






What causes excessive drooling in babies: Baby Drooling? 5 Revealing Things About Your (Adorable) Drooling Monster
Sialorrhea (Excessive Drooling): Causes, Symptoms and Treatments
Nationwide Children’s Hospital
Meet Dr. Murakami
Improving children’s lives through innovative imagining
Close Video
Overview
Causes
Signs & Symptoms
Diagnosis
Treatment
Seeking Help
What is Sialorrhea (Excessive Drooling)?
Sialorrhea or hypersalivation literally means excessive saliva flow. Patients with sialorrhea will manifest this problem in one of two principle ways. Anterior sialorrhea is when patients have excessive anterior or forward spillage of saliva from their mouths, commonly called drooling, onto their faces and clothes causing difficulty with cleanliness, skin care, and socialization. Posterior sialorrhea is when patients have excessive posterior spillage of saliva from their mouths down their airways (tracheas) rather than being swallowed normally. This results in chronic lung irritation called aspiration which can sometimes progress to pneumonia. Often patients have a mixture of both of these types of sialorrhea.
What Causes Excessive Drooling?
Usually sialorrhea results from a decrease in normal control of oral (mouth and throat) sensation and motor function. This diminished oral control results in the inability to manage normal swallowing of saliva or inattention to the need to swallow saliva. There are a variety of causes for this condition but usually it results from brain abnormalities such as cerebral palsy, prior brain injury such as stroke, congenital abnormalities of brain development, or traumatic brain injury. Usually the sialorrhea does not worsen over time if the patient has a brain injury which does not progress with time (static brain injury). Sometimes, if the child’s underlying condition leads to a deterioration in function over time, the degree of sialorrhea will increase as the child ages.
Sometimes, if the child’s underlying condition leads to a deterioration in function over time, the degree of sialorrhea will increase as the child ages.
What are the Symptoms of Excessive Drooling?
Anterior sialorrhea is easy to identify as the drooling is readily visible. Often there is constant drooling with resultant chronic wet clothing or bibs. Sometimes the drooling is worse at night with wet bedding every morning. Posterior sialorrhea can be more difficult to appreciate but may need to be considered if the child is constantly visibly choking and coughing or seems to be prone to repeated episodes of aspiration pneumonia.
How is Excessive Drooling Diagnosed?
Anterior sialorrhea is diagnosed by the family or their caregivers via the observation of excessive drooling. Posterior sialorrhea can be suggested by the history of choking and repeated pneumonias. Occasionally, additional tests can be helpful including swallowing evaluations done jointly between the Speech Pathologists and Radiologists where the child is examined with x-ray imaging during the act of swallowing.
How is Excessive Drooling Traditionally Treated?
Treatment options center around medical and surgical therapies to diminish the amount of saliva present in the mouth. Approximately 1 liter of saliva is produced each day primarily by three salivary glands on either side of the mouth: the parotid glands, the submandibular glands, and the sublingual glands.
Traditional treatment options include daily oral medications to diminish saliva production, periodic injections of a medication called Botox for temporary reduction in saliva production, or a variety of open surgical procedures to remove some salivary glands or disconnect others from the mouth.
How is Excessive Drooling Treated at Nationwide Children’s?
In order to effectively treat this problem and diminish the invasiveness of operative interventions, Interventional Radiologists at Nationwide Children’s Hospital, developed an alternative percutaneous procedure called Salivary Gland Ablation around 2004.
Instead of operatively removing salivary glands, we inject them with medications such as alcohol in order to shrink them and decrease saliva production. No incisions are made. Some injections are delivered through the normal salivary gland drainage tubes (parotid ducts), while other injections are delivered through the skin directly into the sublingual and submandibular glands. In all cases, image guidance is employed for accurate placement of the medications. After injection the glands decrease in size and produce less saliva.
All injections are performed under anesthesia. In most cases all the glands on one side of the face are injected in a single procedure. At follow-up appointments, if the problem persists, injection of the other side can be considered.
What are the Risks and Potential Complications of this Procedure?
Salivary Gland Ablations have been safely performed at Nationwide Children’s Hospital since around 2004. The aim of the procedure is to diminish the patients’ dependence upon daily medications and to permanently decrease the amount of saliva production without open surgical procedures. While there are no incisions or stiches and therefore no post-treatment wound care, Salivary Gland Ablation does result in significant, usually painless, facial swelling for several weeks after injection.
While there are no incisions or stiches and therefore no post-treatment wound care, Salivary Gland Ablation does result in significant, usually painless, facial swelling for several weeks after injection.
While our percutaneous procedure is very safe, all treatments carry risks. The primary serious risk that can occur with alcohol injection of salivary glands is injury to a nearby nerves which can result in temporary facial muscle weakness in rare cases (2-3%). As the glands are not physically removed with salivary gland ablation, after injection they continue with some saliva production and to date no child has suffered from an overly dry mouth.
Can Excessive Drooling be Cured?
Sialorrhea is a chronic condition that sometimes be can be managed with conservative measures such as attention to oral hygiene and skin care together with therapy to maximize swallowing function. If symptoms remain severe enough then daily medications can be added to decrease saliva production though these medications can have unwanted side effects. Beyond that, salivary gland ablation or operative interventions may be considered.
Beyond that, salivary gland ablation or operative interventions may be considered.
Sialorrhea can rarely be completely eliminated with any strategy and all treatments are designed to decrease symptoms without overly limiting salivary production. As this is a benign condition, treatment options also are chosen to minimize risk to the patient undergoing those procedures.
When Should we See a Doctor?
If a child’s symptoms are felt to be severe enough by his or her physicians salivary gland ablation can be considered to further diminish saliva production.
You Might Also Be Interested In
Article
Salivary Gland Ablation
Prior to advancements at Nationwide Children’s Hospital, there were no successful interventional radiological (minimally invasive) therapies for ranulas and sialorrhea. The need for salivary gland ablation treatment was recognized, so our interventional radiologists developed a new procedure.
The need for salivary gland ablation treatment was recognized, so our interventional radiologists developed a new procedure.
