peter Duus: anatomy, physiology, clinic. Per. from English. Ed. Z. A. Suslina. 4th ed. Moscow: Practical medicine. 2009. pp. 163–164.
2009. pp. 163–164.
6. Scully C., Limeres J., Gleeson M., Tomas I., Diz P. Drooling. J Oral Pathol Med. 2009; 38(4): 321–327.
7. Erasmus C. E., Van Hulst K., Rotteveel L. J., Jongerius P. H., Van Den Hoogen F. J., Roeleveld N., Rotteveel J. J. Drooling in cerebral palsy: hypersalivation or dysfunctional oral motor control? Dev Med Child Neurol. 2009; 51(6): 454–459.
8. Tahmassebi J. F., Curzon M. E. The cause of drooling in children with cerebral palsy hypersalivation or swallowing defect? Int J Paediatr Dent. 2003; 13(2): 106–111.
9. Dodds W. J. Physiology of swallowing. Dysphagia. 1989; 3:171–178.
10. Senner J. E., Logemann J., Zecker S., Gaebler-Spira D. Drooling, saliva production, and swallowing in cerebral palsy. Dev Med Child Neurol. 2004; 46(12): 801–806.
11. Tahmassebi J. F., Curzon M. E. Prevalence of drooling in children with cerebral palsy attending special schools. Dev Med Child Neurol. 2003; 45(9): 613–617.
12. Parkes J., Hill N., Platt M. J., Donnelly C. Oromotor dysfunction and communication impairments in children with cerebral palsy: a register study. Dev Med Child Neurol. 2010; 52(12): 1113–1119.
Parkes J., Hill N., Platt M. J., Donnelly C. Oromotor dysfunction and communication impairments in children with cerebral palsy: a register study. Dev Med Child Neurol. 2010; 52(12): 1113–1119.
13. Lin Y. C., Shieh J. Y., Cheng M. L., Yang P. Y. Botulinum toxin type A for control of drooling in Asian patients with cerebral palsy. Neurology. 2008; 70(4): 316–318.
14. Lakraj A. A., Moghimi N., Jabbari B. Sialorrhea: anatomy, pathophysiology and treatment with emphasis on the role of botulinum toxins. Toxins (Basel). 2013; 5(5): 1010–1031.
15. Fairhurst C. B., Cockerill H. Management of drooling in children. Arch Dis Child Educ. Pract Ed. 2011; 96(1): 25–30.
16. Klochkova O. A., Kurenkov A. L., Namazova-Baranova L. S., Mamedyarov A. M. Spasticity patterns of the muscles of the upper limbs and the use of botulinum therapy in patients with cerebral palsy with hand involvement. Pediatric pharmacology. 2013; 10(5):31–39.
17. Reddihough D., Erasmus C. E., Johnson H., McKellar G. M., Jongerius P. H. Cereral Palsy Institute. Botulinum toxin assessment, intervention and aftercare for pediatric and adult drooling: international consensus statement. Eur J Neurol. 2010; 17 (Suppl. 2): 109-121.
E., Johnson H., McKellar G. M., Jongerius P. H. Cereral Palsy Institute. Botulinum toxin assessment, intervention and aftercare for pediatric and adult drooling: international consensus statement. Eur J Neurol. 2010; 17 (Suppl. 2): 109-121.
18. Naumann M., So Y., Argoff C. E., Childers M. K., Dykstra D. D., Gronseth G. S., Jabbari B., Kaufmann H. C., Schurch B., Silberstein S. D., Simpson D. M. Botulinum neurotoxin in the treatment of autonomic disorders and pain (an evidence based review): report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2008; 70(19): 1707–1714.
19. Rodwell K., Edwards P., Ware R. S., Boyd R. Salivary gland botulinum toxin injections for drooling in children with cerebral palsy and neurodevelopmental disability: a systematic review. Dev Med Child Neurol. 2012; 54 (11): 977–987.
20. Naumann M., Dressler D., Hallett M., Jankovic J., Schiavo G., Segal K. R., Truong D. Evidence based review and assessment of botulinum neurotoxin for the treatment of secretory disorders. Toxicon. 2013; 67:141–152.
Toxicon. 2013; 67:141–152.
21. Walshe M., Smith M., Pennington L. Interventions for drooling in children with cerebral palsy. Cochrane Database Syst Rev. 2012; 2: CD008624. Doi: 10.1002/14651858.CD008624.pub2.
22. Nosko AS, Zykov VP, Komarova IB Correction of sialorrhea in neuropediatrics. Focus on botulinum toxin type A preparations as the first line of choice. Child and adolescent rehabilitation. 2013; 2(21):33–38.
23. Palisano R., Rosenbaum P. L., Walter S., Russell D., Wood E., Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997; 39(4):214–223.
24. Reid S. M., Johnson H. M., Reddihough D. S. The Drooling Impact Scale: a measure of the impact of drooling in children with developmental disabilities. Dev Med Child Neurol. 2010; 52(2):23–28.
25. Reid S. M., Johnstone B. R., Westbury C., Rawicki B., Reddihough D. S. Randomized trial of botulinum toxin injections into the salivary glands to reduce drooling in children with neurological disorders. Dev Med Child Neurol. 2008; 50(2):123–128.
Dev Med Child Neurol. 2008; 50(2):123–128.
26. Banerjee K. J., Glasson C., O’Flaherty S. J. Parotid and submandibular botulinum toxin A injections for sialorrhoea in children with cerebral palsy. Dev Med Child Neurol. 2006; 48(11): 883–887.
27. Savarese R., Diamond M., Elovic E., Millis S. R. Intraparotid injection of botulinum toxin A as a treatment to control sialorrhea in children with cerebral palsy. Am J Phys Med Rehabil. 2004; 83(4): 304–311.
28. Alrefai A. H., Aburahma S. K., Khader Y. S. Treatment of sialorrhea in children with cerebral palsy: a double blind placebo controlled trial. Clin Neurol Neurosurg. 2009; 111(1): 79–82.
29. Lagalla G., Millevolte M., Capecci M., Provinciali L., Cera volo M. G. Botulinum toxin type A for drooling in Parkinson’s disease: a double blind, randomized, placebo controlled study. mov discord. 2006; 21(5): 704–707.
30. Kalf J. G., Smit A. M., Bloem B. R., Zwarts M. J., Mulleners W. M., Munneke M. Botulinum toxin A for drooling in Parkinson’s disease: a pilot study to compare submandibular to parotid gland injections. Parkinsonism Relat Disord. 2007; 13(8): 532–534.
Parkinsonism Relat Disord. 2007; 13(8): 532–534.
31. Jongerius P. H., van den Hoogen F. J., van Limbeek J., Gabreels F. J., van Hulst K., Rotteveel J. J. Effect of botulinum toxin in the treatment of drooling: a controlled clinical trial. Pediatrics. 2004; 114(3): 620–627.
32. Harris S. R., Purdy A. H. Drooling and its management in cerebral palsy. Dev Med Child Neurol. 1987; 29(6): 807–811.
33. Erasmus C. E., Scheffer A. R., van Hulst K., van Limbeek J., van den Hoogen F. J., Rotteveel J. J., Jongerius P. H. Does motor perfor mance matter in botulinum toxin efficacy for drooling? Pediatric Neurol. 2011; 45(2):95–99.
Why does a child grind his teeth in his sleep
Teeth grinding (bruxism) is a common problem in children that causes concern to parents. This phenomenon does not apply to diseases. This is a symptom that signals various failures in the endocrine, digestive and nervous systems of the child’s body. Here it is necessary to pay attention to other changes in the behavior of the child. The exact cause can only be established by a doctor after a thorough examination.
The exact cause can only be established by a doctor after a thorough examination.
In the article we will try to find out why a child can grind his teeth, how dangerous it is, and what to do in this case.
What is bruxism and its manifestations
Bruxism is a pathological condition that occurs due to excessive compression of the jaws.
Under the age of 5 years, grinding of the teeth is observed in almost 50% of children. This happens involuntarily, and is associated with a spasm of the masticatory muscles. Usually, the pathology occurs at night, paroxysmal for 10-15 seconds. Attacks can be repeated in the daytime. At the same time, daily grinding of teeth gives parents more anxiety, as it is more noticeable.
Help! Sporadic cases of teeth grinding are not dangerous and do not require intervention. If the attacks become chronic, the help of a pediatrician is needed.
In addition to squeaking teeth, the following manifestations of pathology are possible in a child:
-
headache;
-
daytime sleepiness, lethargy;
-
pain in the neck;
-
tearfulness;
-
tooth sensitivity – the result of their abrasion and damage to the enamel;
-
restless sleep with frequent awakenings;
-
ear congestion.

Dentists identify a triad of symptoms in childhood bruxism (up to 5 years). This is erosive abrasion of milk teeth, malocclusion and narrowing of the dental arches. Teeth grinding usually goes away on its own when the child reaches puberty. In adolescents and young people, grinding their teeth is a rare occurrence.
Call right now
+7 (495) 215-58-10
Make an appointment with a doctor
Causes of teeth grinding in sleep
Until the end, the exact causes of pathological grinding of teeth have not been clarified. In most cases, seizures occur at night, so sleep disturbances are a common cause. In children, this is associated with hypertrophy of the tonsils and adenoids, which makes nasal breathing difficult and leads to apnea (suspension of breathing during sleep). Obesity is also a contributing factor.
Other possible reasons why a child may grind their teeth include:
-
Incorrect deep bite.
-
Individual characteristics of the inclination of the lower jaw.
-
Nervous tension, emotional overexcitation.
-
hereditary predisposition.
-
Neurological or endocrine disorders.
-
Teething.

Causes and manifestations may vary depending on what time of day bruxism occurs.
Night grinding of teeth
If during sleep you notice several seizures, and at the same time the child behaves restlessly (breathing becomes more frequent, pupils actively move, talks), then the reason is emotional overexcitation. More often this manifests itself in emotionally sensitive children, overly active or with hyperexcitability syndrome.
Stress can also provoke night bruxism – moving to a new apartment, entering a kindergarten, divorce of parents or frequent scandals at home. In the daytime, the child tries not to show his emotions and tension accumulates, and at night it “splashes out” through clenching of the jaws and grinding of teeth.
In some cases, an ordinary seal, which was installed incorrectly, can become a provocateur. It can interfere with the tight closure of the jaw, and the child is too small to tell about it. Difficulty in nasal breathing and snoring in a child’s sleep is a sign of problems with the adenoids. In this case, you need to consult an ENT doctor.
Grinding teeth during daytime
In the afternoon, a spasm of the masticatory muscles in a baby may occur due to teething. It is also possible to form a malocclusion, which leads to discomfort and clenching of the jaws. In these situations, you need to show the child to the dentist.
During a stressful situation, involuntary grinding of teeth is possible. Observe when the child has this phenomenon during the day, what precedes it. With frequent attacks, it is recommended to consult a child psychologist or neurologist. Digestive and endocrine problems can also cause daytime bruxism.
What about worms?
There is a widespread belief that teeth grinding can be a sign of a parasitic disease. This is due to the fact that preschool children often suffer from helminths. And it is for this age that creaking of teeth is characteristic. Also, this assumption was explained by the fact that when infected with helminths, salivation increases. This provokes the compression of the jaws, which leads to the grinding of the teeth. But according to research experts, this is just a coincidence. A direct relationship between the presence of worms in a child and bruxism has not been identified.
This is due to the fact that preschool children often suffer from helminths. And it is for this age that creaking of teeth is characteristic. Also, this assumption was explained by the fact that when infected with helminths, salivation increases. This provokes the compression of the jaws, which leads to the grinding of the teeth. But according to research experts, this is just a coincidence. A direct relationship between the presence of worms in a child and bruxism has not been identified.
Is bruxism dangerous and what are the consequences
Bruxism does not lead to serious health problems, and even more so does not threaten the development and life of the child. Most of all, parents are worried about this phenomenon, and they begin a hospital quest in search of the cause. As a rule, the child grows out of this problem without the participation of a doctor, if it is not chronic. This is due to the development of the chewing apparatus, the elimination of problems with adenoids and the normalization of sleep.
If the grinding of the teeth is repeated often for several months, then a doctor’s consultation is necessary. Otherwise, bruxism can lead to the following consequences:
-
thinning of tooth enamel and increased sensitivity of teeth;
-
problems with fillings, they will crumble and crack;
-
malocclusion;
-
loosening of milk teeth;
-
headaches and decreased concentration;
-
overload of the maxillofacial joint;
-
spasm of the facial muscles.
Excessive tooth wear increases the risk of bruxism during adolescence and adolescence. Also, a strong uncontrolled spasm of the jaws can lead to dislocation of the temporomandibular joint.
What to do if a child grinds his teeth in his sleep
Pay attention to when attacks most often occur – during the day, at night, at home or in a public place. Also record other violations in the child’s behavior and his health complaints. Seek advice from a pediatrician, pediatric dentist. Pass the necessary tests and go through the examinations prescribed by the doctor.
Also record other violations in the child’s behavior and his health complaints. Seek advice from a pediatrician, pediatric dentist. Pass the necessary tests and go through the examinations prescribed by the doctor.
The following tips will also help to cope with bruxism:
-
Adjust the psychological climate at home. Try not to swear with loved ones in front of the child, talk to the baby more often and ask him to talk about his feelings, fears.
-
Do not load your child with various early development circles.
-
Organize the right daily routine with obligatory daytime sleep. The nervous system of the child needs a break during the day, even if he himself looks active and does not want to sleep. Take a relaxing bath 1-2 hours before bed and read a book. Active games should be prohibited.
-
Review your diet. Add solid vegetables to the menu to provide a load on the chewing muscles.
If the baby often catches a cold, suffers from a chronic runny nose or nasal congestion, then you need to check the adenoids. With a syndrome of hyperactivity and emotional excitability of a child, it is recommended to visit a psychologist or neurologist.
With a syndrome of hyperactivity and emotional excitability of a child, it is recommended to visit a psychologist or neurologist.
Treatment and prevention of teeth grinding during sleep
There is no specific treatment for bruxism, since this pathology is not an independent disease. The main task of the doctor is to identify the cause of the pathology. This will depend on the treatment plan. To eliminate the grinding of teeth, drug therapy, physiotherapy, correction of the emotional state and dental methods are used, for example, the installation of protective caps on the teeth.
The main methods of therapy:
-
Normalization of sleep with the help of sedatives.
-
Taking vitamins of group B, preparations with magnesium and calcium.
-
Treatment of adenoids.
-
Psychological correction – art therapy, music therapy, sandbox. Working with parents in the presence of intra-family conflicts.

To relieve muscle tension, you can use coniferous baths, massage and exercises in the pool.
The dentist helps to protect the teeth from abrasion by installing a special protective cap. It is made of soft material, so it does not cause discomfort. It can only be worn at night. The most optimal is the manufacture of caps on an individual cast. But you can also buy ready-made ones. This method is only suitable for students.
Also, in the presence of damage to the enamel and sensitivity, fluoridation and remineralization of the teeth are carried out. If necessary, caries is treated.
An orthodontist can help correct your bite. For this, plates, bracket systems are used. Orthodontic design is selected individually, based on the severity of the problem and the age of the child. Incorrect bite is easy to correct when the jaws have not yet fully formed. Therefore, the sooner you visit a pediatric orthodontist, the better the result will be.
How to prevent bruxism: advice for parents
The main preventive measure is to create a comfortable, calm and trusting atmosphere at home. Even if you think that everything is fine in your family, the child may think otherwise.
Try to help your child deal with emotions. Communication with animals, drawing a problem, using toys as interlocutors helps well.
Do not ignore preventive examinations from specialists. Treat caries promptly. Try to enrich the child’s diet with vitamins, do not chop food. Walk outdoors daily.
A single grinding of the teeth is not a cause for concern. But, if bouts of bruxism are becoming more frequent, then consult a doctor to identify the cause.
Call now
+7 (495) 215-58-10
Make an appointment
Why do newborns spit up? | Philips Avent
search support icon
Search Keywords
Home ›› Why is my baby spitting up and how can I help him?
Home ›› Why does my baby spit up and how can I help him?
↑ Top
Whether it’s your first or third baby, you’re bound to have questions about feeding. Reflux (spitting up) is a common topic among frequently discussed feeding topics, so you are not alone in finding the answer to the question “Why does my baby spit up so often?”.
Reflux (spitting up) is a common topic among frequently discussed feeding topics, so you are not alone in finding the answer to the question “Why does my baby spit up so often?”.
So why do babies spit up? And is spitting up normal for babies? You have probably thought about this many times. After reading this article, you will receive important information that will explain the causes of infant spitting up, and you will learn how to act to help the child.
If you have any questions or your child has other symptoms, please contact your doctor.
Why do babies spit up and when is it normal?
Let’s look at why babies spit up and answer the frequently asked question “Why does my baby spit up so much?”. Many newborns spit up after feedings or when burping because their digestive tract is not yet fully developed. However, in some situations, the likelihood of regurgitation in infants increases.
So what causes reflux in babies? The following are some of the main causes of regurgitation in infants:

So is regurgitation normal in infants? In simple words: spitting up after some feeds, or even after each, is absolutely normal for a growing baby. However, there are points that need to be noted in order to distinguish ordinary regurgitation from vomiting. The two processes are very different, so you should check with your doctor if your baby is vomiting heavily after every or most feeds.
Also seek medical attention if your child has any of the following symptoms that a doctor can help identify: 2
- The child spit up frequently, does not gain enough height or weight.
- Appears to be in pain, cries a lot, or arches his back.
- Coughing or difficulty breathing, which may be a symptom of gastroesophageal reflux disease.
- Spitting up even if he hasn’t eaten anything.
- There is intense vomiting.
- Fever or diarrhea, which may be a sign of an intestinal infection and lead to dehydration.
If your baby spit up a small amount of milk after a feed and continues to grow and stay healthy, rest assured that this is normal and nothing to worry about. If you have any questions about reflux in infants, check out this article to learn about the symptoms of reflux and how to deal with it!
What to do
Now that you know that spitting up is a normal physiological process and what causes it, you are probably wondering what you can do to help your baby. After you have consulted with your pediatrician and he has determined that spitting up is not a cause for concern, there are a few things you can do to help you when you are not sure: 1
1. Regular belching of air.
In addition to burping after feedings, try helping your baby burp when changing breasts. And when feeding from a bottle, try to have the child spit up air every 30-60 ml of the mixture. Consider using an anti-colic bottle with an AirFree valve. The AirFree valve prevents air from entering the nipple even when the bottle is in a horizontal position and the nipple remains completely filled with milk. The use of such a bottle will allow your baby to drink in an upright position, which will reduce the frequency of reflux, improve the digestion process and make the feeding process more comfortable for both you and the baby. Find out more about Philips Avent anti-colic bottles with AirFree valve here.
And when feeding from a bottle, try to have the child spit up air every 30-60 ml of the mixture. Consider using an anti-colic bottle with an AirFree valve. The AirFree valve prevents air from entering the nipple even when the bottle is in a horizontal position and the nipple remains completely filled with milk. The use of such a bottle will allow your baby to drink in an upright position, which will reduce the frequency of reflux, improve the digestion process and make the feeding process more comfortable for both you and the baby. Find out more about Philips Avent anti-colic bottles with AirFree valve here.
3. Avoid vigorous movement after feeding.
To avoid spitting up after a feed, it is best to refrain from any bouncing, rocking or active play until the milk has been digested better.
4. Keep your baby’s head up while feeding.
When you’re trying to find the right feeding position that’s comfortable for both your baby and you, try to avoid a position where your baby’s head is down. In other words, it is necessary to ensure that in the process of feeding the head of the child is above the level of his legs.
In other words, it is necessary to ensure that in the process of feeding the head of the child is above the level of his legs.
5. Raise the mattress at the head of the bed
It is a good idea to roll up some towels or blankets and put them under the mattress (but not on top of the mattress) in the crib. Make sure that only the headboard is raised and that there are no creases in the middle of the mattress. There should be a very slight slope from which the baby will not slip.
It’s a natural process
If you ever ask yourself the question “Why does my baby spit up?” just remember that spitting up is a completely natural, sometimes troublesome process that is part of parenthood. There are various reasons for spitting up in babies, but if your baby looks calm after a feed and is actively developing, you have nothing to worry about. In truth, spitting up is more of a problem for the parents than for the child himself, who may not even notice it.
Articles & tips from Philips Avent
New Anti-colic bottle with AirFree valve
Designed to reduce colic, gas and spitting up 1
9007 If you see or feel any other symptoms that the baby is not getting enough milk, do not postpone the visit to the doctor. If the doctor confirms that the baby’s spitting up is normal, all you have to do is keep a clean bib ready!
Baby+ app
Download the app and track your child’s development and growth with trackers, and keep those special moments forever.
Download App:
1 kidshealth.org – Breastfeeding FAQs: Some Common Concerns Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
I understand
You are about to visit a Philips global content page
You are about to visit the Philips USA website.
Delayed speech development: how to help your child speak
№8 (185) September, 2018
Continued. Beginning at #6(183).
“Dysarthria”: diagnostics and methods of speech therapy correction
The fourth lesson is taught by a clinical speech pathologist of the highest category, rehabilitation specialist of the Center for Pediatric Neurology and Medical Rehabilitation Tatyana Kalabukhova.
Good speech is the most important condition for the comprehensive development of children. The richer and more correct the child’s speech, the easier it is for him to express his thoughts, the wider his possibilities in cognizing the surrounding reality. A child with a well-developed speech easily enters into communication with others, he can clearly express his thoughts, desires, ask questions, and agree with peers on a joint game. Conversely, a child’s slurred speech complicates his relationships with people and often leaves an imprint on his character.
Dysarthria is a speech disorder in which the movements of the articulatory apparatus are disturbed, that is, the mobility of the speech organs (lips, soft palate, tongue) is limited, and as a result, sound pronunciation is impaired, speech becomes less intelligible, blurred and not clear. Children with dysarthria find it difficult not only to pronounce sounds, but also to chew and swallow. The voice of dysarthric children is quiet, weak, and sometimes harsh, with hoarseness. The rhythm of breathing is disturbed, speech loses its smoothness.
Depending on the area of brain damage, various manifestations of dysarthria are possible: from severe forms with swallowing problems. salivation, paresis of the muscles of the larynx, to light “erased” forms, in which slurred speech with a nasal tinge is noted. There is even a “cold” form of dysarthria, which occurs only in a cold room or in winter.
Yes logopedic classification based on the intelligibility of the child’s speech to others. There are 4 degrees of severity of speech impairment. From mild (I), which can only be detected with a special examination, for others this violation may look like a fuzzy diction.
There are 4 degrees of severity of speech impairment. From mild (I), which can only be detected with a special examination, for others this violation may look like a fuzzy diction.
Up to severe (IV) degree, when the child’s speech is incomprehensible even to parents or is completely absent.
Since dysarthria is a neurological diagnosis, a speech therapist deals with the correction of impaired speech functions, and medication is prescribed by a neurologist. Speech therapy work with children with dysarthria should be started at an early age, since timely speech therapy help in 75% of cases helps to avoid many problems in the further development of the baby. Dysarthria in infancy may present as:
- – difficulty sucking breasts, bottles, nipples;
- – violation of swallowing in the process of drinking, eating, swallowing saliva, the child chokes, often burps;
- – disorders of chewing and biting at an older age.