Blog
Sclerotherapy: Using Minimally Invasive Technology to Treat Disease
Parents are understandably nervous when they learn their child has been diagnosed with a swelling or growth. Fortunately, many times the growth is not a cancerous life threatening tumor, but is instead a benign collection of abnormal blood vessels or fluid that is swelling and causing pain and
Scientific Publication
Salivary gland ablation: introducing an interventional radiology treatment alternative in the management of sialorrhea
What to Know About Excessive Drooling in Children
Written by Sonia Findlay
In this Article
- What Is Sialorrhea?
- What Are the Causes of Sialorrhea?
- What Are the Symptoms of Sialorrhea?
- How Is Sialorrhea Diagnosed?
- How Is Sialorrhea Treated?
- When Should You Be Worried About Drooling?
Drooling is common in children between the ages of 15 and 19 months. But after the age of 4, excessive drooling can point to an underlying condition. Sialorrhea, also known as hypersalivation, is usually present in children with neurological or anatomical abnormalities. If you’re worried your child has sialorrhea, here’s what you need to know about the causes, symptoms, and treatments.
But after the age of 4, excessive drooling can point to an underlying condition. Sialorrhea, also known as hypersalivation, is usually present in children with neurological or anatomical abnormalities. If you’re worried your child has sialorrhea, here’s what you need to know about the causes, symptoms, and treatments.
What Is Sialorrhea?
Sialorrhea is excessive oral secretion, or drooling. Children usually produce up to 1.5 liters of saliva per day, but children with hypersalivation may produce up to 5 liters. This condition may also happen in children who produce an average amount of saliva but can’t swallow properly.
There are two types of sialorrhea:
Anterior sialorrhea. Anterior sialorrhea is what is commonly referred to as drooling. The excess saliva spills onto the child’s face and, if left unchecked, their clothes. This can cause issues with skin care and cleanliness. Because of this, they may also have issues with socializing.
Posterior sialorrhea. Posterior sialorrhea is when the saliva spills down the child’s airway instead of being swallowed. This form of hypersalivation leads to chronic lung irritation, which can cause other health issues.
Posterior sialorrhea is when the saliva spills down the child’s airway instead of being swallowed. This form of hypersalivation leads to chronic lung irritation, which can cause other health issues.
Children with sialorrhea typically have a combination of anterior and posterior sialorrhea.
What Are the Causes of Sialorrhea?
Sialorrhea in children is often caused by existing underlying diseases. Conditions that affect the brain can cause reduced muscle control, especially around the mouth and throat. This leads to difficulty swallowing saliva and results in excessive drooling.
Excessive oral secretions are common in children who are born with cerebral palsy, which is a condition that affects the brain’s ability to move muscles. Some studies suggest that up to 58% of children with cerebral palsy also have sialorrhea.
Other conditions that affect motor control of the mouth and throat include stroke, traumatic brain injuries, and abnormalities in brain development. The severity of the sialorrhea normally depends on the severity of the underlying disease. For example, if the brain injury does not worsen over time, the excessive drooling shouldn’t either.
The severity of the sialorrhea normally depends on the severity of the underlying disease. For example, if the brain injury does not worsen over time, the excessive drooling shouldn’t either.
Sialorrhea also happens in children with anatomical abnormalities that lead to physical difficulties swallowing. Hypersalivation causes may include:
- A large tongue
- A malformed jaw
- A malformed throat
- Orthodontic issues
- Clefts in the lip, palate, or larynx
Excessive drooling can also be caused by the child’s body producing too much saliva or mucus rather than their inability to swallow. This can happen as a result of other neurological or respiratory conditions or as a side effect of certain medications.
What Are the Symptoms of Sialorrhea?
Hypersalivation symptoms depend on whether the saliva is being drooled onto the child’s face or spilling into their airway.
Children with anterior sialorrhea have visible drooling that is usually accompanied by wet clothing. If the drooling is severe, the child’s bed sheets may also be wet after sleeping.
If the drooling is severe, the child’s bed sheets may also be wet after sleeping.
Constant drooling can lead to facial rashes and the breakdown of skin around the mouth and chin. This can cause some irritation and soreness.
Children with sialorrhea may also have mild dehydration, difficulties with speech, and feeding issues as a side effect of constant drooling.
Children with posterior sialorrhea may have more serious symptoms due to chronic lung irritation and a blocked airway. Symptoms can include:
- Choking
- Coughing
- Gagging
- Vomiting
- Congestion
- Breathing difficulty
- Aspiration
Aspiration, which is breathing in non-air substances, is especially dangerous as it can lead to pneumonia.
How Is Sialorrhea Diagnosed?
Healthcare professionals can diagnose anterior sialorrhea by observation. Excessive drooling is an easily identifiable, visible symptom. Posterior sialorrhea diagnosis may need additional tests.
To identify posterior sialorrhea, doctors can use special equipment and procedures to examine the child’s throat as well as their swallowing and speech functions. This often involves the use of videofluoroscopy, which is a specific type of x-ray used to assess swallowing.
How Is Sialorrhea Treated?
Sialorrhea treatments include oral medications, botox injections, surgical procedures, and oral motor training.
Oral medications. Doctors may prescribe oral medications to reduce saliva production or ease the child’s airway. The side effects of this medication may be uncomfortable or lead to other health complications. Anticholinergic medications, which are used to ease airways, usually cause dry mouth and constipation.
More serious side effects include fever and thicker secretions, which can cause further respiratory issues. Because of this, medication may only be appropriate for serious cases of hypersalivation in children.
Botox injections. Studies show that botulinum toxin, or botox, can safely treat sialorrhea in children. Doctors can reduce saliva production for around 4 months by injecting botox into the salivary glands.
Studies show that botulinum toxin, or botox, can safely treat sialorrhea in children. Doctors can reduce saliva production for around 4 months by injecting botox into the salivary glands.
Surgical procedures. There are many surgeries for the treatment of sialorrhea. Usually, they involve removing or disconnecting some salivary glands from the child’s mouth. By permanently reducing saliva production, some surgeries can curatively treat excessive drooling.
Oral motor training. Children who drool due to physical malformations should consider doing oral motor training, such as speech or swallowing therapy, if they can. This can help them learn how to swallow properly and reduce the amount of excess drool.
Mild cases of sialorrhea may not need aggressive treatment. You can manage drooling by using bibs or other cloths to absorb excess oral secretion. Additionally, you can use barrier creams around the mouth and chin to help prevent skin irritation.
When Should You Be Worried About Drooling?
Drooling often happens in young children who haven’t yet developed the proper motor control or awareness to swallow their saliva. But, by the age of four, children should be able to control their drooling habits. After this age, excessive drooling may be a sign of an underlying condition. If you’re unaware that your child has any existing conditions, you should seek additional advice from your doctor.
Excessive drooling usually doesn’t cause serious medical problems, especially if it’s anterior sialorrhea. But if sialorrhea has started to affect your child’s quality of life, it may be worthwhile to seek more advanced treatment from your doctor.
You should also keep in mind that if the onset of sialorrhea is sudden, excessive drooling may be a sign of a throat infection or that your child has swallowed an object.
In all cases, it’s important to take your child to a doctor to get the correct diagnosis and treatment.
Drooling: Causes and treatments
Drooling is a normal part of life for infants, but it can be a problem for children and adults. A person may drool for a variety of reasons. For example, allergies and certain neurological conditions can cause this symptom.
Some people may find excessive drooling embarrassing. However, it should not be a cause of embarrassment.
In some cases, excess saliva production can cause swallowing issues and other problems. Doctors may refer to excess drooling as sialorrhea or ptyalism.
This article will examine the potential causes of drooling and the treatments available to manage this symptom.
Share on PinterestAlthough drooling is common among infants, some adults may also drool — especially in their sleep.
Drooling occurs when saliva pools outside the mouth involuntarily. It can happen when the muscles around the mouth are weak or underdeveloped.
It can also occur if a person produces too much saliva or has difficulty swallowing.
The salivary glands create saliva. Saliva helps with:
- digestion
- swallowing
- oral health
- speech
There are three pairs of major salivary glands. These are the parotid, submandibular, and sublingual glands. People also have hundreds of minor salivary glands.
Typically, people produce up to 1.5 liters of saliva per day. Sometimes, however, the glands overproduce saliva. This can cause drooling.
In infants, drooling is normal. Infants have weak muscles around the mouth and do not have full control over swallowing. Usually, drooling stops when infants reach the age of around 15–18 months.
Drooling can also occur in people with certain medical or neurological conditions.
Drooling can be the result of a medical condition. It can also be a side effect of certain drugs.
Any disease, condition, or medication that weakens the muscles, causes excess saliva production, or makes it harder to swallow may cause drooling.
The following are some potential causes of drooling.
Age
Infants are prone to drooling because they do not have full control of their mouth muscles until they are a little older. Drooling also happens when infants are teething.
Diet
Consuming acidic foods, such as alcohol and certain fruits, can encourage excess saliva production and lead to drooling.
Allergies
People who have seasonal allergies may experience excess saliva production, which can lead to drooling. Some other symptoms of allergies include:
- itchy eyes
- a runny nose
- sneezing
Medications
Certain medications can cause people to produce more saliva than usual. Potential culprits include medications for:
- psychiatric conditions
- myasthenia gravis
- Alzheimer’s disease
Neurological conditions
Some neurological conditions can also cause drooling. These include conditions that cause muscle weakness, especially in the face.
Some examples of neurological conditions that may impact a person’s ability to swallow or close their mouth include:
- Parkinson’s disease
- amyotrophic lateral sclerosis (ALS)
- cerebral palsy
- stroke
Other conditions
Other conditions that cause excess saliva production or difficulty swallowing may also lead to drooling. Some examples of such conditions include:
- acid reflux
- infections, such as tonsillitis, strep throat, or sinusitis
- anatomical irregularities in the head and neck
- sleep apnea
Pregnancy is another factor that may lead to drooling.
Sometimes, drooling requires no treatment. In infants, for example, people consider drooling to be normal.
Doctors will recommend treatment if the drooling is severe, interrupts daily activities, or causes embarrassment.
In some cases, severe drooling can also give rise to respiratory infections if the person inhales the excess saliva.
Excess drooling can also cause skin irritation, such as drool rash, as people frequently wipe the saliva from around their mouths.
Some ways that people can manage excess saliva production include:
- sucking on hard candies
- chewing gum
- wearing a wristband to discreetly wipe the mouth
Treatment varies depending on the severity of a person’s drooling and what is causing it. Options include the following:
Therapy
Certain kinds of therapy can help treat excess drooling.
For example, swallowing therapy can help people with swallowing problems by teaching them exercises to strengthen their mouth and throat muscles.
Healthcare professionals can also help people learn eating and drinking techniques that can help limit drooling.
Likewise, speech therapy can help with tongue mobility and improve lip position and closure during swallowing.
Dental or oral devices
Oral devices may help with drooling. These help ensure proper positioning of the jaw, lips, and tongue to limit drooling.
These help ensure proper positioning of the jaw, lips, and tongue to limit drooling.
However, they are not very comfortable. They are also not suitable for people who have difficulty breathing through their nose or individuals with seizure disorders.
Botox injections
Healthcare professionals can inject Botox into the salivary glands to reduce saliva production.
Usually, this treatment does not have significant side effects. It does not always work, but when it does, it may reduce drooling for a few months.
Injections are usually into the parotid glands via the cheek.
Medications
In people whose drooling is the result of allergies, taking allergy medication can help limit excess saliva production.
Doctors may also prescribe particular saliva curbing medications to people with neurological conditions.
Anticholinergic drugs can help control saliva production. Anticholinergic drugs are not the top treatment choice, however, because many have adverse side effects.
The potential side effects of these drugs include:
- dry mouth
- vomiting
- drowsiness
- dizziness
- vision issues
- constipation
- headaches
If medication is causing or exacerbating drooling, a person can speak to their doctor to find a different treatment option.
Surgery
A doctor will only recommend surgery if the drooling is excessive, leads to respiratory infections, and does not respond to other treatment options.
Drooling is fairly common and is not usually a cause for concern.
However, if excessive drooling is persistent, severe, interrupts daily activities, or causes embarrassment, it may be worth seeking medical advice to help manage this symptom.