At the Center for Child Neurology and Medical Rehabilitation, I, as a clinical speech therapist, conduct speech therapy massage courses to stimulate sucking, swallowing, and later chewing in children from 1 month old, including children on tube feeding. Under the supervision of a specialist, mothers are taught the elements of a special massage to stimulate sucking and swallowing (massage should be done before each feeding). It explains the need for the mother to keep a “Feeding Diary” of the baby (taking into account regurgitation and supplementary feeding through a tube). Our main task is to remove the child from tube feeding and normalize his nutrition.
The restoration of the sucking reflex is slow, it can be stimulated by special speech therapy massage and point stimulation at home:
*Face muscle massage
9000 evenly on both sides.
1. From the middle of the forehead to the temples.
2. From the middle of the forehead to the ears.
3.From the middle of the forehead to the auricles and then through the cheeks to the chin.
4. From the eyebrows to the scalp.
5. From the back of the nose to the auricles.
6. From the earlobes along the cheeks to the wings of the nose.
* Tongue massage
It is convenient to massage the tongue with a nipple placed on a spatula or a finger in a fingertip.
1. Stroking the tongue from its middle to the tip. Gradually move closer to the root of the tongue.
2. Stroking from the middle line of the tongue to the sides.
3.Pat over the entire surface of the tongue and along the edge of the tongue from top to bottom.
* Massage of the lips and circular muscles of the mouth
The child’s lips are massaged with the index or middle fingers of both hands.
1. Stroke above the upper lip and under the lower lip from the middle to the edges.
2. Kneading the lip between the thumb and forefinger, “rubbing” the lip. Massage is performed with the upper and lower lips.
3. The fingers are placed in the corners of the mouth, the lips are stretched into a smile, and then gathered into a “tube”.
At about 5 months old, babies begin to put things in their mouths, which allows them to learn the movements of their jaws, tongue and lips. If for some reason this does not happen, you can teach your child to bite and chew, or seek help from a specialist.
Since biting and chewing are important steps in teaching a child to feed themselves, I recommend starting with special devices designed to stimulate and exercise the lips, cheeks, tongue and gums. These can be teethers, vibrating sticks, syringes and other tools. They can be found on speech therapy sites, in pharmacies.
The process of learning to bite and chew is long, so you need to follow the sequence of work:
Stage 1 – Show the child how to bite so that the baby understands what this word means. This stage can be turned into an exciting game if you take turns feeding the doll. Let the child feed you too. Use any sound or word at the same time (“bite”, “am-am”).
This stage can be turned into an exciting game if you take turns feeding the doll. Let the child feed you too. Use any sound or word at the same time (“bite”, “am-am”).
Stage 2 – Aimed at the formation of the correct opening of the mouth when chewing. Place the teether between the chewing surfaces of the teeth and help the gums close and open. When doing this, use the word “bite”. Do this in front of a mirror so that the baby can see how he bites (if this is not too distracting for him).
Stage 3 – After the child understands the word “bite” and learns how to do it, start chewing. Do up to 20-25 chewing movements on each side (in difficult cases, help with your hand, holding your chin and repeating lowering and raising the lower jaw in time with chewing).
Stage 4 – Use long teethers to develop bilateral chewing and increase jaw strength. Change sides to stimulate movement of chewing activity: 3-5 on one side, then on the other. Start with the side teeth, gradually moving to the back teeth.
Start with the side teeth, gradually moving to the back teeth.
Stage 5 – When the child has learned to bite and chew, dip the teether in puree while working – this will transfer the new skill to real food.
And praise, praise, praise the baby!
To overcome hypersalivation (profuse salivation) in children with dysarthria, it is necessary to teach the child with closed lips to suck, swallow saliva with the head thrown back and in the usual position. Salivation can be both constant and intensify under certain conditions. Even mild drooling, such as moistening of the corners of the mouth during speech, a small amount of saliva leakage can indicate dysarthria. Before performing any articulation exercise, the speech therapist reminds the child to swallow saliva, blot inside the mouth with a napkin.
The main stages of speech therapy correction for hypersalivation:
1. Cryotherapy of active points in the lips.
2. Mouthwash with medicinal herbs, mineral water, jelly and kefir.
3. Speech therapy massage and acupressure massage.
4. Chewing solid food.
5. Static and dynamic mimic and articulation exercises.
6. Breathing exercises and pronunciation of vowels on a hard attack.
Speech therapist advice for parents with hypersalivation in children:
- – Bystanders should constantly monitor the position of the child’s mouth and remind him to keep his mouth closed when he is not eating or talking.
- – It is important that the child develops a differentiated sensation of dry and wet chin.
- – In the classroom, it is necessary to pause at certain intervals and invite the child to swallow saliva.
Based on my practical experience, with systematic work, salivation is reduced and the child has better control over swallowing.
In most cases, dysarthric children have some behavioral features. For example, babies do not like to lace up their shoes or fasten buttons on their own. This is due to poorly developed fine motor skills. Such children cannot properly hold a pen or pencil in their hands, control the force of pressure, use scissors. Therefore, most dysarthria have poor handwriting. It is difficult for children to exercise and dance. Musical hearing impaired. Children cannot accurately perform different motor exercises, they are clumsy.
For example, babies do not like to lace up their shoes or fasten buttons on their own. This is due to poorly developed fine motor skills. Such children cannot properly hold a pen or pencil in their hands, control the force of pressure, use scissors. Therefore, most dysarthria have poor handwriting. It is difficult for children to exercise and dance. Musical hearing impaired. Children cannot accurately perform different motor exercises, they are clumsy.
Treatment of dysarthria in children requires an integrated approach that combines drug therapy, speech therapy correction and rehabilitation .
Drug treatment of dysarthria in children
The treatment is based on the treatment of the underlying neurological disease, as well as the use of nootropic drugs. They improve mental activity, memory, stimulate cognitive functions.
Speech therapy and rehabilitation
Speech therapy includes special sessions for children. The speech therapist draws up an individual speech chart, which contains the results of the diagnosis and a detailed plan for correcting the defect with a description of the exercises:
The speech therapist draws up an individual speech chart, which contains the results of the diagnosis and a detailed plan for correcting the defect with a description of the exercises:
- – for the development of fine motor skills – finger games, gymnastics;
- – for the development of articulatory motor skills – articulatory gymnastics, speech therapy massage;
- – for speech and physiological breathing – breathing exercises;
- – to correct the broken and consolidate the correct pronunciation ;
- – for the formation of the expressiveness of speech and speech communication .
Section 8 diseases of the oral mucosa
001. A 2-year-old child fell ill acutely. Temperature rise up to 38°С. Sleep badly. Refused to eat. Mom noticed that when tying a scarf and touching the submandibular region, the child cries. Objectively: the state of moderate severity, the child is tearful, lethargic. On the skin of the face in the oral region, a group of bubbles is determined. Significantly enlarged, dense, painful lymph nodes are palpated in the submandibular region on both sides (with which the child was sent to the surgical room). The skin over the lymph nodes is somewhat hyperemic, going into a fold. Fluctuation is not defined. Estimated diagnosis
On the skin of the face in the oral region, a group of bubbles is determined. Significantly enlarged, dense, painful lymph nodes are palpated in the submandibular region on both sides (with which the child was sent to the surgical room). The skin over the lymph nodes is somewhat hyperemic, going into a fold. Fluctuation is not defined. Estimated diagnosis
a) acute serous odontogenic lymphadenitis
b) acute serous dentogenic lymphadenitis
c) abscessing lymphadenitis
g) adenoflegmon of the submarine 9000 9008. Temperature rise up to 38°С. Sleep badly. Refused to eat. Mom noticed that when tying a scarf and touching the submandibular region, the child cries. Objectively: the state of moderate severity, the child is tearful, lethargic. On the skin of the face in the oral region, a group of bubbles is determined. Significantly enlarged, dense, painful lymph nodes are palpated in the submandibular region on both sides (with which the child was sent to the surgical room). The skin over the lymph nodes is somewhat hyperemic, going into a fold. Fluctuation is not defined. Likely to confirm presumptive diagnosis
The skin over the lymph nodes is somewhat hyperemic, going into a fold. Fluctuation is not defined. Likely to confirm presumptive diagnosis
A) Determination of the KPU index
b) Study of the state of the mucous membrane of the oral cavity
c) Purification of the lymph node
g) Clinical blood test
d) X -ray
9000 9000 003. 2 years old. acutely. Temperature rise up to 38°С. Sleep badly. Refused to eat. Mom noticed that when tying a scarf and touching the submandibular region, the child cries. Objectively: the state of moderate severity, the child is tearful, lethargic. On the skin of the face in the oral region, a group of bubbles is determined. Significantly enlarged, dense, painful lymph nodes are palpated in the submandibular region on both sides (with which the child was sent to the surgical room). The skin over the lymph nodes is somewhat hyperemic, going into a fold. Fluctuation is not defined. The most appropriate method of treatment in this case
Fluctuation is not defined. The most appropriate method of treatment in this case
A) UHF-therapy
b) ointment dressings
c) Sanning of the oral cavity
g) Treatment of the main disease + ointment dressings
d) oral sanitation
004. A 1.5-year-old child who had an acute respiratory infection two weeks ago had a fever of 39°C on the second day and vomiting. The child refuses food, is naughty. The pediatrician was diagnosed with ARI. At the time of the present examination: lymphadenitis of the submandibular lymph nodes, profuse salivation, on the sharply hyperemic mucous membrane of both lips, the tip of the tongue and cheeks – small multiple erosions with clear outlines, covered with fibrous plaque. The gum is swollen, bleeding. Specify the main symptoms indicating the diagnosis of acute herpetic stomatitis
a) clinical picture of an acute infectious disease
b) lymphadenitis
c) gingivitis
g) rashes in the oral cavity
d) all the above symptoms
005. in a child is one year old. who suffered from acute respiratory infections two weeks ago, the second day the body temperature was raised to 39 ° C, vomiting. The child refuses food, is naughty. The pediatrician was diagnosed with ARI. At the time of the present examination: lymphadenitis of the submandibular lymph nodes, profuse salivation, on the sharply hyperemic mucous membrane of both lips, the tip of the tongue and cheeks – small multiple erosions with clear outlines, covered with fibrous plaque. The gum is swollen, bleeding. The leading role in the pathogenesis of this disease was played by
in a child is one year old. who suffered from acute respiratory infections two weeks ago, the second day the body temperature was raised to 39 ° C, vomiting. The child refuses food, is naughty. The pediatrician was diagnosed with ARI. At the time of the present examination: lymphadenitis of the submandibular lymph nodes, profuse salivation, on the sharply hyperemic mucous membrane of both lips, the tip of the tongue and cheeks – small multiple erosions with clear outlines, covered with fibrous plaque. The gum is swollen, bleeding. The leading role in the pathogenesis of this disease was played by
A) Contact with a sick child
b) a decrease in immunity level
c) hypothermia
g) recently transferred ARS
d) all of the above
006. in a child of a year and a half of a year and a child, transferred. two weeks ago acute respiratory infections, the second day the body temperature was raised to 39°C, vomiting. The child refuses food, is naughty. The pediatrician was diagnosed with ARI. At the time of the present examination: lymphadenitis of the submandibular lymph nodes, profuse salivation, on the sharply hyperemic mucous membrane of both lips, the tip of the tongue and cheeks – small multiple erosions with clear outlines, covered with fibrous plaque. The gum is swollen, bleeding. The main treatment for this child can be prescribed
The child refuses food, is naughty. The pediatrician was diagnosed with ARI. At the time of the present examination: lymphadenitis of the submandibular lymph nodes, profuse salivation, on the sharply hyperemic mucous membrane of both lips, the tip of the tongue and cheeks – small multiple erosions with clear outlines, covered with fibrous plaque. The gum is swollen, bleeding. The main treatment for this child can be prescribed
A) antiviral
b) antipyretic
c) anesthetic
g) antiseptic
d) stimulating immunity
007. acute herpetic stomatitis – this is
rye. b) diseases of the oral mucosa
c) changes in the oral mucosa
d) acute respiratory disease
e) recurrent disease of the oral mucosa
008. A child with acute hepatitis C is not a spreader of the virus lymphadenitis
A child with acute hepatitis C is not a spreader of the virus lymphadenitis
e) in any of the listed periods
009. Children over 3 years old
a) brunettes
c) children who are naturally fed up to 1 year of life
) all named
d) none of the named
010. The reason for acute herpetic stomatitis is
A) Herpes virus
9,0003
9EL viral-microbial associations of the oral cavity
c) microflora of the oral cavity, acquiring pathogenic properties with a decrease in the reactivity of the body
d) viral Mich. infection
infection
e) not named
011. In acute herpetic stomatitis,
A) crust
b) blister
c) Bubble
) PUENCE
012. The occurrence of
. ) hypothermia
b) taking immunosuppressants
c) emotional and hormonal changes
d) any past illness
e) each of the listed
013. For early diagnosis and initiation of preventive measures in relation to stomatitis, such signs of ACS as
a) herpetic eruptions on the skin of the face, hands
b) rise in temperature, deterioration in general well-being, refusal to eat, salivation
c) catarrhal gingivitis and lymphadenitis
d) catarrhal gingivitis, lymphadenitis, herpetic eruptions on the skin
e) don’t know
014. The determination of the period of development of acute herpetic stomatitis is based on
The determination of the period of development of acute herpetic stomatitis is based on
a) the state of the lymph nodes
b) the nature of the elements of the lesion of the oral mucosa against the background of concomitant symptoms of the disease
c) the state of the gums
d) the presence of symptoms of general intoxication of the body
e) I don’t know
015. OGS clinic is typical
a) elevated body temperature
b) lymphadenitis
c) the presence of erosion in the oral cavity
g) the presence of gingivitis
d) all of the listed
016. For a slight form of OGS
A) lymphadenitis
b) increased body temperature
Gingivitis
d) erosions on the oral mucosa
e) all of the above symptoms0003
c) gingivitis
g) erosion on the mucous membrane of the cavity of the RTU
d) all of the listed symptoms
018. For the moderate form OGS are characteristic ) gingivitis
For the moderate form OGS are characteristic ) gingivitis
d) erosion on the oral mucosa
e) all of the above symptoms
019.0003
A) gingivitis
b) fever up to 39-40 ° C
c) submandibular nodes
g) rashes in the oral cavity
d) named
020. The first clinical clinical signs of acute herpetic stomatitis (AHS) of moderate severity in children are
a) an increase in body temperature
b) a violation of the behavior of the baby: lethargy, drowsiness or increased excitability, crying, restless sleep, etc. .
c) dyspeptic symptoms: refusal to eat, vomiting, loose stools
d) lymphadenitis of the submandibular, submental, cervical nodes, gingivitis
e) blisters on the skin, single and multiple aphthae on the oral mucosa
2172. The duration of the period of rashes in moderately severe acute hepatitis C
The duration of the period of rashes in moderately severe acute hepatitis C
a) less than one day
b) no more than 29 hours
c) one or two days
d) two or three days
e) at least a week
022. The role of the endogenous microbial flora of the oral cavity in acute hepatitis C is as follows
contributes to the transition from acute catarrhal gingivitis to chronic and subacute
e) causes a long course of the disease and pyogenic complications
023. The essence of antiviral therapy for acute hepatitis C in the period of rashes
a) promote the fastest epithelialization of lesions
b) help reduce the body’s temperature response
c) stimulate nonspecific reactivity of the child’s body
d) prevent the recurrence of lesions 9006
e) promote detoxification of the body°С), shown
a) antibiotics
b) sulfonamides
c) 2% solution of sodium salicylate
d) enema with analgin (1 ml of 50% solution in 25 ml of water)
e) interferon 9006
025. For local treatment of acute hepatitis C in the first 3 days,
For local treatment of acute hepatitis C in the first 3 days,
a) antiviral drugs
b) keratoplastic agents
c) antiseptics
d) antiviral ointments and painkillers
d) All substances listed above
026. For the local treatment of OGS in the catarrhal period, the most shown
A) Antiviral drugs
b) Keratoplastic agents
B) Antiseptic substances
G) and painkillers
e) all of the above substances
027.0003
A) antiviral agents
b) antiseptics
c) Keratoplastic agents
g) Proteolytic agents
d) None of the
028. It is more advisable to prescribe to the child with the OGS 9) during the period of rashes
It is more advisable to prescribe to the child with the OGS 9) during the period of rashes
b) at the time of onset of lymphadenitis
c) during the prodromal period
d) during the onset of gingivitis
e) during all indicated periods
029. More effective in the phase of non -specific inflammation during the treatment of OGS and RGS
a) a solution of chlorin
b) a hydrogen peroxide solution
c) Kalanchoe juice
g) calendar
9000 3 furacillin
030.
have an antiviral effect a) bonafton 0.5% ointment
b) flucinar
c) nonmycin ointment
3 g)0003
d) NISTAIN ointment
031. The least effective antiviral ointment used locally for the treatment of herpetic lesions of SOPR, is
The least effective antiviral ointment used locally for the treatment of herpetic lesions of SOPR, is
A) Bonafton ointment 0.5%
b) ointment of florenal 0.5%
c) tiber -tirep
d) rhyodoxol ointment 0.5%
e) oxolinic ointment 0.25%
0320003
b) alpizarine ointment 2%
c) Gossipol line 3%
g) Megosin ointment 3%
d) any of the above
033. The most shown the following methods mouth –
a) irrigation of the oral cavity with antiseptics
b) antiseptic hygienic treatment of teeth
c) oxygen therapy
d) all the methods listed above
e) None of the methods listed above
034. Patients with ACS should preferably be admitted
Patients with ACS should preferably be admitted
d) none of the listed
e) any of the listed
035. Leading in anti-epidemic measures in case of an outbreak of ACS in kindergarten is
a) disinfection of the premises
b) isolation and treatment of sick children
c) Establishment of the source of infection
g) The disposal of public objects
d) Determining the transmission of infection
036. The priority anti -epidemic measures for the OGS and RSS are 9000 9079
a) individual oral hygiene, individual utensils
b) daily examinations of children to diagnose and isolate patients
c) all of the above
d) disinfection of premises and common areas
e) carrying out preventive measures for all contacted children without clinical symptoms using antiviral ointments (3-4 times a day)
037. Dentists at admission
Dentists at admission
a) specific disinfection of working instruments
b) the presence of a gauze bandage on the face during the reception
c) quartzization of the office
d) all of the above
e) none of them
038. with diseases of the oral mucosa
b) in the management of the admission of patients with acute hepatitis C in the general medical office
c) in the establishment of certain hours of admission for the first time applied and re-called children
d) in the clinical examination of children with recurrent herpes infection in the oral cavity
e) in the use of masks by a doctor and medical staff
039. Chronic herpes infection (development of CHD) contributes to
a) ACS disease at certain times of the year
b) child’s age
c) child’s gender
d) child’s immune system
e) oral mucosal injury
040. To confirm the diagnosis of CHD, it is necessary to conduct a number of studies. The most appropriate way to clarify the diagnosis is
To confirm the diagnosis of CHD, it is necessary to conduct a number of studies. The most appropriate way to clarify the diagnosis is
a) examination of the contents of the vesicles for microflora
b) examination of smears-imprints for the presence of symplasts, giant cells (cytological method)
c) direct electron microscopy method for the study of smears-imprints with erosion bubbles
d) bacteriological method
e) clinical trial
041. RGS is characterized by
a) uneven edges of erosion, absence of infiltrate at the base, recurrent character
edges, single element
d) none of the named
e) ulcer
042. The main thing in the local treatment of chronic recurrent herpetic stomatitis is
a) use of drugs that stimulate local immunity
b) long-term local treatment with antiviral drugs
c) use of keratoplastic agents
d) use of painkillers
e) none of the above
9072 The most important in the treatment of chronic recurrent herpetic stomatitis in children is
a) the use of antiviral agents
b) the use of anti-inflammatory, analgesic and keratoplastic drugs
c) detection and elimination of an infectious-allergic focus in the body
d) a course of treatment with antiviral drugs in combination with an increase in the level of the immune system
e) I don’t know
9 044. Specify the scheme of anti-relapse therapy for recurrent herpetic stomatitis (with permanent course of the disease)
Specify the scheme of anti-relapse therapy for recurrent herpetic stomatitis (with permanent course of the disease)
a) bonafton 1 table. 3 times a day for 10 days. Immunoglobulin antiherpetic 1.5 ml every other day / m. Course 6 injections.
b) antistaphylococcal gamma globulin 3 ml IM every 3-4 days. Course 6 injections. Askorutin 1 tab. 3 times a day. Prednisolone – 20 mg.
c) Aevit 1 capsule 2-3 times a day
d) Deoxyribonuclease – 25 mg IM
e) Any of the listed
045. Which of the listed systemic drugs are indicated for patients with recurrent herpes (mild severity, frequency of relapses 1-2 times a year)?
A) Levamisole
b) Fenkarol
c) Nucleinate sodium
g) Nystatin
d) prenisalon
048. Indicate the systems of systemic administration, which are shown to the patients with the recurrent degrees
Indicate the systems of systemic administration, which are shown to the patients with the recurrent degrees
a) Phencarol
b) Decaris
c) Anti-measles gamma globulin
d) Anti-herpetic vaccine
e) Vitamin therapy (C)
049. Recurrent herpetic stomatitis differentiate
A) with a shingle lichen
b) with acute herpetic stomatitis
c) with recurrent Afts of the oral cavity
) one of the named
050. The causative agent of herpangina is
a) herpes simplex virus
b) ECHO and Coxsackie virus
c) Candida
g) hemolytic streptococcus a
d) None of the listed
051. Pathogenetic treatment of herpangin is
Pathogenetic treatment of herpangin is
a) Lapivirus, keratoplastic
B) Antiviral treatment
9) don’t know
e) none of the named
052. The differential diagnostic sign between ACS and herpangina is
a) with herpangina there are no catarrhal gingivitis phenomena
B) Duration of the disease
c) the nature of the elements of the lesion
g) Localization of the elements of the lesion
d) None of the
053. Supporting lichen must differentiate
) with red flat lichen 9000
b) with pemphigus
c) with primary syphilis
d) with acute herpetic stomatitis
e) none of them
054. 0003
0003
a) diffuse localization, on the mucous membrane of the oral cavity
b) localization on the skin
c) localization along the neurovascular bundles
d) localization on the skin of the chest
e) none of the above localizations
055. The form of severity in recurrent herpetic stomatitis is determined
a) based on clinical data
b) depending on the number of relapses
c) on the level of rise in body temperature
d) on the localization of rashes
e) on the duration of the recurrence
056. In herpes zoster, the following elements of lesions of the oral mucosa occur
a) 907 b) 2 erythema
c) vesicle
d) abscess
e) erosion with scalloped outlines
057. 0003
0003
a) in the use of antiviral drugs
b) in good oral hygiene
c) in the use of keratoplastic agents
d) in the use of anesthetics
e) don’t know Treatment
stomatitis in chickenpox consists
a) in the use of antiviral drugs throughout the illness
b) in antiseptic treatment of the oral cavity, anesthesia
c) in the use of antiviral drugs at the beginning of the disease, anti-inflammatory drugs in the period of development of the disease, keratoplastic drugs in the period of extinction
d) in the appointment of anti-inflammatory drugs
e) I don’t know
059. Most typical for the first year life of a child
a) acute gingivitis
b) chronic gingivitis
c) cheilitis
d) exudative erythema multiforme
e) none of the listed diseases
060. For the age of 2, the most typical is
For the age of 2, the most typical is
A) Candidiasis
b) OGS
B) AFTA Bernara
g) HIELIT
d-shaped gingivitis
9000 9079 061. Most common at the age of 4 years
a) Bernard’s aphthae
b) OGS
c) exudative erythema multiforme
d) symptom of recurrent aphthae
e) all of these diseases
062. The most typical for the school age
A) OGS
b) Hileit
c) U-shaped atropical gingivitis
g) AFTA Bernara
d) None of the listed diseases
063. Typical for school age
a) OGS
b) Bernard’s aphtha
c) Erythema multiforme exudative
d) Gingivitis
9072
064. Hemorrhages in the mucous membrane of the mouth are possible
Hemorrhages in the mucous membrane of the mouth are possible
A) with impaired renal function
b) with diatheses
c) for thrombocytopenia of different origin
g) with hypoplastic (melting) anemia
d) neutropenia
065. What is more important to use as a basis for the classification of diseases of the oral mucosa for making a diagnosis of the disease?
a) the nature of the elements of the lesion and the severity of the clinical development of the disease
b) localization of pathological changes
c) causes of pathology
d) course, type and localization of pathological changes, etiological factors
e) I don’t know
066. violation of the integrity of the oral mucosa, accompanied by dysfunction?
a) disease
b) damage to the oral mucosa
c) changes in the oral mucosa
d) I don’t know
e) any of the above
067. Which concept characterizes a pathological condition in which a violation of the body’s vital functions develops under the influence of extreme stimuli of the external and internal environment, decrease in adaptability with simultaneous mobilization of the body’s defenses?
Which concept characterizes a pathological condition in which a violation of the body’s vital functions develops under the influence of extreme stimuli of the external and internal environment, decrease in adaptability with simultaneous mobilization of the body’s defenses?
a) disease
b) injury
c) Change
g) I don’t know
d)
068. Manifestations in the oral cavity have
A) Kori
b) chickenpox
c) flu
g) any of the named
e) none of the named
069. Manifestations in the oral cavity in a child have
a) X-histiocytosis
b) neutropenia
c) any of the named 9025
070. Manifestations in the oral cavity in a child have
Manifestations in the oral cavity in a child have
071. Erythema multiforme exudative is
a) disease
b) damage to the oral mucosa
c) change in the oral mucosa
d) any of the above
e) none of the above
072. Crimson tongue symptom refers
a) to a disease of the oral mucosa
b) to damage to the oral mucosa
c) to a change in the mucous membrane
6
) to any of the named
e) to none of the named
073. What concept characterizes a pathological condition in which diseases of the body appear as separate symptoms on the mucous membrane of the oral cavity?
a) disease of the oral mucosa
b) damage to the oral mucosa
c) change in the oral mucosa
d) any of the above
e) none of the above
07
The symptom of “Hunter’s” tongue refers
a) to a disease of the oral mucosa
b) to damage to the oral mucosa
c) to a change in the oral mucosa
d) to any of the named
e) to none of the named
075. Necrosis of the oral mucosa is observed
Necrosis of the oral mucosa is observed
) in diseases of the blood and hematopoietic organs
d) in diseases of the respiratory system
e) in chronic diseases of the stomach and other parts of the digestive tract
076.0003
a) a bad habit of biting the mucous membrane of the mouth and cheeks
b) the presence of recurrent herpetic lesions of the lips and facial skin in family members
c) fillings from different metals (halodent, silver and copper amalgam), orthodontic crowns
d ) chronic diseases of the upper respiratory tract, gastrointestinal tract, etc.
e) hereditary factors affecting the characteristics of the body’s reactivity
077. At what rate of recurrence of aphthae in the oral cavity can a severe form of the disease be called?
a) monthly
b) once every few years
c) once a quarter
d) once a year
e) any of the above
characterizes
a) bubble
b) blister
c) Rubts
g) Erosion
d) spot
079. At what changes of the language do children sometimes complain of pain in some types of food?
At what changes of the language do children sometimes complain of pain in some types of food?
A) folded tongue
b) the lined tongue
c) “hairy” language
g) “geographical” language
d) the combination of the folded and “geographical” language
080. children are
a) violation of nasal breathing
b) weakening of the tone of the mimic muscles of the mouth
c) violation of the control of the circular muscle of the mouth
d) none of the above
d) all named
081. The leading in the treatment of heilites in children is
e) all of the above
082. Red border, corners of the mouth and adjacent skin are affected0003
c) with an atopic (eczematous) heilite
g) with a Gradulard Heilite
d) with a facial derivative of Manganotti
083. The main in the treatment of chronic province cracks (stops) is
The main in the treatment of chronic province cracks (stops) is
903 903 9000 3
b) antimicrobial treatment
c) antimicotic treatment
g) orthodontic treatment
d) myotherapy
084. Signs of strepto-staphylococcal lesions (pyoderma) of the Red Kayma of the GUB, the face and mucous membrane of the mouth are
a) fever precedes rashes
b) body temperature rises with significant spread of rashes
c) hemorrhagic crusts on lips deep ulcers with necrotic bottom, dense edges
e) thick, yellow (“honey”) crusts, pustular rashes on the skin and red border of the lips
085. The main factor for the occurrence of candidiasis in infants is
a) dysbiosis
b) Disorders’ disorders
B) Chronic or acute injury (nipple-dummy)
gpovitaminosis) e) none of the above
086. Candidomycosis (thrush) of the oral mucosa is prescribed
Candidomycosis (thrush) of the oral mucosa is prescribed
a) antibiotic ointments
b) antiviral ointments
c) clotrimazole (kavisten) – ointment or solution after feeding the child
d) the same agents before feeding the child
e) none of these agents
087. with fungal stomatitis?
a) “Remodent” toothpaste (contains “Remodent” drug)
b) “Berry” toothpaste (contains a mixture of borax with glycerin)
c) “Health” toothpaste (contains St. John’s wort extract)
d) toothpaste “Forest” (contains chlorophyll: ascorbic acid)
e) hygienic toothpowder “Good morning!”
088. Clinical signs characteristic of erythema multiforme are
a) vesicular rashes on the lips and surrounding skin
b) papules on the hands, forearms, face and other parts of the body
c) crusts on the lips and skin
d) erosions of various sizes and shapes on any parts of the oral mucosa against the background of diffuse hyperemia
d) All listed
089. The most characteristic localization of skin lesions with multiform exudative erytemia is the localization of
The most characteristic localization of skin lesions with multiform exudative erytemia is the localization of
A) in the axillary and inguinal region
b) on the back of the hands
c) any areas
d) skin lesions do not occur
e) all of the above
090. Optimal for identifying the source of allergization in exudative erythema multiforme is
A) The acute initial period of the disease
b) the period of rashes on the mucous membrane of the oral cavity
c) the period of remission
g) repeated relapse
d) any of the named
91. Vincent is called
a) a sharp decrease in the body’s resistance due to adverse social factors or serious illnesses
b) the presence of carious teeth, lack of oral hygiene
c) prepubertion and puberty periods of development
g) the presence of fusospyricular symbiosis in the groove of
d) the use of a hard toothbrush for teeth to teeth
092.
A is used by Antis. b) oxygen therapy
c) antiseptic hygienic treatment of teeth
d) all of the above methods
e) none of the above methods
093. In case of ulcerative-necrotic gingivostomatitis, it is advisable
a) removal of only soft plaque on the teeth
b) removal of supragingival and subgingival calculus
c) removal of necrotic areas in the affected area 907 periodontal pockets
e) the use of broad-spectrum antibacterial drugs and agents that increase body resistance, oral hygiene
094. Soft leukoplakia in the oral cavity characterizes
At the age of 6-7 years, milk teeth begin to fall out and are gradually replaced by permanent teeth. By the age of 13, there is a complete change of time units and a permanent bite is formed in the child. Normally, this is a painless process due to the natural physiology of changing teeth.
Normally, this is a painless process due to the natural physiology of changing teeth.
How do teeth change?
The rudiments of future permanent units are located under the root of the milk tooth and are separated from it by a thin bony septum. At 6-7 years old, osteoclasts of the connective tissue surrounding the milk tooth dissolve the mineral component of the septum and destroy it. At the same time, the pulp of the temporary unit is gradually transformed into a granulation connective tissue rich in osteoclasts, which gradually destroy the dentin of the milk tooth. At the same time, the roots of temporary units dissolve and, in fact, only the crown of the milk tooth remains. It is easily removed on its own, with the help of manipulations by the dentist, or it is pushed out by an actively growing molar (permanent) tooth.
Anatomy of Permanent Teeth The permanent units of a child (and adult) have a complex anatomy.
Visually, the tooth consists of three parts – crown, neck, roots.
- Crown – the visible part of the tooth that rises above the gum.
- Neck – part of the tooth at the level of the gums, in the place where the crown passes into the root, and the enamel unit into the cement.
- Root – part of the unit invisible to the eye, located in the alveolar socket. The basis of each unit consists of dentine – hard tissue. In the coronal part, the dentin is covered with enamel, and in the root part, cementum. Inside the dentin is the pulp of the tooth – loose-fibrous soft connective tissue, penetrated by a large number of blood, lymphatic vessels and nerve endings. Passing through the root canal, through the apical opening located on the upper part of the root, they communicate with the main neurovascular bundle, providing nutrition to the tooth, outflow of excess fluid and its innervation.
Normally, by the age of 13, when a permanent bite is formed, a child has 28 permanent teeth. At the age of 17 – 25 years, the third molars (wisdom teeth) erupt and the number of units may increase – 32 teeth.
Terms and order of eruption of permanent teeth
Normally, the eruption of permanent units occurs 3-4 months after the loss of milk teeth. In girls, this process occurs a little earlier and faster than in boys. In both sexes, the first lower molars appear first. Then the sequence of eruption of permanent teeth is approximately the same as for milk teeth and is as follows.
- 6 – 7 years – central incisors.
- 7 – 8 years – lateral incisors.
- 9 – 12 years old – fangs.
- 10 – 12 years – premolars.
- 10 – 12 years – molars.
The eruption of the second molars completes the formation of a permanent bite.
The main differences between milk teeth and permanent teeth
Unlike the 28 permanent teeth, the milk bite suggests the presence of 20 units. However, they have a number of characteristic features.
- Smaller than permanent teeth.
- White with a slightly blue tint (permanent units have a slightly yellowish tint).
- Less developed and slightly short roots compared to permanent teeth.
- Enamel of temporary teeth is poorly formed – thinner.
- Dairy units can wear off (permanent ones can also, but this is considered a pathology).

As the child grows, milk teeth fall out on their own – this is the norm. Permanent occlusion units should not fall out on their own.
How can you tell if your child will soon have molars?
An increase in the size of the jaw is the main sign of a future change of teeth. Visually, it may not be noticeable. But the appearance of three and diastema (gap) between milk teeth indicates that the child’s jaw is growing and preparing for the formation of a permanent bite.
The following signs are purely individual – they may or may not be present in the child.
- Increased salivation.
- Redness, swelling of the gums and oral mucosa.
- Sore gums.
- Unpleasant itching of the gums.
- Increased body temperature.
- Unreasonable cough, runny nose.
- Disorder of the stool.
- General malaise, lethargy.
- Loss of appetite.
- Sleep disturbance or, conversely, drowsiness.
- Anxiety, irritation, whims.