Drooling is a common symptom of many medical and neurological conditions. It may seem like a minor problem, but it can severely impact a person’s quality of life.
Drooling can cause skin problems and respiratory infections. It also has the potential to harm a person’s self-esteem and social life.
Although chronic drooling can be difficult to control, there are several ways to manage excess drooling, including therapy, oral devices, medications, and, in severe cases, surgery.
Autism and drooling: Why so common? What helps?
Our 3-year-old was recently diagnosed with autism. He has made progress and is now talking, requesting and labeling. But he drools all the time, and we have to wipe his face constantly. How can we help him not drool?
Today’s “Got Questions?” answer is by behavior analyst Kara Reagon, Autism Speaks associate director for dissemination science.
Editor’s note: The following information is not meant to diagnose or treat and should not take the place of personal consultation, as appropriate, with a qualified healthcare professional.
Everybody drools – at least to start. Typically developing infants start to gain control of their swallowing and mouth muscles between 18 and 24 months of age. But it’s common for children with developmental disorders to drool excessively and for longer than is typical with other children. This includes children with autism, many of whom have delays and difficulties with muscle control and sensitivity.
But it’s common for children with developmental disorders to drool excessively and for longer than is typical with other children. This includes children with autism, many of whom have delays and difficulties with muscle control and sensitivity.
What causes excessive drooling?
Typically, drooling involves low muscle tone, a lack of sensitivity around the lips and face, difficulty swallowing and/or excessive production of saliva. A variety of neurological and attention deficits can contribute to these issues – as is often the case among children – and sometimes adults – who have autism.
You are right to be concerned. Drooling becomes socially stigmatizing when it continues beyond infancy. It’s also unhygienic – an important issue as your son enters group settings such as preschool.
That said, drooling in some situations – for instance, while sleeping – is generally harmless unless it’s so excessive that your child is inhaling saliva.
So let’s focus on your son’s tendency to drool during the day.
Evaluation and treatment options
First, it’s important to discuss your son’s drooling with his pediatrician or a pediatric ear-nose-throat specialist to address or rule out serious underlying medical conditions. This will likely involve an examination of his tonsils, sinuses, and salivary glands. Also, certain medications can worsen drooling – another issue to discuss with your son’s doctor. In addition, the doctor should evaluate whether your son’s drooling is resulting in his inhaling saliva into his lungs – putting him at risk for pneumonia.
Treatment options should be tailored to your son’s needs and may require further evaluation – for instance by a speech-language pathologist or occupational therapist experienced in oral-sensitivity and muscle tone issues.
Speech and occupational therapists can help your son improve his oral muscle tone, lip closure and swallowing. In some cases, the therapist may suggest a dental appliance or chin cup to assist in lip closure, tongue positioning and swallowing.
It may also help to reduce the amount of acidic foods your son is eating – as they can trigger the production of excessive saliva. But it’s important to work with a dietician before introducing any significant change to your son’s diet – particularly if he’s already a picky eater.
The goals of therapy
Generally drooling can be addressed through occupational and/or speech therapy that focuses on the following:
1. Develop good posture and positioning
Sometimes, poor muscle control of the trunk, neck and head results in the head tilting downward. In this position, saliva tends to pool at the front of the mouth and spill from parted lips. The therapist can help you position your child in ways that encourage proper trunk control and head support.
2. Build oral muscle strength and control.
Therapists use a variety of playful oral-motor exercises to help children build muscle tone around the mouth. For instance, the therapist may have your son practice closing his lips around a straw, spoon or a piece of food and/or practice pronouncing closed-lip speech sounds such as “p,” “b” and “m.” The therapist will show you how to continue these exercises at home, with lots of encouragement in the form of praise and/or small rewards.
For instance, the therapist may have your son practice closing his lips around a straw, spoon or a piece of food and/or practice pronouncing closed-lip speech sounds such as “p,” “b” and “m.” The therapist will show you how to continue these exercises at home, with lots of encouragement in the form of praise and/or small rewards.
3. Increase oral sensitivity. Similarly, therapists have a variety of tactile exercises that can help your child develop sensitivity in the lips, tongue, mouth and chin. This includes building awareness of dryness versus wetness – so your child becomes aware when he’s drooling. Playful oral-sensitivity exercises can include blowing bubbles, making exaggerated sounds involving the lips such as “oooo,” “eeee” and “puh-puh-puh.” Again the therapist will give you guidance on how to practice these exercises at home.
4. Practice proper chewing and swallowing. Does your child drool excessively while eating? If so, you and the therapist can work with your child to master the steps of proper chewing and swallowing. It’s helpful to practice these exercises when your child is hungry enough to enjoy a snack but not ravenous. In general, the therapist will show you how to model, or exaggerate, appropriate chewing motions (closing the teeth and then the lips, etc.) and encourage your child to do the same. It can help to give your son a hand-held mirror so he can watch himself perform these steps. As always, remember to encourage and praise, as in:
It’s helpful to practice these exercises when your child is hungry enough to enjoy a snack but not ravenous. In general, the therapist will show you how to model, or exaggerate, appropriate chewing motions (closing the teeth and then the lips, etc.) and encourage your child to do the same. It can help to give your son a hand-held mirror so he can watch himself perform these steps. As always, remember to encourage and praise, as in:
“That’s great. You’re chewing your cracker. Awesome, you swallowed the cracker! Good eating.”
5. Practice wiping with a napkin or handkerchief. While your child is learning to become aware of wetness on his face, it’s important to encourage the socially appropriate practice of wiping with a napkin or handkerchief. For mealtimes, I suggest teaching him the habit of “wipe, wipe, swallow” – wiping one side of the mouth and then the other before swallowing. Consider attaching the napkin to a wristband during meals to encourage this habit.
You mention that your son drools continuously. So you’ll also want to teach him the habit of wiping with a handkerchief when not at the dinner table. This includes helping him learn to keep a clean handkerchief handy in a pocket. Another option is have your son wear wrist sweatbands and encourage him to use them to wipe each side of his face regularly.
Both at the dinner table and away, you’ll want to cue your child – perhaps by properly wiping your own mouth – when you see him drooling.
6. Put it all together with rewards.
Be sure to create a reward system to reinforce each step your child takes with chewing, swallowing, wiping and most importantly keeping a clean, dry face. At age 3, you may want to keep this simple – with lots of praise and small rewards. But your son may be old enough to enjoy a token system that involves earning larger rewards such as a favorite activity with you.
One of my favorite resources is How to Stop Drooling, by speech-language pathologist Pam Marshalla.
Got more questions for our behavioral and medical experts? Send them to [email protected].
Your Baby at 2 Months | Patient Education
Patient Education A-Z
At 2 months, most babies are beginning to cry less and spend more time awake. They are interested in what’s going on around them. Babies enjoy looking at faces, seeing you smile and hearing your voice. They are learning language now, so talk and sing to your baby.
Development
Talk to your baby in long sentences so he or she can hear and learn the grammar of your language. Also spend time making baby sounds, like “ba ba ba,” to encourage language development. Pause and allow your baby time to respond. Your baby will also try to copy funny faces that you make.
If your baby will hear more than one language at home, begin exposing him or her to both languages now. It is much easier for children to speak more than one language if they’ve heard both languages from infancy. Hearing more than one language will not confuse your baby, but consider having one person speak one language to your baby, and another person speak the second language.
Hearing more than one language will not confuse your baby, but consider having one person speak one language to your baby, and another person speak the second language.
Parents often wonder what toys are best for babies. At around 2 months babies are learning to use their neck and shoulder muscles. They soon will begin trying to raise their heads when lying down and to reach out for objects when sitting. You can hold toys out in front of your baby to encourage him or her to reach. Babies love brightly colored objects, and mobiles will attract their attention. You can also introduce a soft rattle.
Here are a few safety tips to remember when choosing toys for your baby:
- Never give your baby a toy with sharp or pointed edges.
- Don’t let your baby hold a toy with small removable parts that could cause choking.
- Choose toys made for your baby’s age.
In addition to learning how to reach for objects, babies this age are able to put their hands in their mouths. It’s normal for babies to put objects in their mouths — it is their way of exploring and learning about their world. To keep your baby safe, be careful what objects are left within reach.
It’s normal for babies to put objects in their mouths — it is their way of exploring and learning about their world. To keep your baby safe, be careful what objects are left within reach.
Soon your baby’s salivary glands will start to work and your baby will begin to drool. This does not mean that your baby is teething.
At this age babies often like to “stand up” while held and bear weight. It is fine to allow your baby to do this. To help your baby’s development, allow your baby to spend time in various positions — sitting, standing while held, and lying on his or her back or tummy. Just remember, babies should always be placed on their backs to go to sleep.
Remember that babies develop differently and on their own schedules. Because babies are sleeping on their backs these days, some do not like to roll over. This doesn’t mean the baby has a problem. Later on, some babies will also skip the crawling phase.
Sleeping
There are many different ideas about where babies should sleep. Some people believe it is important for babies to sleep with their parents, while others believe babies should sleep by themselves. We believe it is most important that the parents decide what is right for their babies. Take a moment to talk with any adults who live at home with you to decide where you feel comfortable having the baby sleep.
Some people believe it is important for babies to sleep with their parents, while others believe babies should sleep by themselves. We believe it is most important that the parents decide what is right for their babies. Take a moment to talk with any adults who live at home with you to decide where you feel comfortable having the baby sleep.
Remember that sleep patterns or habits are formed by 6 months of age. Here are some things you can do now to prevent sleep problems in the future:
- Try not to feed your baby more frequently than every two hours during the day. Babies who eat frequently during the day will normally wake up to eat frequently at night.
- Try to put your baby to bed at the same time each night.
- Try to avoid waking your baby at night — don’t turn on the light or talk to your baby at night. This helps your baby realize that nighttime is not a very interesting time to be awake.
- Try to delay or shorten middle-of-the-night feedings. If you are breast-feeding, try nursing from just one side.
 If you are bottle-feeding, do not make your baby finish the bottle. This teaches babies that they don’t need a full tummy to fall asleep.
If you are bottle-feeding, do not make your baby finish the bottle. This teaches babies that they don’t need a full tummy to fall asleep. - Try not to change your baby’s diaper at night, unless your baby has a diaper rash. You can use extra diaper liners if necessary.
- If possible, put your baby to bed slightly drowsy but still awake. Your baby may be restless and cry a little before falling asleep, but it is helpful for babies to learn that they can calm down and fall asleep on their own.
- Consider beginning a bedtime routine to help your baby learn the difference between daytime sleep and nighttime sleep. Try to do the same steps every night at about the same time. A soft song, a gentle massage and warm bath — these can all help signal to your baby that nighttime is coming.
- Young babies need to be encouraged or allowed to fall asleep after about one hour of being awake. If your baby has been awake for one hour, watch for clues that he or she is sleepy — yawning, rubbing eyes, looking away from you or acting fussy. Many parents misinterpret these signs, believing their baby is bored and needs more stimulation; it is more likely that the baby needs to be allowed to fall asleep.
 If you are bottle-feeding, do not make your baby finish the bottle. This teaches babies that they don’t need a full tummy to fall asleep.
If you are bottle-feeding, do not make your baby finish the bottle. This teaches babies that they don’t need a full tummy to fall asleep. Many parents misinterpret these signs, believing their baby is bored and needs more stimulation; it is more likely that the baby needs to be allowed to fall asleep.
Many parents misinterpret these signs, believing their baby is bored and needs more stimulation; it is more likely that the baby needs to be allowed to fall asleep.One baby book author advocates the “E-A-S-Y” plan to help babies nap better:
- E — Eating: The baby is fed after waking up from nighttime sleep or a nap.
- A — Activity: After feeding, the baby has time for activities and being awake.
- S — Sleep: After 30 to 45 minutes of awake time, the baby is placed down for sleep. This helps prevent the baby from forming an association between feeding and falling asleep.
- Y — You: This is “you time.”
Flat Heads
For safety reasons babies should always sleep on their backs. Sometimes this causes their heads to become flattened in the back, usually on the right side. To help prevent this, encourage your baby to look to the left and let him or her spend more time sitting up. You you can also give your baby “tummy time” when he or she is awake and supervised. Tummy time helps babies learn how to use their neck and shoulder muscles.