Important! During the period of eruption of permanent teeth, parents should monitor the condition of the child, the oral cavity and gums. If symptoms that cause concern appear, you should immediately contact a pediatrician and a pediatric dentist.
Possible problems
Despite the fact that the change of teeth is a natural physiological process, some children and their parents may encounter a number of problems that need to be addressed to a pediatric dentist.
No molars
The absence of permanent units can be caused by congenital adentia – the complete or partial absence of tooth buds.
Another reason for the absence of molars is previously transferred inflammatory diseases – periostitis or periodontitis, resulting from progressive caries. Inflammatory diseases of the periosteum and periodontal tissues have an extremely negative effect on the condition of the rudiments of the teeth and can lead to their death.
Inflammatory diseases of the periosteum and periodontal tissues have an extremely negative effect on the condition of the rudiments of the teeth and can lead to their death.
Important! It is absolutely necessary to treat milk teeth from caries. Do not assume that with the change of teeth, the problem will go away by itself. The progression of the disease can adversely affect the health of the rudiments of the teeth.
Molar pain
Enamel, newly appeared permanent teeth, is still poorly formed. The low level of its mineralization makes the teeth vulnerable to cariogenic microflora. This can lead to the development of caries and cause pain.
Due to poorly formed enamel, the sensitivity of teeth to external stimuli (cold, hot, sour, sweet) may increase, which is also accompanied by painful sensations.
Important! Normally, permanent teeth do not hurt. If pain occurs, you should contact a pediatric dentist. The specialist will determine the cause of the pain, carry out the necessary treatment, fluoridation or remineralization of tooth enamel.
Molars growing crooked
The incorrect position of permanent teeth can be caused by two reasons – the growth of a permanent unit is ahead of the process of loss of milk teeth or they were removed ahead of time, which led to the incorrect formation of the rudiments of permanent teeth.
In this case, there is only one way out – orthodontic treatment of malocclusion.
Important! Malocclusion must be corrected. The sooner the visit to the dentist, the more successful the treatment will be. The child will be assigned to wear removable or non-removable orthodontic structures that will help align the permanent teeth and bite.
Injuries
Due to their activity and lack of experience, children can accidentally injure a newly appeared permanent tooth. Due to mechanical damage, cracks and chips may appear on it. Damage looks unattractive. Caring for such teeth is complicated, since food residues can fill up in the cracks, which will certainly lead to the development of caries.
 I’m sure a lot of other men would enjoy the same. Some of my guy friends who are now parents had planned something similar (like a gathering or a weekend trip with their friends).”
I’m sure a lot of other men would enjoy the same. Some of my guy friends who are now parents had planned something similar (like a gathering or a weekend trip with their friends).” With the help of TODAY hosts Savannah Guthrie and Natalie Morales, the party included the father, Britt, in the festivities.
With the help of TODAY hosts Savannah Guthrie and Natalie Morales, the party included the father, Britt, in the festivities.  Her favorite pastimes include watching Dr. Phil, practicing her Emmy acceptance speech, and subtly sneaking feminism into her daily conversations.
Her favorite pastimes include watching Dr. Phil, practicing her Emmy acceptance speech, and subtly sneaking feminism into her daily conversations.



 Called “diaper parties” or “dadchelor parties,” these male-centered baby showers involve guests watching sports and bringing diapers rather than anything listed on a baby registry. Another great excuse to have a bash for the boys too!
Called “diaper parties” or “dadchelor parties,” these male-centered baby showers involve guests watching sports and bringing diapers rather than anything listed on a baby registry. Another great excuse to have a bash for the boys too!
 Times have changed though, and many men want to go to baby showers now.
Times have changed though, and many men want to go to baby showers now.
 A father’s perspective was something that was usually lacking at baby showers in the past
A father’s perspective was something that was usually lacking at baby showers in the past
 But don’t worry!
But don’t worry! 


 Shashlik can be anything, you can mix fruits, vegetables, feta cheese, both raw and fried .
Shashlik can be anything, you can mix fruits, vegetables, feta cheese, both raw and fried .  To remember this party for a long time, you can give your friends a small part . Here is a very simple and inexpensive idea:
To remember this party for a long time, you can give your friends a small part . Here is a very simple and inexpensive idea:  Only one thing is missing: birthday list, so you will definitely get targeted gifts that really serve and use immediately.
Only one thing is missing: birthday list, so you will definitely get targeted gifts that really serve and use immediately. 
 It can be an original and practical gift, especially in the first months of pregnancy.
It can be an original and practical gift, especially in the first months of pregnancy.  .. in short, we are sure that theme parties you will find at your party.
.. in short, we are sure that theme parties you will find at your party. 
 You can also order them and make them confectioners: You won’t believe your eyes admiring them in all their perfection.
You can also order them and make them confectioners: You won’t believe your eyes admiring them in all their perfection. 

 The first to finish will receive a special gift.
The first to finish will receive a special gift.  Thoughts for baby shower guests
Thoughts for baby shower guests

 Wait for the ambulance team to stabilize your baby. The only exception is if they have a seizure. In this case, you can carefully roll them over to their side while you wait for the ambulance. If they aren’t breathing, start CPR if you know how.
Wait for the ambulance team to stabilize your baby. The only exception is if they have a seizure. In this case, you can carefully roll them over to their side while you wait for the ambulance. If they aren’t breathing, start CPR if you know how. You should watch for signs of concussion in your baby, including if they:
You should watch for signs of concussion in your baby, including if they: If they have minor injuries or bumps, you can use some home care to soothe them.
If they have minor injuries or bumps, you can use some home care to soothe them.
 Babies are especially at risk of falling as they learn to roll, climb, and walk. No matter how careful you are, you can’t prevent all accidents, so it’s important to know what to do when your baby falls.
Babies are especially at risk of falling as they learn to roll, climb, and walk. No matter how careful you are, you can’t prevent all accidents, so it’s important to know what to do when your baby falls.

 Then watch for changes in any symptoms. They will usually get better on their own over several days, though it can take up to 4 weeks to fully recover.
Then watch for changes in any symptoms. They will usually get better on their own over several days, though it can take up to 4 weeks to fully recover.  This can help relieve pain and swelling.
This can help relieve pain and swelling.
 Babies are especially at risk of falling as they learn to roll, climb, and walk. No matter how careful you are, you can’t prevent all accidents, so it’s important to know what to do when your baby falls.
Babies are especially at risk of falling as they learn to roll, climb, and walk. No matter how careful you are, you can’t prevent all accidents, so it’s important to know what to do when your baby falls.

 Then watch for changes in any symptoms. They will usually get better on their own over several days, though it can take up to 4 weeks to fully recover.
Then watch for changes in any symptoms. They will usually get better on their own over several days, though it can take up to 4 weeks to fully recover.  This can help relieve pain and swelling.
This can help relieve pain and swelling.
 Babies are especially at risk of falling as they learn to roll, climb, and walk. No matter how careful you are, you can’t prevent all accidents, so it’s important to know what to do when your baby falls.
Babies are especially at risk of falling as they learn to roll, climb, and walk. No matter how careful you are, you can’t prevent all accidents, so it’s important to know what to do when your baby falls.

 Then watch for changes in any symptoms. They will usually get better on their own over several days, though it can take up to 4 weeks to fully recover.
Then watch for changes in any symptoms. They will usually get better on their own over several days, though it can take up to 4 weeks to fully recover.  This can help relieve pain and swelling.
This can help relieve pain and swelling.
 However, injuries are possible, so caregivers should be aware of signs indicating that a baby needs a medical check after a fall.
However, injuries are possible, so caregivers should be aware of signs indicating that a baby needs a medical check after a fall.
 Even a minor cut or injury can bleed a lot, so it can look more serious than it is.
Even a minor cut or injury can bleed a lot, so it can look more serious than it is. If something seems wrong with a baby, it is essential to take them to see a doctor. It is always better to be safe and to make sure that no serious injuries occurred.
If something seems wrong with a baby, it is essential to take them to see a doctor. It is always better to be safe and to make sure that no serious injuries occurred. It is best to check the medication type and dosage with the doctor.
It is best to check the medication type and dosage with the doctor. After a fall, it is important to stay calm and quickly assess the baby. Seek emergency care immediately if necessary.
After a fall, it is important to stay calm and quickly assess the baby. Seek emergency care immediately if necessary. Additionally, we have some advice for you to follow in case this unfortunate accident happens to your child.
Additionally, we have some advice for you to follow in case this unfortunate accident happens to your child. If the fall resulted in an open wound, then you should apply gentle pressure and check for any bruising.
If the fall resulted in an open wound, then you should apply gentle pressure and check for any bruising.
 Another crucial fact to remember is that if you decide to call emergency medical services, your doctor, or you decide to go to the ER immediately, no one will fault you for taking an abundance of caution. It’s always better to make sure your baby is ok.
Another crucial fact to remember is that if you decide to call emergency medical services, your doctor, or you decide to go to the ER immediately, no one will fault you for taking an abundance of caution. It’s always better to make sure your baby is ok. But parents can prevent it.
But parents can prevent it.  In addition: when the child is smeared with baby cream or oil after bathing, it can easily slip out of the parents’ hands.
In addition: when the child is smeared with baby cream or oil after bathing, it can easily slip out of the parents’ hands.  Fortunately, this happens very rarely in children.
Fortunately, this happens very rarely in children.  But this can only be solved by medical specialists. If all is well, they will report it too. A detailed neurological examination or ultrasound examination usually provides the specialist with sufficient information.
But this can only be solved by medical specialists. If all is well, they will report it too. A detailed neurological examination or ultrasound examination usually provides the specialist with sufficient information.  But it is better to leave the baby on a special play mat on the floor – there will be nowhere to fall.
But it is better to leave the baby on a special play mat on the floor – there will be nowhere to fall.  However, doctors do not get tired of repeating: babies are actually very hardy and have a phenomenal ability to survive in extreme conditions. And yet, the only thing that can really seriously harm a child who was born perfectly healthy is trauma.
However, doctors do not get tired of repeating: babies are actually very hardy and have a phenomenal ability to survive in extreme conditions. And yet, the only thing that can really seriously harm a child who was born perfectly healthy is trauma. 
 Therefore, they get the false impression that they are not going anywhere with it. Isn’t it wonderful: to put a naked baby on a diaper so that he takes an air bath. And, nevertheless, it is here that one of the most serious dangers lies in wait for the child – falling from the changing table.
Therefore, they get the false impression that they are not going anywhere with it. Isn’t it wonderful: to put a naked baby on a diaper so that he takes an air bath. And, nevertheless, it is here that one of the most serious dangers lies in wait for the child – falling from the changing table.  As a result of a fall, the following types of injuries are possible:
As a result of a fall, the following types of injuries are possible:  You can’t turn away, even if you hold the child with your hands – he can magically slip between them. Before you start manipulating the baby, you need to prepare everything in advance and only then get him out of the crib. Very often, mom remembers that a pack of diapers is on the couch, and napkins are in the bathroom. It is better to lay a fabric on the table that would not slip – for example, a flannel diaper, a terry towel or a blanket. If the baby has outgrown the age of 2 months, then, ideally, all manipulations should be carried out on the floor or a low bed. Shaken Baby Syndrome
You can’t turn away, even if you hold the child with your hands – he can magically slip between them. Before you start manipulating the baby, you need to prepare everything in advance and only then get him out of the crib. Very often, mom remembers that a pack of diapers is on the couch, and napkins are in the bathroom. It is better to lay a fabric on the table that would not slip – for example, a flannel diaper, a terry towel or a blanket. If the baby has outgrown the age of 2 months, then, ideally, all manipulations should be carried out on the floor or a low bed. Shaken Baby Syndrome 
 Repeated brain injuries lead to quite serious consequences, which then she will have to correct all her life. The same may apply to the father, if he is the main caregiver for the baby due to the workload of the mother.
Repeated brain injuries lead to quite serious consequences, which then she will have to correct all her life. The same may apply to the father, if he is the main caregiver for the baby due to the workload of the mother.  However, there are situations when it is worth being distracted for a second – the child slipped out, fell out, got hurt. No one is immune from such situations.
However, there are situations when it is worth being distracted for a second – the child slipped out, fell out, got hurt. No one is immune from such situations. 
 If, as a result of a bruise, the baby lost consciousness, but then came to his senses again and began to behave as usual, he should still be scheduled for an appointment with a doctor.
If, as a result of a bruise, the baby lost consciousness, but then came to his senses again and began to behave as usual, he should still be scheduled for an appointment with a doctor. 
 DS-245-S
DS-245-S
 Today we will talk about how to avoid injury, where to go if a child is injured, how to prevent diseases and complications that injuries can lead to.
Today we will talk about how to avoid injury, where to go if a child is injured, how to prevent diseases and complications that injuries can lead to.  First of all, you need to call an ambulance. Raise, calm the child and call an ambulance. Some parents constantly think that the ambulance will only be in 2 hours, in 3 hours. If this is actually the case, you can get into your personal transport and drive to the nearest emergency room or to the emergency department, and there it is already qualified to help the child.
First of all, you need to call an ambulance. Raise, calm the child and call an ambulance. Some parents constantly think that the ambulance will only be in 2 hours, in 3 hours. If this is actually the case, you can get into your personal transport and drive to the nearest emergency room or to the emergency department, and there it is already qualified to help the child. 
 The strongest bones in the skull are the frontal bone, but the child rarely falls on his forehead, mainly in the occipital and parietal parts, temporal. Often these bones break no matter how high the child falls, even 10 cm.
The strongest bones in the skull are the frontal bone, but the child rarely falls on his forehead, mainly in the occipital and parietal parts, temporal. Often these bones break no matter how high the child falls, even 10 cm.  What is the next period? Or is it rare?
What is the next period? Or is it rare?  Mom comes up, lifts, soothes. How quickly should he calm down, how should the leg look, how should the child feel?
Mom comes up, lifts, soothes. How quickly should he calm down, how should the leg look, how should the child feel?  Observe, maybe even for a day, and then draw a conclusion: if the child does not get up and start acting up, then you need to go to the emergency room or emergency department.
Observe, maybe even for a day, and then draw a conclusion: if the child does not get up and start acting up, then you need to go to the emergency room or emergency department. 
 As a doctor, do you think a child needs such a device?
As a doctor, do you think a child needs such a device? 
 Right on the roller skates, with an ambulance crew, because for one reason or another, due to swelling, they could not remove the roller skates. Here, any protection will not help, it all depends on the speed of the fall, on the type of injury. Even elbow pads or a fixator on the wrist joints will not help. Helmet – yes. The helmet is the only salvation.
Right on the roller skates, with an ambulance crew, because for one reason or another, due to swelling, they could not remove the roller skates. Here, any protection will not help, it all depends on the speed of the fall, on the type of injury. Even elbow pads or a fixator on the wrist joints will not help. Helmet – yes. The helmet is the only salvation.  And up the hill?
And up the hill? 
 Everything is strictly individual. You tell some children even at the age of 3 what to do and what not to do – they understand and try not to do it. I think it is difficult to define a certain age here, but, up to 7 years, I think there is a place for control.
Everything is strictly individual. You tell some children even at the age of 3 what to do and what not to do – they understand and try not to do it. I think it is difficult to define a certain age here, but, up to 7 years, I think there is a place for control. 
 Some say: “Is it worth going to the emergency room about this?” My opinion and the opinion of most traumatologists is that on the first day you can endure if the child was injured at night or at 10 or 11 at night.
Some say: “Is it worth going to the emergency room about this?” My opinion and the opinion of most traumatologists is that on the first day you can endure if the child was injured at night or at 10 or 11 at night. 
 Often these are growing pains. Growing pains, by the way, in children, the active phase of growth goes from 3 to 7 years.
Often these are growing pains. Growing pains, by the way, in children, the active phase of growth goes from 3 to 7 years.  Over time, everything goes away completely. But I wanted to say, to add: there are children who live in the southern countries, or in the south of Russia, they have no problems with the joints in general, absolutely.
Over time, everything goes away completely. But I wanted to say, to add: there are children who live in the southern countries, or in the south of Russia, they have no problems with the joints in general, absolutely.  They come, go to the traumatologist and have a conversation. Naturally, the traumatologist, having examined the child, having carefully collected, again, I emphasize – carefully, the anamnesis is already drawing his own conclusions. If necessary – yes, any traumatologist reinsures himself, sends the child for x-rays, excludes injury. The qualification of a traumatologist, of course, does not end only with traumatology and orthopedics, he naturally gives recommendations to contact a pediatrician.
They come, go to the traumatologist and have a conversation. Naturally, the traumatologist, having examined the child, having carefully collected, again, I emphasize – carefully, the anamnesis is already drawing his own conclusions. If necessary – yes, any traumatologist reinsures himself, sends the child for x-rays, excludes injury. The qualification of a traumatologist, of course, does not end only with traumatology and orthopedics, he naturally gives recommendations to contact a pediatrician. 
 You repeated several times that the traumatologist carefully collects an anamnesis, carefully. How much time is required? As far as I remember, I don’t know how it is now, but while I was a teenager, small, the emergency room was, one might say, my second home. For as long as I can remember, the queue at the emergency room, it seems to me, is generally endless. There are always a lot of people sitting there, mothers with children, in an adult, in general, in my opinion, the line does not end. How many minutes does a pediatric traumatologist have in an emergency room in order to carefully collect an anamnesis, discuss everything, examine a child, write a conclusion, and so on? Pediatricians in polyclinics have 7-12 minutes.
You repeated several times that the traumatologist carefully collects an anamnesis, carefully. How much time is required? As far as I remember, I don’t know how it is now, but while I was a teenager, small, the emergency room was, one might say, my second home. For as long as I can remember, the queue at the emergency room, it seems to me, is generally endless. There are always a lot of people sitting there, mothers with children, in an adult, in general, in my opinion, the line does not end. How many minutes does a pediatric traumatologist have in an emergency room in order to carefully collect an anamnesis, discuss everything, examine a child, write a conclusion, and so on? Pediatricians in polyclinics have 7-12 minutes. 

 What about other injuries? Let’s say there was a cut, a fracture in a child or bruises, you still don’t know what exactly, but the child is injured. You call an ambulance or are going to go to the emergency room, but what do parents need to do, what can and cannot be done?
What about other injuries? Let’s say there was a cut, a fracture in a child or bruises, you still don’t know what exactly, but the child is injured. You call an ambulance or are going to go to the emergency room, but what do parents need to do, what can and cannot be done? 
 If there was nothing like that, or blurred symptoms, or happened in the evening, we were already going home, stumbled and fell. We ate at home, it seems that the child has eaten and is already falling asleep. Sleep or see a doctor?
If there was nothing like that, or blurred symptoms, or happened in the evening, we were already going home, stumbled and fell. We ate at home, it seems that the child has eaten and is already falling asleep. Sleep or see a doctor?  Another point: the child fell somehow unsuccessfully, and we understand that it was either a bruise or a fracture. What should we do?
Another point: the child fell somehow unsuccessfully, and we understand that it was either a bruise or a fracture. What should we do? 
 Give advice to parents, tell them where else you can get information on how to behave correctly.
Give advice to parents, tell them where else you can get information on how to behave correctly.  Do not be afraid of doctors, trust doctors, contact us!
Do not be afraid of doctors, trust doctors, contact us! 




 It is urgent to consult a doctor if there was a short-term loss of consciousness after the injury, and also if headache, nausea/vomiting, weakness and drowsiness appeared within three days after the injury. In this case, the child should be examined by a neurologist and an ophthalmologist, and an x-ray or computed tomography of the head may also be needed. If the child feels well after the injury, he still needs to be provided with a calm regime, without physical activity in the first 3 days after the injury.
It is urgent to consult a doctor if there was a short-term loss of consciousness after the injury, and also if headache, nausea/vomiting, weakness and drowsiness appeared within three days after the injury. In this case, the child should be examined by a neurologist and an ophthalmologist, and an x-ray or computed tomography of the head may also be needed. If the child feels well after the injury, he still needs to be provided with a calm regime, without physical activity in the first 3 days after the injury. 
 Gently show that the stove is hot, and the drawer can pinch your fingers. This is how cause-and-effect relationships and concepts of danger are formed. After several repetitions, the child will become more careful.
Gently show that the stove is hot, and the drawer can pinch your fingers. This is how cause-and-effect relationships and concepts of danger are formed. After several repetitions, the child will become more careful.

 It is difficult for them to sit in one place, and when it is a closed space of an apartment with many objects that a child can be injured about, the risk increases. Sports and active walks help the child get rid of this “excess” of energy.”
It is difficult for them to sit in one place, and when it is a closed space of an apartment with many objects that a child can be injured about, the risk increases. Sports and active walks help the child get rid of this “excess” of energy.”
 If you do not notice the absence of the testicles in the scrotum in time, the fertile function will be disturbed, and sometimes an oncological process may develop. And ignoring the torsion of the spermatic cord is fraught with the removal of the testicle. We talk about the most common urological problems.
If you do not notice the absence of the testicles in the scrotum in time, the fertile function will be disturbed, and sometimes an oncological process may develop. And ignoring the torsion of the spermatic cord is fraught with the removal of the testicle. We talk about the most common urological problems.  This is an event that entails the appearance of a huge number of warnings, recommendations, restrictions, and at the same time fears, anxieties, experiences in the life of a mother. What is really important to do in order to reduce the risks of premature birth of a child?
This is an event that entails the appearance of a huge number of warnings, recommendations, restrictions, and at the same time fears, anxieties, experiences in the life of a mother. What is really important to do in order to reduce the risks of premature birth of a child?

 Also, drugs are often used that do not work with a viral infection. We tell why such methods do not work, why they are dangerous and how you can save on unnecessary medicines.
Also, drugs are often used that do not work with a viral infection. We tell why such methods do not work, why they are dangerous and how you can save on unnecessary medicines.  ”
” 
 Perhaps the outflow of cerebrospinal fluid (clear liquid) or blood from the nose, ear. There are bruises around the eyes (a symptom of glasses). However, symptoms may appear several hours after the injury.
Perhaps the outflow of cerebrospinal fluid (clear liquid) or blood from the nose, ear. There are bruises around the eyes (a symptom of glasses). However, symptoms may appear several hours after the injury.  At a later age, such a study will not work if a large fontanel is overgrown.
At a later age, such a study will not work if a large fontanel is overgrown.  5-2 years).
5-2 years). 

 Some experts say frozen teething toys are too cold and may hurt your baby’s mouth. Make sure to clean teething toys, washcloths, and other items after the baby uses them.
Some experts say frozen teething toys are too cold and may hurt your baby’s mouth. Make sure to clean teething toys, washcloths, and other items after the baby uses them. Look for ones made of rubber.
Look for ones made of rubber. It can cause rare but serious side effects.
It can cause rare but serious side effects.

 This means the total teething period lasts about two years.
This means the total teething period lasts about two years.
 Your little one might seem a little fussier and may cry more than usual.
Your little one might seem a little fussier and may cry more than usual.
 4 degrees for a baby under 3 months) , contact your little one’s healthcare provider, who can determine what’s causing the fever.
4 degrees for a baby under 3 months) , contact your little one’s healthcare provider, who can determine what’s causing the fever.  Among the many ways to soothe your teething baby are these two quick ideas:
Among the many ways to soothe your teething baby are these two quick ideas:

 Once your child is about 2 years old you can start using a pea-sized amount of fluoride toothpaste. You’ll need to teach him how to rinse and spit, rather than swallowing the toothpaste.
Once your child is about 2 years old you can start using a pea-sized amount of fluoride toothpaste. You’ll need to teach him how to rinse and spit, rather than swallowing the toothpaste.


 This is completely normal—it’s the mouth’s way of making space for the bigger adult teeth that will follow.
This is completely normal—it’s the mouth’s way of making space for the bigger adult teeth that will follow.
 Each new tooth that emerges will make that smile even more adorable than it was before.
Each new tooth that emerges will make that smile even more adorable than it was before.
 In the words of all those babies out there…uh oh.
In the words of all those babies out there…uh oh.

 (Macknin et al, 2000; Wake, 2002; Sarrell et al, 2005; NICE, 2014; Eisenstadt et al, 2017)
(Macknin et al, 2000; Wake, 2002; Sarrell et al, 2005; NICE, 2014; Eisenstadt et al, 2017)
 researchgate.net/publication/12574630_Symptoms_Associated_W… [accessed 24th September 2018].
researchgate.net/publication/12574630_Symptoms_Associated_W… [accessed 24th September 2018].  Pediatrics. 128(3):471-476.
Pediatrics. 128(3):471-476.

 This causes part of the gums to separate and allow teeth to grow through. How clever is that? (Harding, 2016; NHS, 2016).
This causes part of the gums to separate and allow teeth to grow through. How clever is that? (Harding, 2016; NHS, 2016). In fact, each tooth or pair of teeth should only cause your little one pain for just over a week. In other words, for five days ahead of an appearance – ‘eruption day’ – and three days afterwards (Macknin et al, 2000).
In fact, each tooth or pair of teeth should only cause your little one pain for just over a week. In other words, for five days ahead of an appearance – ‘eruption day’ – and three days afterwards (Macknin et al, 2000).





 This Government benefit provides each eligible child $1,026 of general dental treatment over a two-year period.
This Government benefit provides each eligible child $1,026 of general dental treatment over a two-year period.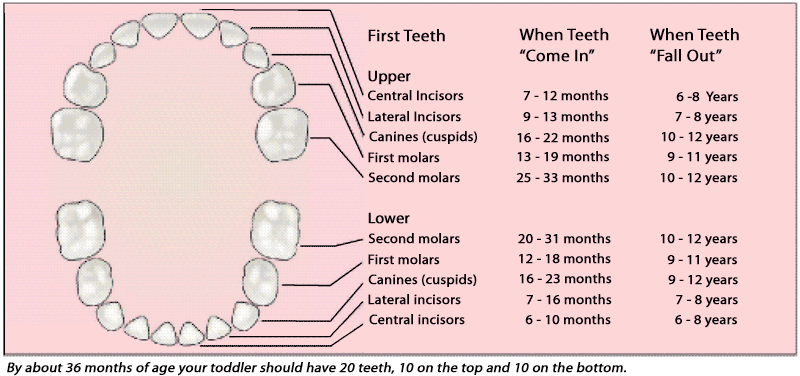 Discover teething remedies which help reduce the pain and settle your baby.
Discover teething remedies which help reduce the pain and settle your baby.



 Do not use ibuprofen medicines if your baby is under the age of 3 months.
Do not use ibuprofen medicines if your baby is under the age of 3 months. These are not safe for young infants and babies.
These are not safe for young infants and babies. If you’re tired and stressed, try asking for help from friends or family.
If you’re tired and stressed, try asking for help from friends or family. This is normally at around 6 months of age.
This is normally at around 6 months of age. This is known as ‘tongue tie’.
This is known as ‘tongue tie’.

 First, one central lower incisor appears, the second is cut almost immediately. In general, milk teeth erupt in pairs: if one climbs, then the second begins to grow almost simultaneously. It doesn’t matter if it’s an incisor, canine or premolar.
First, one central lower incisor appears, the second is cut almost immediately. In general, milk teeth erupt in pairs: if one climbs, then the second begins to grow almost simultaneously. It doesn’t matter if it’s an incisor, canine or premolar.

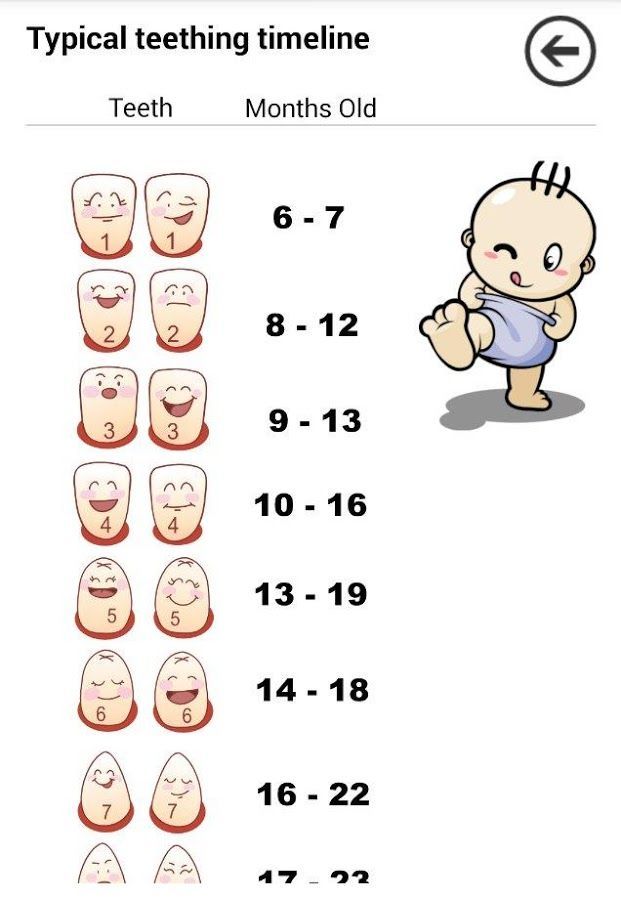 Earlier eruption is an occasion to show the child to the therapist.
Earlier eruption is an occasion to show the child to the therapist.
 Sometimes even the skin on the chest suffers from increased salivation;
Sometimes even the skin on the chest suffers from increased salivation;  There are several other reasons for this:
There are several other reasons for this:
 Values up to 38.5° are considered normal. The temperature usually lasts no more than 3 days.
Values up to 38.5° are considered normal. The temperature usually lasts no more than 3 days.
 As for Asepta’s fingertips, their advantage is the ability to “get” any place due to the soft fibers of a napkin soaked in chamomile and witch hazel extracts.
As for Asepta’s fingertips, their advantage is the ability to “get” any place due to the soft fibers of a napkin soaked in chamomile and witch hazel extracts.


 5 °. Taking antipyretics is allowed at lower values if the child is very naughty and feels unwell.
5 °. Taking antipyretics is allowed at lower values if the child is very naughty and feels unwell.

 This is one of the most common causes of restlessness, moody behavior and poor appetite in an infant in the first year of life. Let’s discuss how parents need to behave in order to help the baby get through this difficult period.
This is one of the most common causes of restlessness, moody behavior and poor appetite in an infant in the first year of life. Let’s discuss how parents need to behave in order to help the baby get through this difficult period.  At this age, many children begin to appear the first milk teeth. However, the timing of the onset of eruption can be shifted to the second half of life, this is also a variant of the norm. On average, by the 12th month of life, a child has 8 teeth and 20 by 2 years.
At this age, many children begin to appear the first milk teeth. However, the timing of the onset of eruption can be shifted to the second half of life, this is also a variant of the norm. On average, by the 12th month of life, a child has 8 teeth and 20 by 2 years.  Against the background of teething, the immune defense of the baby is often reduced, which leads to the appearance of symptoms of a viral or bacterial infection. Therefore, changes in the state of health of the crumbs can only be indirectly associated with teething. In every ambiguous situation, do not neglect the advice of a pediatrician.
Against the background of teething, the immune defense of the baby is often reduced, which leads to the appearance of symptoms of a viral or bacterial infection. Therefore, changes in the state of health of the crumbs can only be indirectly associated with teething. In every ambiguous situation, do not neglect the advice of a pediatrician. 
 Among complementary foods, the most optimal choice during teething are cereal complementary foods.
Among complementary foods, the most optimal choice during teething are cereal complementary foods.  During this period, another important advantage of the Bebi Premium line of children’s cereals is the reduced sugar content. Sugar is a good breeding ground for microbes that live in the oral cavity, its excess intake can increase the inflammatory process in the gums.
During this period, another important advantage of the Bebi Premium line of children’s cereals is the reduced sugar content. Sugar is a good breeding ground for microbes that live in the oral cavity, its excess intake can increase the inflammatory process in the gums. 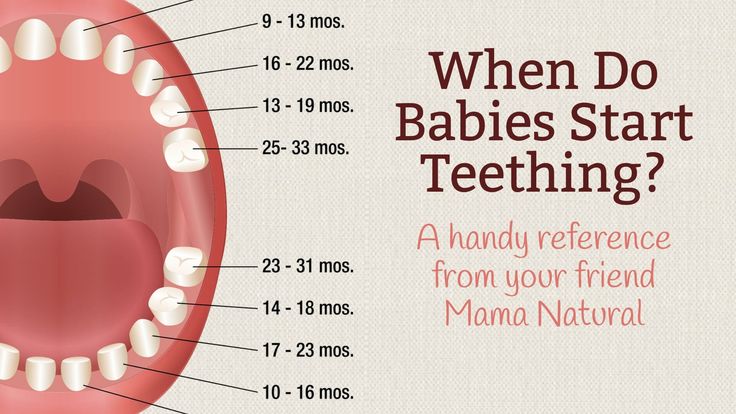 Massage improves blood flow, activates growth processes and reduces tension in the gum area. Remember, teething is a natural physiological process, and the task of parents is to help the baby to overcome this difficult life stage as comfortably as possible.
Massage improves blood flow, activates growth processes and reduces tension in the gum area. Remember, teething is a natural physiological process, and the task of parents is to help the baby to overcome this difficult life stage as comfortably as possible. 
 Today we consume a lot more thermally processed foods. The “softening” of the diet led to the fact that the “eights” lost their original function, and the jaw itself decreased. In the modern world, primary adentia of the third molar is increasingly observed, that is, a situation where rudiments of wisdom teeth are not formed .
Today we consume a lot more thermally processed foods. The “softening” of the diet led to the fact that the “eights” lost their original function, and the jaw itself decreased. In the modern world, primary adentia of the third molar is increasingly observed, that is, a situation where rudiments of wisdom teeth are not formed .  For example, they protect neighboring teeth from loosening and creating gaps in which food can accumulate. In addition, it is to the large extreme teeth that a bridge is sometimes attached.
For example, they protect neighboring teeth from loosening and creating gaps in which food can accumulate. In addition, it is to the large extreme teeth that a bridge is sometimes attached.  The gum around the cutting wisdom tooth takes the form of a pocket with a hood, under which plaque, food debris and bacteria accumulate (see Fig. 2). This causes festering and an unpleasant odor.
The gum around the cutting wisdom tooth takes the form of a pocket with a hood, under which plaque, food debris and bacteria accumulate (see Fig. 2). This causes festering and an unpleasant odor. 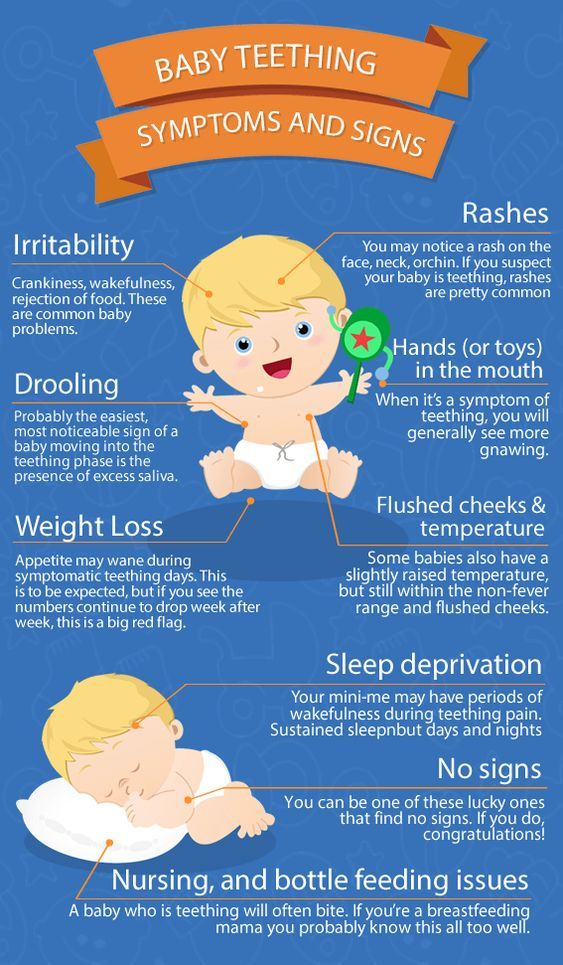