You you can also give your baby “tummy time” when he or she is awake and supervised. Tummy time helps babies learn how to use their neck and shoulder muscles.
Feeding
Your baby will continue to grow well on breast milk or formula for the next four months. Although you may be tempted to try giving your baby solid foods early, there are a number of reasons not to start solid foods, including baby cereal, until about 6 months of age. Some of these reasons include:
- Babies’ intestinal tracts are immature. It is easier for them to develop allergies if you offer solid foods too early.
- Babies’ muscles are not able to coordinate sucking and swallowing solid foods yet. When a baby can sit and reach out for objects, he or she will probably be able to use the mouth muscles to swallow solids as well.
- When babies are given solid foods too early, they don’t get all the nutrition they need from breast milk or formula, which is specially designed to meet babies’ needs.

Safety
A few extremely important safety tips:
- Remember to always place your baby on his or her back to sleep.
- Always secure your baby in a car seat when traveling by car or taxi. The car seat should still face backward in the car. Do not place the car seat in a seat equipped with airbags. Parents, remember that you need to buckle up too, and make sure that you never drink alcohol and drive.
- Do not leave your baby alone in a high place such as a changing table — your baby is beginning to scoot and roll, and can quickly fall off.
- Do not drink hot liquids while holding your baby. Your baby will soon begin reaching for objects and may make you spill the liquid, burning both of you.
- Do not allow anyone to smoke in your home. If you or someone in your home must smoke, please go outside so your baby will not be exposed to the smoke. Wear a special covering or jacket while you are smoking outdoors and take it off before coming back inside. This will prevent the smoke particles from attaching to your clothing and affecting your baby. Never hold a cigarette when you are holding your baby.
- Never shake your baby — it can cause serious injuries.
 This will prevent the smoke particles from attaching to your clothing and affecting your baby. Never hold a cigarette when you are holding your baby.
This will prevent the smoke particles from attaching to your clothing and affecting your baby. Never hold a cigarette when you are holding your baby.Used by permission of Jane E. Anderson, M.D.
UCSF Benioff Children’s Hospitals medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your child’s doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your child’s provider.
Recommended reading
Your Baby at 1 Week
Your 1-week-old baby enjoys looking at your face and hearing your voice. Learn more about developmental milestones, sleep safety and parenting tips.
Your Baby at 2 Weeks
Your 2-week-old baby already has a unique personality. Read about developmental milestones and tips for feeding, sleeping and safety, including car seats.
Your Baby at 1 Month
Your 1-month-old baby is beginning to smile, make sounds and raise their head. Learn more about milestones for feeding, development and health.
Your Baby at 4 Months
Your 4-month-old baby might enjoy laughing more than eating. Read about developmental milestones, such as teething, and get tips for feeding and sleeping.
Your Baby at 6 Months
Your 6-month-old baby may be sleeping 6 to 8 hours at night. Read about developmental milestones, such as teething, and get tips for feeding and sleeping.
Your Baby at 9 Months
At 9 months old, your baby may be learning to pull up to stand. Read about safety tips and developmental milestones in feeding, sleeping and language.
Your Baby at 12 Months
Your 12-month-old baby is becoming an independent eater. Learn about developmental milestones and tips for feeding, dental care and car and water safety.
Breast Milk or Formula?
Breast milk and infant formula benefit your baby in different ways. Read our tips to help feeding time go smoothly and ensure your child is well nourished.
Read our tips to help feeding time go smoothly and ensure your child is well nourished.
Breastfeeding and Returning to Work
If you are breastfeeding and returning to work, read our tips to ensure a smooth transition for you and your baby.
Siblings and a New Baby
Bringing a new baby into your family can be difficult for their siblings. Find out how to support your older children through this transition.
Soothing Your Crying Infant
Babies cry for several reasons, and there are many ways you can soothe them. Read our recommendations and what you can do if your baby continues crying.
Recommended Vaccines for Your Child
Experts recommend that children receive vaccinations (shots) to protect them from 13 serious illnesses. Find out which ones and how often shots are needed.
Related clinics (1)
10
San Francisco / Oakland / San Mateo / San Rafael / Sonoma / Novato
Tender wagging care
Our therapy dogs spread joy and smiles at the bedside and throughout the hospital.

Visit Child Life services
Excess Saliva Can Signal Health Conditions that Cause Speech Development Delays
by Chris O
Sometimes something that sounds so innocent can be a symptom of a larger issue. Drooling in infants and toddlers is often associated with teething, but can also be the sign of a larger health problem that can affect your child’s speech development.
Drooling and Teething – A Normal Process
When your baby begins to teethe, often around 6 months of age, you will likely see an increase in drool. There are no front lower teeth to hold back the saliva stream, and the body naturally increases saliva in a baby’s mouth to prepare for the healthy eruption of teeth. Saliva has mild antibacterial properties that help to keep your baby’s mouth healthier, and as more teeth erupt the levels of saliva can be expected to increase.
Drooling and Muscle Tone Issues – What Are the Causes?
While drooling for most babies and toddlers is part of a natural process, sometimes either excessive drooling or drooling beyond teething can signal a bigger issue. Researchers have developed four theories as to why drooling might be the sign of something more than teething.
Researchers have developed four theories as to why drooling might be the sign of something more than teething.
1. Some children are not aware that they are drooling.
2. Some children do not swallow frequently, or at least enough to be rid of the excess saliva.
3. Some children do not swallow completely, leaving some saliva in the mouth each time.
4. Some children do not seal their lips when trying to swallow their saliva.
It might be hard to imagine not being aware of excessive drooling, or difficult to even try to swallow with your mouth open, but for kids who have decreased muscle tone around the mouth and other problems this is their reality. There are several underlying reasons why a child might have excessive drooling connected to any of these four above theories:
- Hypotonia is a condition where a person has decreased muscle tone, including those responsible for swallowing and speaking.
- Cerebral palsy is a condition that encompasses many levels of brain developmental problems, most noticeably affecting a child’s motor abilities.