 In total, 20 milk teeth are laid in a child, while permanent ones – 32. To provide the crumbs with a Hollywood smile, the expectant mother needs to eat right throughout all nine months of pregnancy. There are no calcium preparations that would be 100% absorbed, so it is very important to draw “natural” calcium from food, especially cottage cheese. And, of course, the most pregnant woman needs to cure all her teeth – now there are very sparing technologies for this.
In total, 20 milk teeth are laid in a child, while permanent ones – 32. To provide the crumbs with a Hollywood smile, the expectant mother needs to eat right throughout all nine months of pregnancy. There are no calcium preparations that would be 100% absorbed, so it is very important to draw “natural” calcium from food, especially cottage cheese. And, of course, the most pregnant woman needs to cure all her teeth – now there are very sparing technologies for this.  Sometimes teething is delayed, and the first tooth appears closer to the year. Usually there is nothing wrong with this. It is believed that not so much the timing as the order of teething speaks about the health of the child. If it is broken, pay attention to this fact and show the baby to a pediatric dentist.
Sometimes teething is delayed, and the first tooth appears closer to the year. Usually there is nothing wrong with this. It is believed that not so much the timing as the order of teething speaks about the health of the child. If it is broken, pay attention to this fact and show the baby to a pediatric dentist. 
 In order to prevent it, you need to brush your teeth regularly: for this, you can use various massage brushes that not only teach the child to hygiene, but also facilitate the process of teething. Teeth are immediately taught to clean correctly – from the gums to the edge, slightly “sweeping”, semicircular movements, and in no case horizontal. If possible, brush your teeth after every meal (and at least twice a day). Is there no such possibility? Give the baby a drink – the water will wash away the remnants of food.
In order to prevent it, you need to brush your teeth regularly: for this, you can use various massage brushes that not only teach the child to hygiene, but also facilitate the process of teething. Teeth are immediately taught to clean correctly – from the gums to the edge, slightly “sweeping”, semicircular movements, and in no case horizontal. If possible, brush your teeth after every meal (and at least twice a day). Is there no such possibility? Give the baby a drink – the water will wash away the remnants of food.  You can check this with a pediatric dentist using the radiovisiography method. By 13–15 months , first the upper first molars appear, and then the lower ones.
You can check this with a pediatric dentist using the radiovisiography method. By 13–15 months , first the upper first molars appear, and then the lower ones.  As practice shows, there are no regularities here. Of course, if parents do not neglect the prevention of diseases and dental hygiene. At 2.5 years old, the baby normally has a full set of milk teeth. There are 20 of them – 10 on each jaw .
As practice shows, there are no regularities here. Of course, if parents do not neglect the prevention of diseases and dental hygiene. At 2.5 years old, the baby normally has a full set of milk teeth. There are 20 of them – 10 on each jaw .  To clarify the current cost, select a clinic
To clarify the current cost, select a clinic
 Every baby, no matter how healthy he is, no matter how well his mother takes care of him, goes through similar problems. Despite the fact that sleep disorders in children are much less common than in adults, doctors attach great importance to them. This is due to the role of “quality and quantity” of sleep for the normal mental and physical development of the child. Lack of sleep is associated with arousal, impulsivity, and attention deficit. Sleep problems in childhood often lead to serious problems in adulthood. The causes of sleep disorders in children can be divided into several groups. First of all, these are somatic causes – diseases that are not associated with disorders of the nervous system, but are due to the medical characteristics of the child. Almost all babies go through a period of gas and colic that starts at 1 month of age and can last up to 4 months.
Every baby, no matter how healthy he is, no matter how well his mother takes care of him, goes through similar problems. Despite the fact that sleep disorders in children are much less common than in adults, doctors attach great importance to them. This is due to the role of “quality and quantity” of sleep for the normal mental and physical development of the child. Lack of sleep is associated with arousal, impulsivity, and attention deficit. Sleep problems in childhood often lead to serious problems in adulthood. The causes of sleep disorders in children can be divided into several groups. First of all, these are somatic causes – diseases that are not associated with disorders of the nervous system, but are due to the medical characteristics of the child. Almost all babies go through a period of gas and colic that starts at 1 month of age and can last up to 4 months.  Often, to eliminate sleep disorders in this group, it is enough to consult a pediatrician. Although it is written in the literature that in most children teeth are cut painlessly and imperceptibly, at least a couple of sleepless nights are provided to you. As you understand, this is not the reason that you should try to eliminate. You need to be patient and try to help the child. Your pediatrician will recommend special tooth gels that relieve the pain of teething. True, they cannot be used often, so help to the baby will be more moral.
Often, to eliminate sleep disorders in this group, it is enough to consult a pediatrician. Although it is written in the literature that in most children teeth are cut painlessly and imperceptibly, at least a couple of sleepless nights are provided to you. As you understand, this is not the reason that you should try to eliminate. You need to be patient and try to help the child. Your pediatrician will recommend special tooth gels that relieve the pain of teething. True, they cannot be used often, so help to the baby will be more moral.  ). d.). At the physiological and psychological levels, the sleep of a small child differs not only from the sleep of adults, but also from the sleep of older children. The rhythm of activity in a newborn child is unstable. Most babies don’t have a 4-hour sleep-wake cycle until they’re 3 months old. Due to the fact that in babies the phase of the so-called REM or shallow sleep is up to 80%, the sleep of a small child is more sensitive. At this time, any discomfort: a wet diaper, hunger, cold, loud sound – can lead to awakening. For comparison, the REM sleep phase of an adult, according to various sources, ranges from 10% to 25%. You have probably observed how active the baby’s facial expressions are in a dream: he either frowns his brows, then smiles, then frowns again or even starts sucking on a hypothetical nipple. Maybe the child is dreaming of something – it is during the phase of REM sleep that the period of dreams falls, and studies have shown that the child begins to dream in the womb.
). d.). At the physiological and psychological levels, the sleep of a small child differs not only from the sleep of adults, but also from the sleep of older children. The rhythm of activity in a newborn child is unstable. Most babies don’t have a 4-hour sleep-wake cycle until they’re 3 months old. Due to the fact that in babies the phase of the so-called REM or shallow sleep is up to 80%, the sleep of a small child is more sensitive. At this time, any discomfort: a wet diaper, hunger, cold, loud sound – can lead to awakening. For comparison, the REM sleep phase of an adult, according to various sources, ranges from 10% to 25%. You have probably observed how active the baby’s facial expressions are in a dream: he either frowns his brows, then smiles, then frowns again or even starts sucking on a hypothetical nipple. Maybe the child is dreaming of something – it is during the phase of REM sleep that the period of dreams falls, and studies have shown that the child begins to dream in the womb. The baby’s eyes may not be completely closed for eyelids, and you will see that the eyeballs are moving rapidly. During this period, the child’s breathing may be uneven, general and local shudders may be observed.
The baby’s eyes may not be completely closed for eyelids, and you will see that the eyeballs are moving rapidly. During this period, the child’s breathing may be uneven, general and local shudders may be observed. 
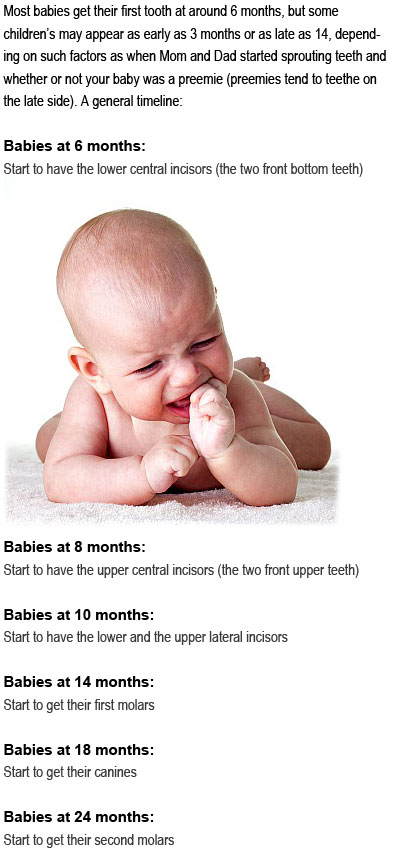 Falling asleep rituals help to put the child to sleep. From day to day, about an hour before the child needs to sleep, stick to the same regimen. It is important to create associations in the baby. Each child develops an individual rhythm of sleep and wakefulness. There are periods when it is easy for a child to fall asleep, and periods when it is very difficult to fall asleep. Watch your child carefully for a while. Even for a day of observations, you will be able to understand how many hours the periods of sleep and wakefulness replace each other in your child. Try to adjust the daily routine for them.
Falling asleep rituals help to put the child to sleep. From day to day, about an hour before the child needs to sleep, stick to the same regimen. It is important to create associations in the baby. Each child develops an individual rhythm of sleep and wakefulness. There are periods when it is easy for a child to fall asleep, and periods when it is very difficult to fall asleep. Watch your child carefully for a while. Even for a day of observations, you will be able to understand how many hours the periods of sleep and wakefulness replace each other in your child. Try to adjust the daily routine for them.  It is important not to miss the moment, put everything aside, and immediately try to put the child to bed – after all, the next moment can only be presented in a couple of hours. If the child woke up at night, in no case should he be “walked around”. Repeat a few steps from your sleep ritual (rocking, humming lullabies). It is better to prepare in advance and have on hand everything that you may need – a pacifier, a diaper, a bottle of water or formula, a mug of yogurt – which your baby usually needs. Of course, a bright light in this case is not an assistant, a night light with a subdued light is better than a bright lamp.
It is important not to miss the moment, put everything aside, and immediately try to put the child to bed – after all, the next moment can only be presented in a couple of hours. If the child woke up at night, in no case should he be “walked around”. Repeat a few steps from your sleep ritual (rocking, humming lullabies). It is better to prepare in advance and have on hand everything that you may need – a pacifier, a diaper, a bottle of water or formula, a mug of yogurt – which your baby usually needs. Of course, a bright light in this case is not an assistant, a night light with a subdued light is better than a bright lamp.  Two months later, the boy died from complications caused by the disease.
Two months later, the boy died from complications caused by the disease. 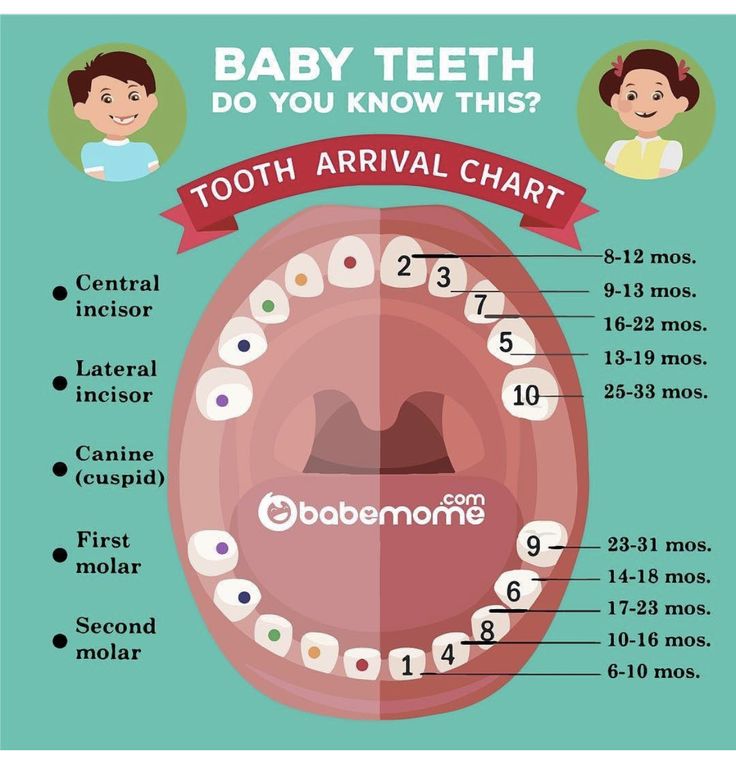 Lucas’s was 86%. Now I know it’s not normal,” says Jessica.
Lucas’s was 86%. Now I know it’s not normal,” says Jessica. 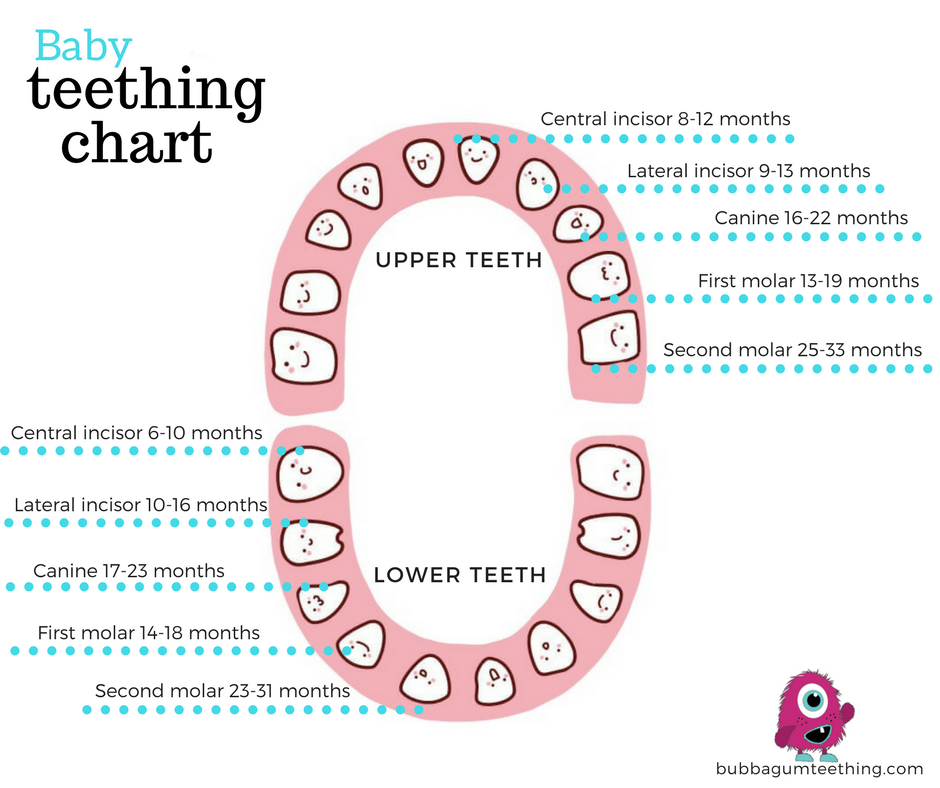
 Fatima Marinho of the University of São Paulo says she is seeing many more cases of MVS during the pandemic.
Fatima Marinho of the University of São Paulo says she is seeing many more cases of MVS during the pandemic. 

 Now their children are healthy and at home, and for me every such saved child is like a piece of Lucas,” says Jessica.
Now their children are healthy and at home, and for me every such saved child is like a piece of Lucas,” says Jessica. 


 You’ll leave with a good understanding of what and how to feed your toddler!
You’ll leave with a good understanding of what and how to feed your toddler!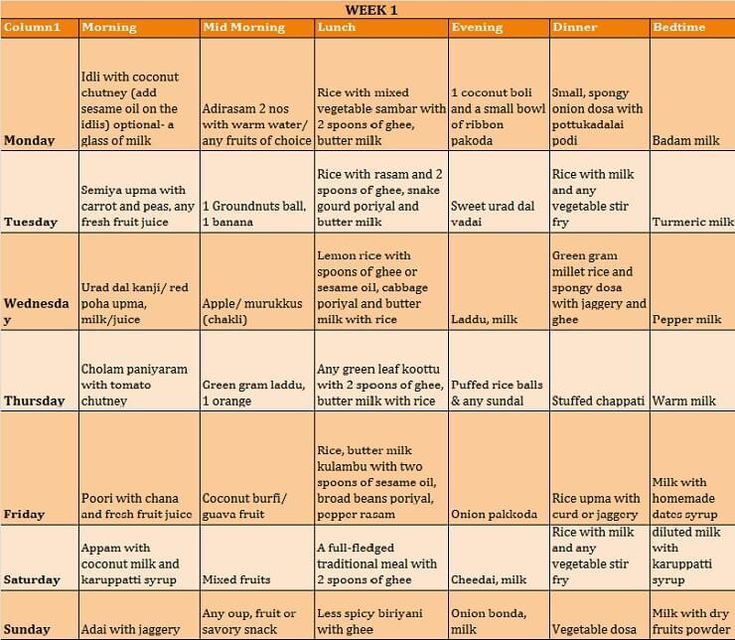 They may want to use big person utensils so they can be just like you! That’s great! We want them to eat, they want to use the utensils, perfect!
They may want to use big person utensils so they can be just like you! That’s great! We want them to eat, they want to use the utensils, perfect! All of these things make it really important to come up with meals that are balanced and have a lot of nutrients.
All of these things make it really important to come up with meals that are balanced and have a lot of nutrients. This trick and having a toddler feeding schedule, can help toddlers not ask for snacks every 10 minutes!
This trick and having a toddler feeding schedule, can help toddlers not ask for snacks every 10 minutes! Here’s a short list of green and orange veggies to focus on:
Here’s a short list of green and orange veggies to focus on:
 Read to learn more!)
Read to learn more!) Here are a few places where you can find help for your specific issue:
Here are a few places where you can find help for your specific issue: And carrots and cabbage will add vitamins and fiber, make this dish a great lunch or dinner for the whole family. Especially it will appeal to children from about 2.5 years. In this case, take lean minced veal. It is especially tasty to cook this dish from young vegetables: cabbage and carrots.
And carrots and cabbage will add vitamins and fiber, make this dish a great lunch or dinner for the whole family. Especially it will appeal to children from about 2.5 years. In this case, take lean minced veal. It is especially tasty to cook this dish from young vegetables: cabbage and carrots. 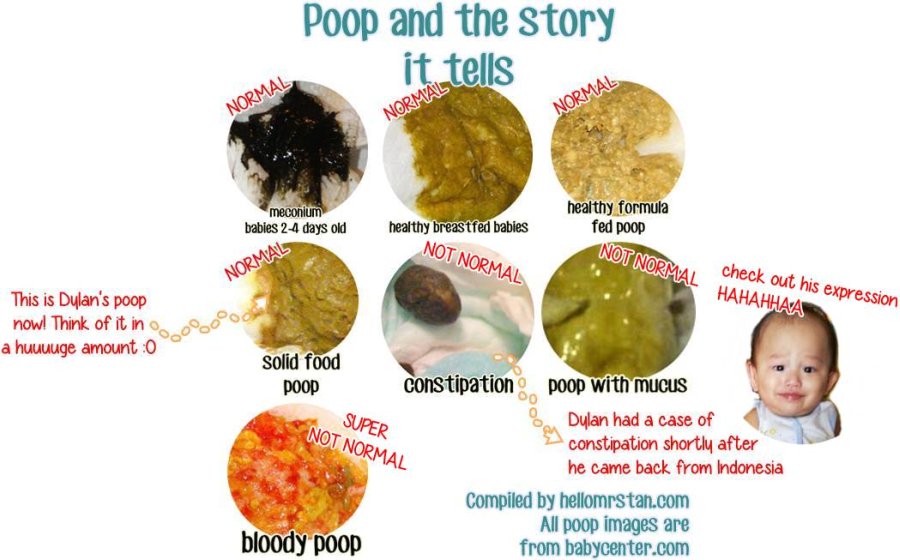
 Therefore, the recipe for pumpkin puree soup will appeal to the whole family: moms – because it is healthy, dads – because it is delicious, and children – because the soup is orange! 🙂
Therefore, the recipe for pumpkin puree soup will appeal to the whole family: moms – because it is healthy, dads – because it is delicious, and children – because the soup is orange! 🙂  Add spices to taste. For example: salt, pepper, bay leaf, a little celery, parsley. Boil for about 15-20 minutes. I had a baked chicken breast and frozen broth, so I skipped the chicken cooking process.
Add spices to taste. For example: salt, pepper, bay leaf, a little celery, parsley. Boil for about 15-20 minutes. I had a baked chicken breast and frozen broth, so I skipped the chicken cooking process. 
 Some babies may need you to stay in the room until they are asleep
Some babies may need you to stay in the room until they are asleep No matter what you try, it does not work. If you start to feel tired, frustrated, upset or anxious, it’s very likely that your baby will also remain upset and unsettled.
No matter what you try, it does not work. If you start to feel tired, frustrated, upset or anxious, it’s very likely that your baby will also remain upset and unsettled.  I can’t put him into the cot/bassinet because he keeps crying. The only way he will go to sleep is on me.
I can’t put him into the cot/bassinet because he keeps crying. The only way he will go to sleep is on me.
 A sleep cycle is around 30-50 minutes and then babies can rouse. It’s very common for babies to wake up after 30-40 minutes sleep at this age. There are several ways of re-settling baby. Hands-on settling is one option where you comfort your baby with gentle ‘ssshh’ sounds, gentle rhythmic patting, rocking or stroking until baby is calm or asleep. If your baby becomes or stays distressed pick him up for a cuddle until calm or asleep before putting baby back in the cot. Stay with your baby until he/she is asleep.
A sleep cycle is around 30-50 minutes and then babies can rouse. It’s very common for babies to wake up after 30-40 minutes sleep at this age. There are several ways of re-settling baby. Hands-on settling is one option where you comfort your baby with gentle ‘ssshh’ sounds, gentle rhythmic patting, rocking or stroking until baby is calm or asleep. If your baby becomes or stays distressed pick him up for a cuddle until calm or asleep before putting baby back in the cot. Stay with your baby until he/she is asleep. Try lots of reassurance :
Try lots of reassurance :
 or screaming and restless. If chatting, leave him. If screaming, check how he is used to settling…. is he needing some help with learning new ways to settle? A predictable bedtime routine (sequence of activities) including a wind-down period (for example, meal, bath, cleaning teeth, story time, brief cuddle and kiss, and into bed) is important to help your child recognise and establish good sleep patterns. In preparation for sleep, a bedtime routine (depending on day or night) encourages a wind-down period and ensures that your child’s physical needs are met.
or screaming and restless. If chatting, leave him. If screaming, check how he is used to settling…. is he needing some help with learning new ways to settle? A predictable bedtime routine (sequence of activities) including a wind-down period (for example, meal, bath, cleaning teeth, story time, brief cuddle and kiss, and into bed) is important to help your child recognise and establish good sleep patterns. In preparation for sleep, a bedtime routine (depending on day or night) encourages a wind-down period and ensures that your child’s physical needs are met. It can take time for children to sleep longer in the morning so set realistic goals and be consistent with self settling methods.
It can take time for children to sleep longer in the morning so set realistic goals and be consistent with self settling methods. It can take up to 6 months for older children to adjust to a new baby. Being mindful of the adjustments your older child needs to make to a new baby in the household and demands on your time, is helpful. If possible involve your older child with caring for the new baby and there are lots of ways you can do this (i.e. at nappy change time, bathing time etc.). Set limits and be clear about boundaries with the older child.
It can take up to 6 months for older children to adjust to a new baby. Being mindful of the adjustments your older child needs to make to a new baby in the household and demands on your time, is helpful. If possible involve your older child with caring for the new baby and there are lots of ways you can do this (i.e. at nappy change time, bathing time etc.). Set limits and be clear about boundaries with the older child. Giving your baby a bottle is usually not the answer. In fact, it may even make your baby more unsettled. Firstly, start by visiting your child and family health nurse and asking her to assess one of your feeds. The nurse will observe a breastfeed and possibly also weigh your baby. She may suggest strategies to increase your milk supply if your baby is not gaining adequate weight. These might include increasing the number of times you breastfeed, expressing a small amount of milk before the feed, resting more and drinking more water. However the issue may be the way you are currently settling your baby to sleep. So, it would also be worthwhile explaining to the Nurse how you put baby to sleep (for example do you wrap baby, and are you consistent in the way you put baby to sleep every time. Again, your Child and Family Health Nurse can advise you on some new strategies to try at home.
Giving your baby a bottle is usually not the answer. In fact, it may even make your baby more unsettled. Firstly, start by visiting your child and family health nurse and asking her to assess one of your feeds. The nurse will observe a breastfeed and possibly also weigh your baby. She may suggest strategies to increase your milk supply if your baby is not gaining adequate weight. These might include increasing the number of times you breastfeed, expressing a small amount of milk before the feed, resting more and drinking more water. However the issue may be the way you are currently settling your baby to sleep. So, it would also be worthwhile explaining to the Nurse how you put baby to sleep (for example do you wrap baby, and are you consistent in the way you put baby to sleep every time. Again, your Child and Family Health Nurse can advise you on some new strategies to try at home.
 However, once any medical cause is ruled out, parents can be reassured that normal crying peaks at this age and will decrease naturally from about 5 months of age.
However, once any medical cause is ruled out, parents can be reassured that normal crying peaks at this age and will decrease naturally from about 5 months of age.

 )
)


 No wonder you’re seeing an increase in fussiness!
No wonder you’re seeing an increase in fussiness! This can certainly cause your baby to be extra fussy if he is having an allergic reaction to any of his foods.
This can certainly cause your baby to be extra fussy if he is having an allergic reaction to any of his foods. 

 This is why your baby might suddenly be super fussy at night and cry way more often than normal.
This is why your baby might suddenly be super fussy at night and cry way more often than normal.  We will research your concern and make corrections accordingly.
We will research your concern and make corrections accordingly. If you see a review that does not reflect these guidelines, you can email us. We will assess
If you see a review that does not reflect these guidelines, you can email us. We will assess J. Bryan Elementary
J. Bryan Elementary Each baby completes these milestones at different times, but our teachers at Kids Castle are working with you and your baby to help your baby grow and achieve each milestone in his/her development.
Each baby completes these milestones at different times, but our teachers at Kids Castle are working with you and your baby to help your baby grow and achieve each milestone in his/her development.  We consider Kids Castle an extension of your home, and are committed to make this first transition easy for both you and your baby.
We consider Kids Castle an extension of your home, and are committed to make this first transition easy for both you and your baby.  Your child’s feeding routine will be maintained during his/her time at Kids Castle.
Your child’s feeding routine will be maintained during his/her time at Kids Castle.  com
com org/ListItem”> Innovative project sites MPADO
org/ListItem”> Innovative project sites MPADO
 05.2022 12:30)
05.2022 12:30) 11.2020 14:00)
11.2020 14:00) Nasyr-Kort District, st. Bakinskaya, d.8
Nasyr-Kort District, st. Bakinskaya, d.8  Gorchkhanov Ul, d 5
Gorchkhanov Ul, d 5  13 enforcement proceedings were initiated against the company, of which 2 are ongoing. GBDOU KINDERGARTEN №1 NAZRANI FAGIC CASTLE participated in 27 arbitration cases: in 1 as a plaintiff, and in 26 as a defendant.
13 enforcement proceedings were initiated against the company, of which 2 are ongoing. GBDOU KINDERGARTEN №1 NAZRANI FAGIC CASTLE participated in 27 arbitration cases: in 1 as a plaintiff, and in 26 as a defendant. 
 No two baby’s feet are the same (and sometimes your baby’s own feet will be slightly different sizes from each other), and there is no universal standard for age-based sizing.
No two baby’s feet are the same (and sometimes your baby’s own feet will be slightly different sizes from each other), and there is no universal standard for age-based sizing.
 Here are a few mom tested and approved ways to confirm a perfect fit:
Here are a few mom tested and approved ways to confirm a perfect fit: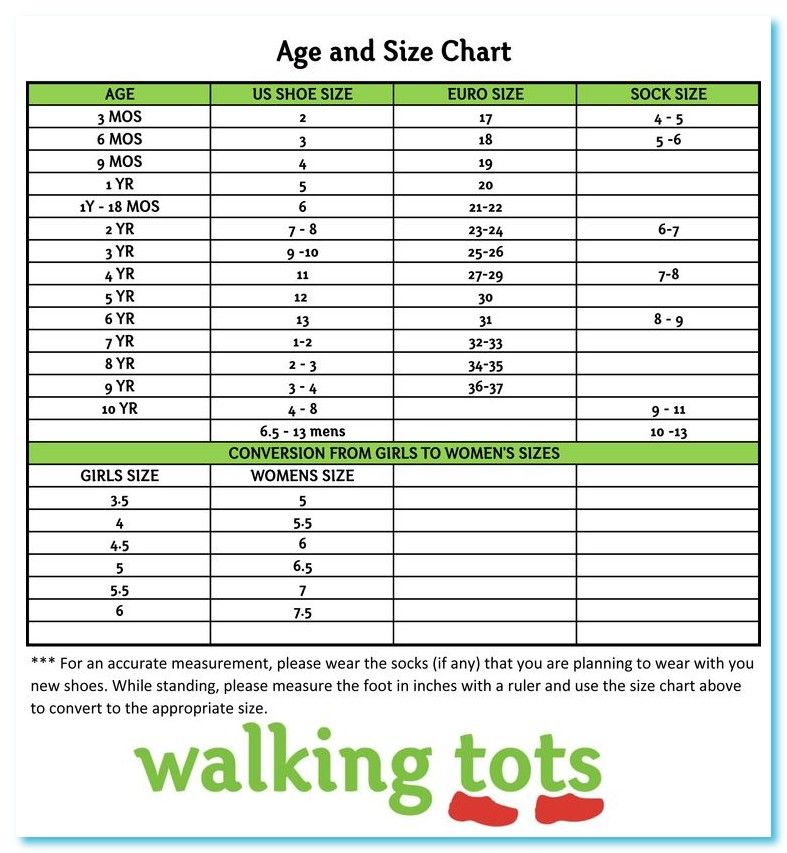 The great thing about soft sole shoes like baby moccasins is that they stretch to fit the width of your child’s feet. Moccs are perfect for both skinny feet and those larger babies who have what we in our family call “Flintstone Feet.”
The great thing about soft sole shoes like baby moccasins is that they stretch to fit the width of your child’s feet. Moccs are perfect for both skinny feet and those larger babies who have what we in our family call “Flintstone Feet.”

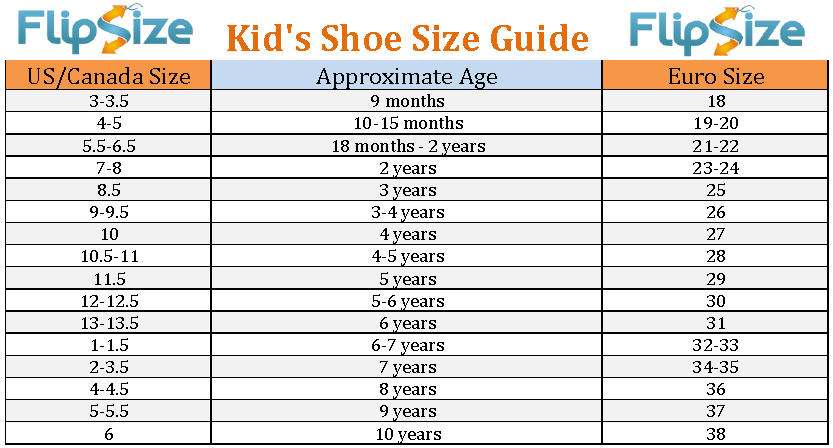 8 cm
8 cm These slip-resistant shoes flex and bend with every step as your
These slip-resistant shoes flex and bend with every step as your

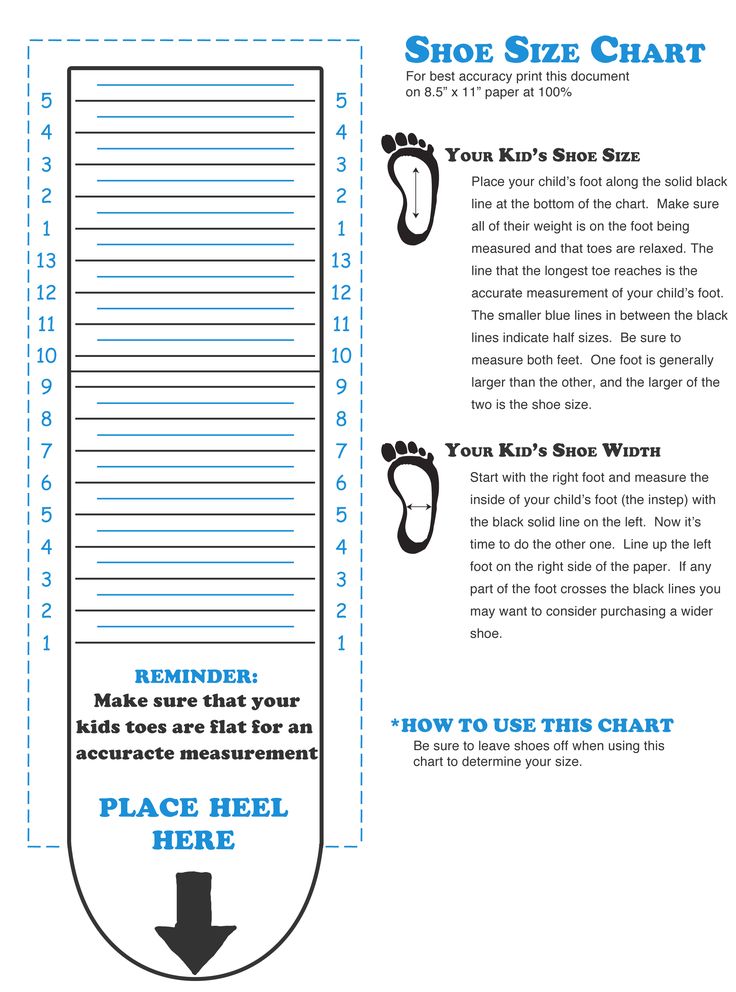 4 cm
4 cm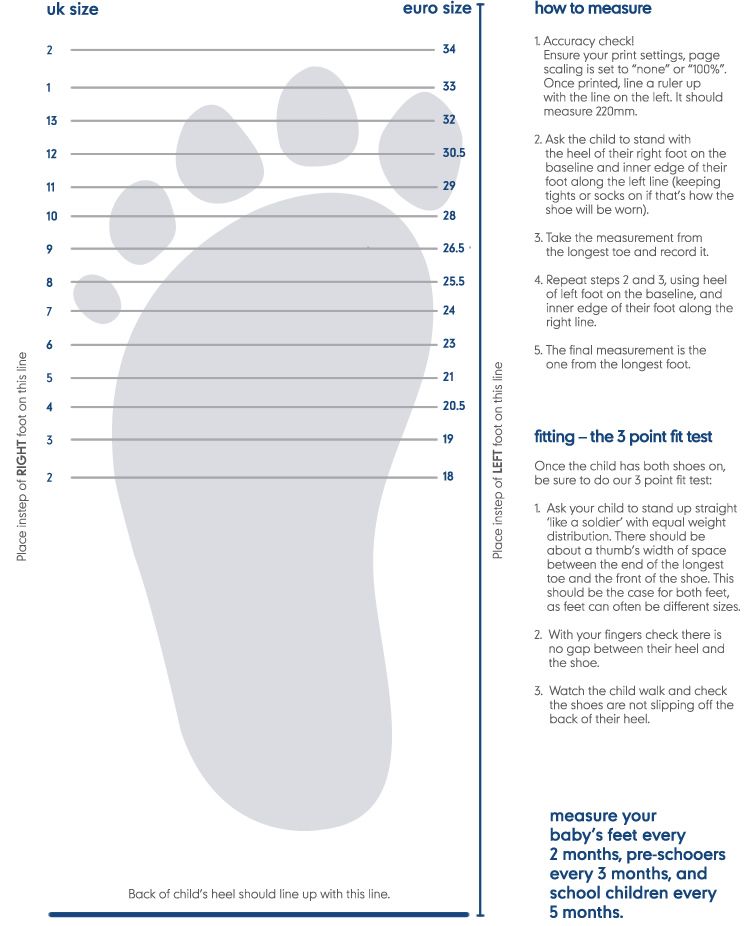 4 cm
4 cm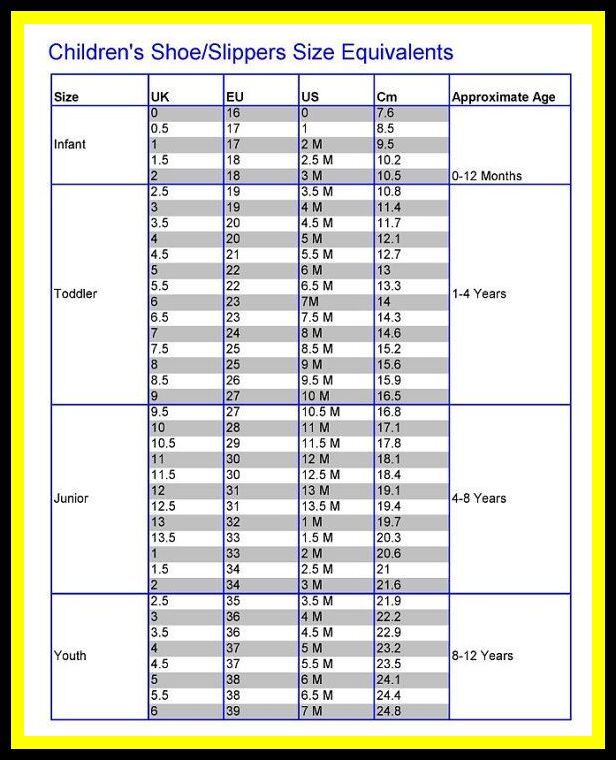
 1 cm
1 cm