- Down syndrome is a condition that affects both the mental and physical development of a person, and which can contribute to drooling.
- Childhood apraxia of speech is a neurological condition that affects the communication between the brain (what it wants to say) and the mouth muscles (that are supposed to help form the words)

Kids develop at different rates with different levels of efficiency, and sometimes facial and neck muscles are not as strong as typically found at certain ages or there is a lack of coordination between the muscle groups responsible for stopping drooling. This can happen without a major health condition as a cause. Drooling caused by teething typically subsides by around ages 2-3 years. If your child is an older toddler and still excessively drooling without any other known health issues, it might be time to take a closer look.
Drooling – Why Should I Care and What Can I Do?
Excessive drooling can not only be messy, but it can lead to social problems as well, especially in individuals who don’t have visibly noticeable health conditions. Drooling can also signal a problem with muscle tone and coordination, for whatever underlying reason, that will contribute to speech and communication delays. If your child’s mouth isn’t working properly to prevent excessive drooling, articulation and other speech milestones might be negatively affected. It can also be a sign of feeding problems that can lead to nutritional deficits. There are several things you can do to try to minimize the drooling and improve the muscle tone needed for proper speech development.
Drooling can also signal a problem with muscle tone and coordination, for whatever underlying reason, that will contribute to speech and communication delays. If your child’s mouth isn’t working properly to prevent excessive drooling, articulation and other speech milestones might be negatively affected. It can also be a sign of feeding problems that can lead to nutritional deficits. There are several things you can do to try to minimize the drooling and improve the muscle tone needed for proper speech development.
- Work with your child’s doctor to determine if there is an underlying health problem related to the drooling.
- Work with an SLP and physical therapist to develop and use exercises that will improve swallowing.
- Skip the sippy cup and teach your child to use a straw. Straws help encourage children to purse their lips together and use the muscles needed for swallowing. As a company of parents, Speech Buddies recommends the OXO Tot Transitions Straw Cup or Thinkbaby Thinkster Straw Bottle. For a stainless steel option, we love the THERMOS Straw Bottle.
- Skip the sugary drinks. They are harmful to your child’s oral health, can increase the odds of obesity, and can promote a thicker saliva that is harder to clear from the mouth during swallowing.
 For a stainless steel option, we love the THERMOS Straw Bottle.
For a stainless steel option, we love the THERMOS Straw Bottle.Some of the links provided on Speech Buddies are affiliate links. We receive a small commission on sales made through these links. We only endorse products that we love.
Language DevelopmentSpeech Therapy Techniques
Tagged: drooling, muscle coordination, muscle tone, speech delays
Causes and treatments for increased salivation
06/15/2018
Increased salivation in an adult is a symptom of inflammation or disease of the gums, teeth or internal organs. It is important not only to eliminate profuse salivation, but also to correctly determine its cause, otherwise recovery will be temporary.
Salivation is considered normal if the volume of saliva does not exceed two liters per day. It is involved in digestion, washes away pieces of food, remnants of drinks and the vital activity of bacteria from the teeth. Normally, the process of saliva secretion is imperceptible to a person – we do not pay attention to it, like, for example, to breathing. But if a failure occurs, then too much saliva causes discomfort.
With this ailment, saliva accumulates in the mouth too quickly, you constantly have to make sure that it does not leak out, spit. It is uncomfortable, unaesthetic, spoils the mood and causes discomfort. In the article we tell what are the causes of increased salivation in men, women and how to treat it.
How to understand that salivation is increased: symptoms and signs of failure
Saliva is involved in many important processes that occur in the human body. When everything is normal, we do not notice that saliva:
● helps to clearly and correctly pronounce words and sounds;
● enhances the perception of the taste of food and drinks;
● is involved in digestion – helps to chew food and swallow it.
When salivation is increased, several processes are disrupted at once:
● the taste of food changes – salty food becomes too pronounced, and subtle shades are not felt;
● problems with diction appear – it is problematic to pronounce some sounds;
● It becomes painful to swallow food.
Location of the glands
In addition to indirect signs, there are clear, measurable criteria. If more than two milliliters of saliva is secreted within five minutes, then the patient is diagnosed with increased salivation. The normal value is 2 ml.
Sometimes patients complain of false profuse salivation. This happens when there is injury or inflammation in the mouth and it may seem that there is more saliva than it should be, although the indicators are normal: 2 ml in 5 minutes or 2 liters per day.
Causes of increased salivation in men and women
The volume of saliva secreted is controlled by the nervous system.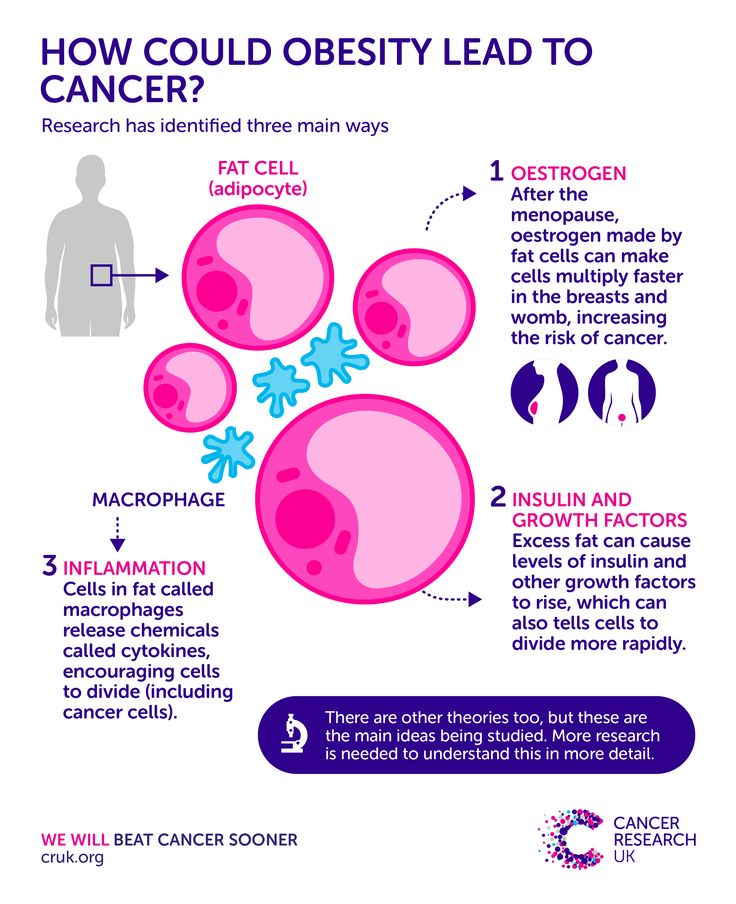 When everything is in order with health, it happens naturally and imperceptibly for a person. But when problems arise or diseases appear, the process is disrupted. A variety of factors can affect, but most often the cause of increased salivation in adult men and women is one of six factors.