 5
5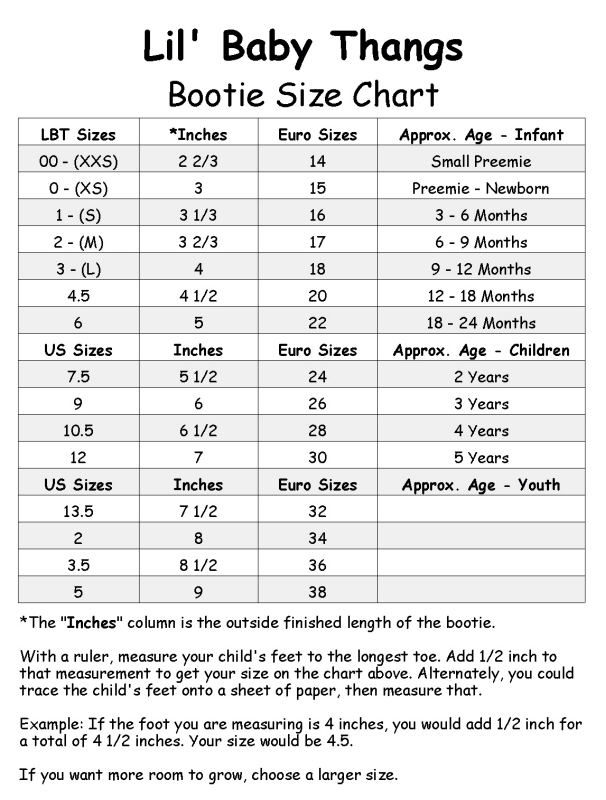 7
7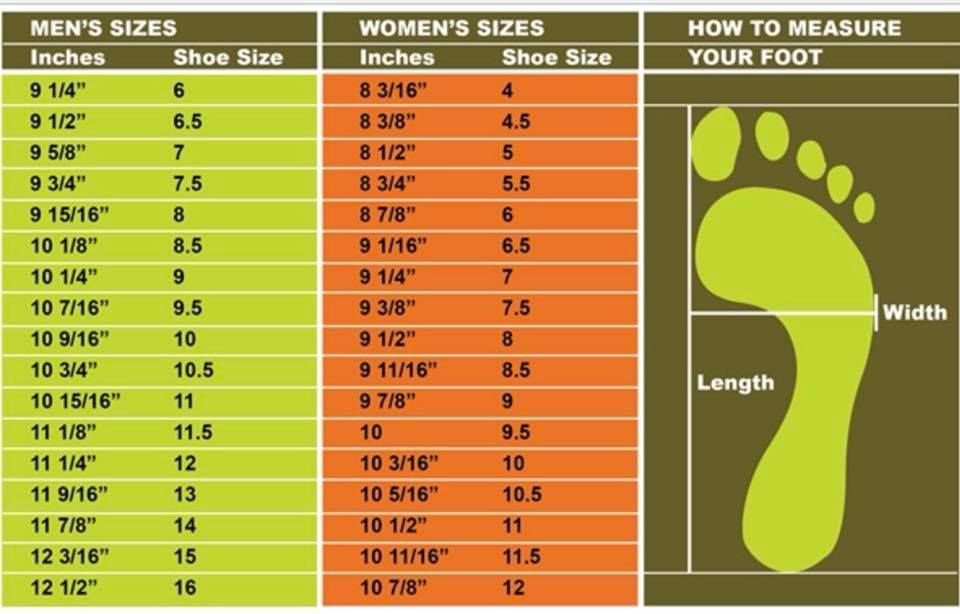 1
1
 1 cm
1 cm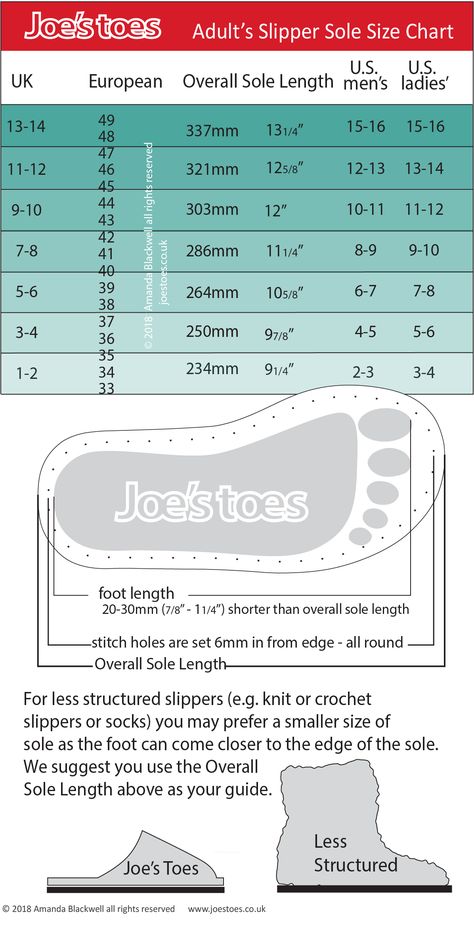 These are ideal for beach days, park trips, and any kind of kiddie
These are ideal for beach days, park trips, and any kind of kiddie
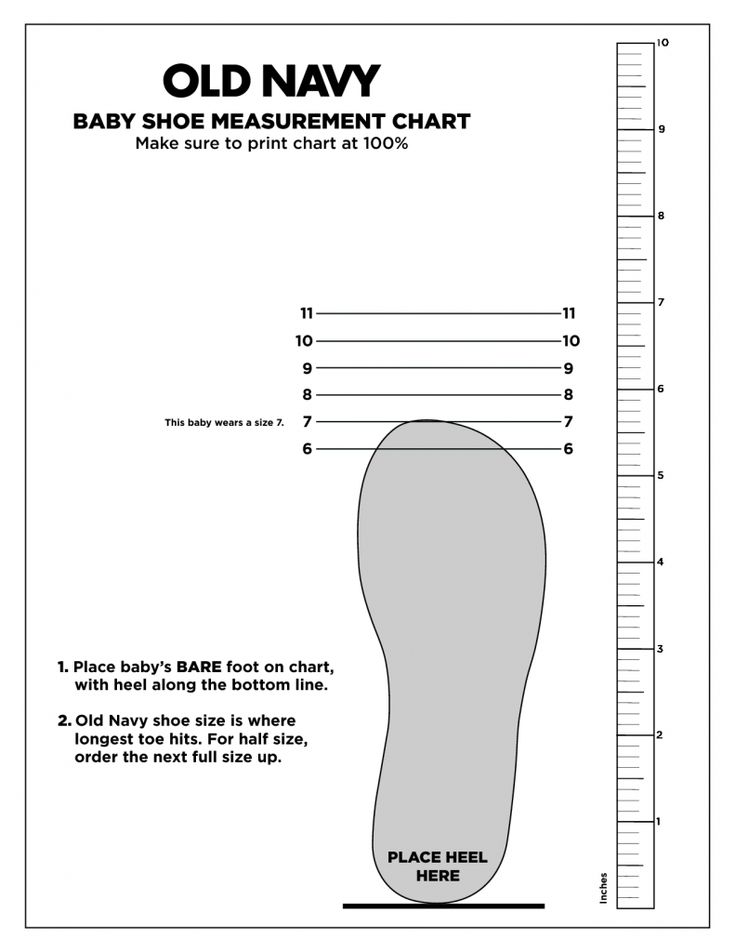 9 cm
9 cm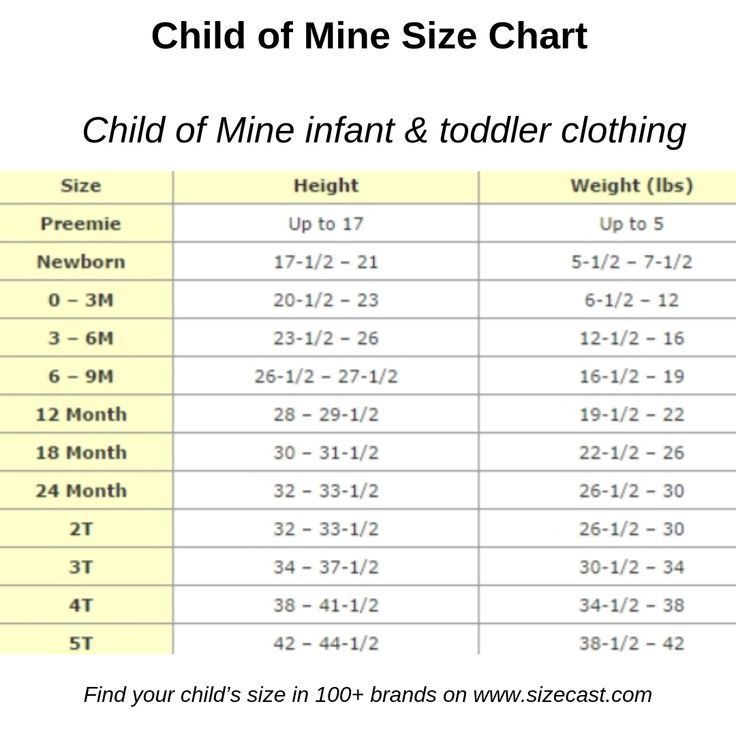 3 cm
3 cm 5
5 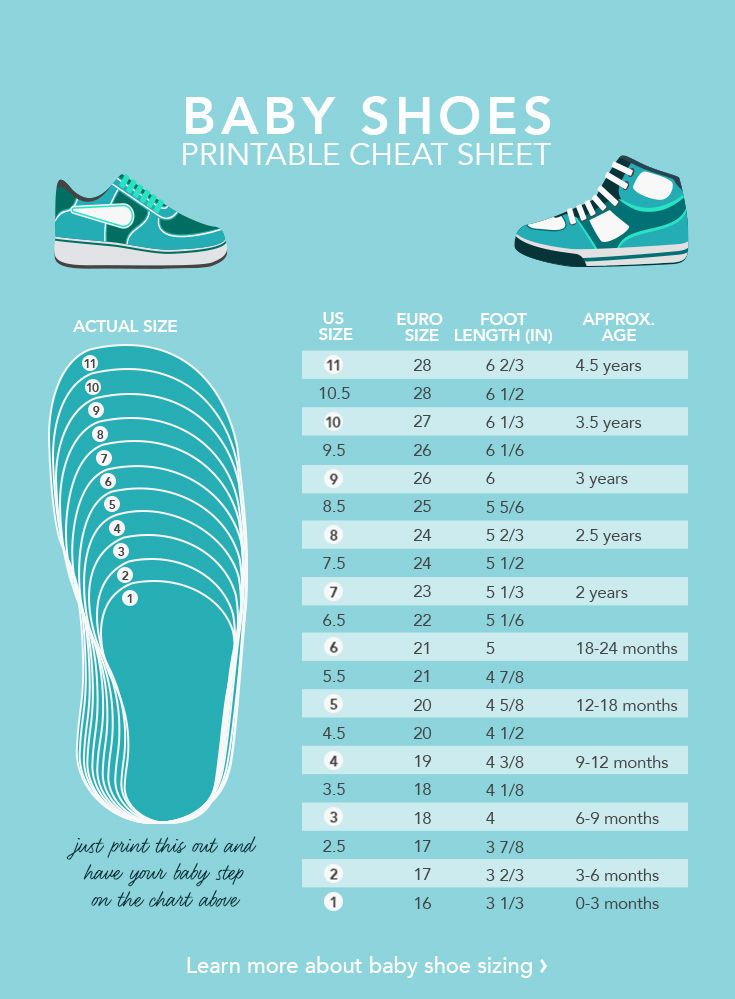 5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 510035 22.5
5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 51.5 510035 22.5  5
5 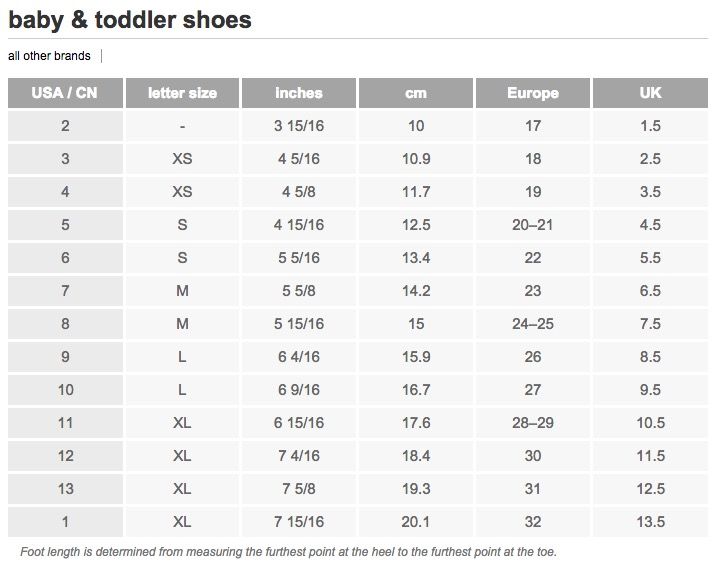 5
5  5
5  5
5  5
5  5
5  The key to choosing the right shoes lies in the parents’ understanding of the nature of children’s development. In the previous article , we talked about this in detail and now we know that flat feet occur in 100% of newborns, arch formation begins around 3-5 years – flattening of the foot goes away on its own during the first 10-12 years of life.
The key to choosing the right shoes lies in the parents’ understanding of the nature of children’s development. In the previous article , we talked about this in detail and now we know that flat feet occur in 100% of newborns, arch formation begins around 3-5 years – flattening of the foot goes away on its own during the first 10-12 years of life. 

 Due to its excessive rigidity, heaviness and fixation, it can be compared with plaster on a healthy leg, which affects the state of development as a whole. It leads the child to excessive fatigue, and the discomfort that this shoe causes causes aching pain, reducing children’s activity to a minimum. The plasticity of gait is lost, the knee joint is involved in an irreversible process, and then the entire leg and spine. It becomes the cause of both acquired flat feet and other unpleasant diagnoses already in older, adult and even old age.
Due to its excessive rigidity, heaviness and fixation, it can be compared with plaster on a healthy leg, which affects the state of development as a whole. It leads the child to excessive fatigue, and the discomfort that this shoe causes causes aching pain, reducing children’s activity to a minimum. The plasticity of gait is lost, the knee joint is involved in an irreversible process, and then the entire leg and spine. It becomes the cause of both acquired flat feet and other unpleasant diagnoses already in older, adult and even old age.  Being aware of this and providing the child with the right and high-quality shoes is the task of every conscious parent.
Being aware of this and providing the child with the right and high-quality shoes is the task of every conscious parent. 
 The straw and sippy cup can aid in teaching your child how to suck. See who can blow the most bubbles, or blow a feather across the table. Teaching him or her to use the mouth in different ways strengthens different oral muscle groups. Encourage playing with food by licking yogurt or applesauce from their lips or off of plates. Picking up cheerios with their mouth and other food play will help them shape their tongue and lips to not only keep the drool in their mouth, but articulate words as well. When they’ve graduated to different foods, give them fruit leather, dried fruit, or breakfast bars to chew on. This will help their oral muscles exercise and grow.
The straw and sippy cup can aid in teaching your child how to suck. See who can blow the most bubbles, or blow a feather across the table. Teaching him or her to use the mouth in different ways strengthens different oral muscle groups. Encourage playing with food by licking yogurt or applesauce from their lips or off of plates. Picking up cheerios with their mouth and other food play will help them shape their tongue and lips to not only keep the drool in their mouth, but articulate words as well. When they’ve graduated to different foods, give them fruit leather, dried fruit, or breakfast bars to chew on. This will help their oral muscles exercise and grow. It is better to check and be wrong, than let something continue to fester, undiagnosed.
It is better to check and be wrong, than let something continue to fester, undiagnosed. ru
ru
 A child between the ages of 3 and 6 begins to explore his sexuality: exploring the difference between boys and girls, showing love to a parent of the opposite sex, then to peers, first interpersonal emotional experiences, and so on. During this period, it is important that parents not only adequately respond to the manifestations of sexuality in their child, but also set certain limits and restrictions.
A child between the ages of 3 and 6 begins to explore his sexuality: exploring the difference between boys and girls, showing love to a parent of the opposite sex, then to peers, first interpersonal emotional experiences, and so on. During this period, it is important that parents not only adequately respond to the manifestations of sexuality in their child, but also set certain limits and restrictions.  .. Creepy, but understandable.
.. Creepy, but understandable.  Why a Tyumen native is against talking about contraceptives and HIV in schools
Why a Tyumen native is against talking about contraceptives and HIV in schools  Fortunately, the teacher intervened in time, and the conflict seemed to fade away.
Fortunately, the teacher intervened in time, and the conflict seemed to fade away.  Inclusion is when no one is a victim to anyone. No one should sacrifice their interests for the sake of a child with special needs. Conversely, a child with special needs should not sacrifice anything.
Inclusion is when no one is a victim to anyone. No one should sacrifice their interests for the sake of a child with special needs. Conversely, a child with special needs should not sacrifice anything. 
 Yes, it is often said that there are no such specialists. There may not be a comprehensive school, but the city budget of the education committee provides funding for the work of such specialists.
Yes, it is often said that there are no such specialists. There may not be a comprehensive school, but the city budget of the education committee provides funding for the work of such specialists.  I think that here the child needs not so much a tutor – an assistant in his studies, as a moderator of relations.
I think that here the child needs not so much a tutor – an assistant in his studies, as a moderator of relations. 
 Does that mean they’re doing it for nothing?
Does that mean they’re doing it for nothing?  Or go where everyone is one-legged. This dilemma is completely unethical. Because nobody wins.
Or go where everyone is one-legged. This dilemma is completely unethical. Because nobody wins.  I have had occasion to communicate with people with autism with excellent higher education. Despite this, they had the highest level of anxiety and inability to work in one place.
I have had occasion to communicate with people with autism with excellent higher education. Despite this, they had the highest level of anxiety and inability to work in one place.  They just don’t know how it will be. They also need to be enlightened – fears, myths, prejudices like “my child will adopt bad habits” or “here the slobber sits and will pull the class back” should be removed.
They just don’t know how it will be. They also need to be enlightened – fears, myths, prejudices like “my child will adopt bad habits” or “here the slobber sits and will pull the class back” should be removed. 
 By 18 months, when the first big burst of spoken words generally occurs, a:
By 18 months, when the first big burst of spoken words generally occurs, a:
 com.au and an early intervention Speech Pathologist will respond to you!
com.au and an early intervention Speech Pathologist will respond to you!

 You will have full 24/7 access to the eProgram for 12 months from the date of purchase. Let’s get started TODAY!
You will have full 24/7 access to the eProgram for 12 months from the date of purchase. Let’s get started TODAY!
 You’re at higher risk of developing dysarthria if you:
You’re at higher risk of developing dysarthria if you: If your symptoms are related to an underlying medical condition, your doctor may recommend medications, surgery, speech-language therapy, or other treatments to address it.
If your symptoms are related to an underlying medical condition, your doctor may recommend medications, surgery, speech-language therapy, or other treatments to address it. But you can reduce your risk of dysarthria by following a healthy a lifestyle that lowers your chance of stroke. For example:
But you can reduce your risk of dysarthria by following a healthy a lifestyle that lowers your chance of stroke. For example: For example, the American Speech-Language-Hearing Association reports that about two-thirds of adults with central nervous system disease can improve their speech skills with the help of a speech-language pathologist.
For example, the American Speech-Language-Hearing Association reports that about two-thirds of adults with central nervous system disease can improve their speech skills with the help of a speech-language pathologist. In fact, this approach is fundamentally wrong. There are physiological norms for proper speech and mental development, and it is very important to monitor their observance from the very birth of a child. Only in this case, he will be able to develop harmoniously and fully.
In fact, this approach is fundamentally wrong. There are physiological norms for proper speech and mental development, and it is very important to monitor their observance from the very birth of a child. Only in this case, he will be able to develop harmoniously and fully.  During the period of true “humming” sounds become long, melodious and more diverse. Along with guttural and vowels, labial sounds and combinations of vowels with labials are increasingly appearing.
During the period of true “humming” sounds become long, melodious and more diverse. Along with guttural and vowels, labial sounds and combinations of vowels with labials are increasingly appearing.  It becomes more expressive, symbolic gestures appear. The child can communicate with one hand. Babble words of various intonations appear.
It becomes more expressive, symbolic gestures appear. The child can communicate with one hand. Babble words of various intonations appear.  ” At the same time, he can still pronounce some sounds indistinctly. By the age of three, a child’s speech has up to 1200-1500 words, including almost all parts of speech.
” At the same time, he can still pronounce some sounds indistinctly. By the age of three, a child’s speech has up to 1200-1500 words, including almost all parts of speech.  The same thing happens with speech: it develops gradually. The child not only memorizes new words, but at the same time trains articulatory muscles, learns to control intonation. It takes more than one year. Therefore, if at 3-3.5 years old your child is just beginning to pronounce the first words and build simple phrases like “mom, give me,” then by the age of six, when it’s time to go to school, he will not form a full-fledged phrasal speech. It is important to engage in the development of speech gradually, but from a very early age.
The same thing happens with speech: it develops gradually. The child not only memorizes new words, but at the same time trains articulatory muscles, learns to control intonation. It takes more than one year. Therefore, if at 3-3.5 years old your child is just beginning to pronounce the first words and build simple phrases like “mom, give me,” then by the age of six, when it’s time to go to school, he will not form a full-fledged phrasal speech. It is important to engage in the development of speech gradually, but from a very early age.  Most often, the reason is the excessive passion of parents for mechanical sound, that is, the sound from a TV, computer, tablet, phone. Children who watch a lot of cartoons or constantly play with singing-talking toys develop passive speech well, but their own active speech is not formed. This is due to the difference in the wavelength of live speech and mechanical speech. In order for the child to start talking, you need to talk with him as much as possible, read fairy tales yourself, sing lullabies.
Most often, the reason is the excessive passion of parents for mechanical sound, that is, the sound from a TV, computer, tablet, phone. Children who watch a lot of cartoons or constantly play with singing-talking toys develop passive speech well, but their own active speech is not formed. This is due to the difference in the wavelength of live speech and mechanical speech. In order for the child to start talking, you need to talk with him as much as possible, read fairy tales yourself, sing lullabies.  At a year and a half, the child is able to hold the bladder, control his pelvic functions. This is one of the important links in mental development. Of course, he will eventually learn to ask to use the toilet himself, but these skills will come much later and no longer in the form in which he would like.
At a year and a half, the child is able to hold the bladder, control his pelvic functions. This is one of the important links in mental development. Of course, he will eventually learn to ask to use the toilet himself, but these skills will come much later and no longer in the form in which he would like. 


 I mean the situation when a pacifier or mother’s breast is in the child’s mouth not for calming or feeding, but just like that, in a state of wakefulness. In this case, the problem arises purely mechanical: in order to speak, the mouth must be free, and if the mouth is occupied, then it is impossible to speak – the nipple or chest interferes.
I mean the situation when a pacifier or mother’s breast is in the child’s mouth not for calming or feeding, but just like that, in a state of wakefulness. In this case, the problem arises purely mechanical: in order to speak, the mouth must be free, and if the mouth is occupied, then it is impossible to speak – the nipple or chest interferes.  But by the age of two, the child already understands the addressed speech well, he can speak himself, so this connection only strengthens and will not be interrupted after weaning the child from the breast.
But by the age of two, the child already understands the addressed speech well, he can speak himself, so this connection only strengthens and will not be interrupted after weaning the child from the breast.  Nobody says that you don’t need to use TV and gadgets at all. This is an important part of modern life, children should be able to master them. But a small child still does not have the skills of speech, movements, motor skills, proper mental development, criticism, self-criticism, and the ability to control oneself are incorrectly formed. Therefore, it is very dangerous to uncontrollably give him something that can provoke improper development.
Nobody says that you don’t need to use TV and gadgets at all. This is an important part of modern life, children should be able to master them. But a small child still does not have the skills of speech, movements, motor skills, proper mental development, criticism, self-criticism, and the ability to control oneself are incorrectly formed. Therefore, it is very dangerous to uncontrollably give him something that can provoke improper development. 
 What should he say at the age of 2-2.2 years, how to talk to him and identify deviations from the norm.
What should he say at the age of 2-2.2 years, how to talk to him and identify deviations from the norm.  Taking into account the individual development of each baby, the norms are applicable to the age from 2 years to 2 years and 2 months.
Taking into account the individual development of each baby, the norms are applicable to the age from 2 years to 2 years and 2 months.
 For example, if a child says at 2 years old like this: at home – “home”, a beautiful jacket – “beautiful jacket”, a rug – “carpet”, then this is normal.
For example, if a child says at 2 years old like this: at home – “home”, a beautiful jacket – “beautiful jacket”, a rug – “carpet”, then this is normal.


 For example, there are only babbling words and onomatopoeia, which is appropriate at 1 year;
For example, there are only babbling words and onomatopoeia, which is appropriate at 1 year;  There is no need to read advice on the forums and hope for a miracle: “We also kept silent, kept silent, and then how to speak! His dad also did not talk for a long time, and nothing, everything is fine … “. Someone waits like this until 3-4 and even 5 years, after which only a speech therapist will no longer help.
There is no need to read advice on the forums and hope for a miracle: “We also kept silent, kept silent, and then how to speak! His dad also did not talk for a long time, and nothing, everything is fine … “. Someone waits like this until 3-4 and even 5 years, after which only a speech therapist will no longer help.