When everything is in order with health, it happens naturally and imperceptibly for a person. But when problems arise or diseases appear, the process is disrupted. A variety of factors can affect, but most often the cause of increased salivation in adult men and women is one of six factors.
- Diseases of the oral cavity – inflammation of the gums, periodontitis, stomatitis, as well as cuts, burns. When bacteria enter the tubules of the glands, the body begins to secrete more saliva to get rid of them. This is a natural reaction.
- Problems of the digestive system – abnormal acidity of the stomach, diseases of the pancreas and liver.
- CNS diseases – Parkinson’s disease, trigeminal nerve injury, bulbar syndrome, migraine. With these diseases, the natural process of salivation is disrupted. Short-term disturbance may occur due to air sickness, seasickness, problems with the vestibular apparatus.
- Hormones – failures of the hormonal system, in particular the thyroid gland, menopause, diabetes mellitus lead to excessive salivation. Sometimes this is observed in adolescents during the restructuring of the body.
- Smoking, removable dentures may also be affected. Both of these phenomena irritate the mucous membrane, stimulating the hyperactive work of the glands.
- Taking medications – some medications have among the side effects increased salivation or, as it is also called, hypersalivation. Most often, these are those drugs that contain iodine or mercury. For example: lithium, physostigmine, muscarine.
 Sometimes this is observed in adolescents during the restructuring of the body.
Sometimes this is observed in adolescents during the restructuring of the body. Pilocarpine, nitrazepam also cause gland hyperactivity
What to do with increased salivation depends on the factors that caused it. In some cases, for example, when taking medication, the disease will pass without the intervention of a doctor.
Increased salivation in women during pregnancy
A common cause of hypersalivation in women is pregnancy. When a woman is preparing to become a mother, the hormonal background of the body changes greatly, and with it many processes: blood circulation, digestion.
Pregnancy affects all systems at once:
● endocrine;
● nervous;
● digestive.
It is not uncommon for expectant mothers to have problems with their teeth and gums, such as gingivitis. This disease also affects the amount of saliva produced.
Healthy and inflamed gums
Causes of nighttime increased salivation in adults
During sleep, the processes in the body are slower, including salivation. But crashes can happen. Here are the main factors leading to excessive saliva during sleep:
● breathing through the mouth rather than through the nose – often happens when a person sleeps on their back;
● malocclusion – the mouth remains open during sleep, the tongue dries up and the body decides that more saliva is needed;
● poor sleep – too much sleep, when a person is not sure that he is sleeping. This can lead to the fact that the body considers a dream to be reality and will salivate like during the day.
This is what an open bite looks like – the tongue protrudes forward
Treatment of increased salivation
Depending on the cause of hypersalivation, different doctors are involved in the treatment:
● dentists solve problems of local diseases of the oral cavity;
● endocrinologists for hormonal disorders;
● gastroenterologists, if the case is in diseases of the digestive system;
● neurologists, if the failure is due to problems with the CNS.
The dentist will help identify the cause, and the therapist will refer you to a specific specialist
Medication treatment
In addition to addressing the causes of internal organ dysfunction, your doctor may prescribe medications to relieve symptoms. For example:
● riabal;
Scopolamine;
● platyfillin.
It is forbidden to drink medicine without a doctor’s prescription!
We do not recommend buying and taking medicines without consulting a doctor. Each drug has contraindications and side effects: from glaucoma to diseases of the liver, heart, blood vessels.
Each drug has contraindications and side effects: from glaucoma to diseases of the liver, heart, blood vessels.
It is not worth risking your life and health to save time or money on a visit to the clinic.
Botox treatment
Botox injections are sometimes used for short-term relief of symptoms. It blocks nerve signals, reducing the activity of the tubules. This method helps to quickly get rid of the problem, but, unfortunately, the effect does not last long.
Facial massage and muscle relaxation
Will help if the cause is related to nervous tension, stress or CNS pathologies.
Removal of glands
It is prescribed extremely rarely, only in cases where all other methods and elimination of the causes of the disease have not helped. Removal, even partial, can damage the facial nerves.
Traditional remedies
Traditional remedies can be used to relieve symptoms. Especially if salivation appeared due to sea sickness, air sickness, stress, or while taking medication.
Traditional medicine offers two homemade recipes for rinsing after meals:
● mix one tablespoon of peppercorn tincture with 200-300 ml of warm water;
● Mix black tea with two tablespoons of crushed fresh raspberries, strain and cool.
Diet modification will also help: avoiding potatoes, pasta, bread, pumpkin and other starchy vegetables.
Make an appointment at the SoloDent clinic by phone or through the website. We will determine the cause of increased salivation and help get rid of this unpleasant ailment.
Increased salivation in the mouth: causes, methods of salivation treatment
Author-physician:
Vinogradova Irina Yurievna
Dentist-therapist, endodontist, head of the therapy and periodontology department, member of the medical council of the network of clinics “STOMPRAKTIKA.RF”
Publication date of the article: December 24, 2020
Increased salivation: causes and treatment
Hypersalivation – what is it
Why is there a lot of saliva in the mouth
Salivation during sleep
Excessive salivation during pregnancy
Treatment of hypersalivation
Saliva is not just a liquid secreted in the mouth. Saliva is involved in the process of digestion and protects the body from bacteria. The process of salivation is not controlled by a person. Usually about 2 liters of saliva are produced per day. Under the influence of certain factors, its amount can greatly increase. In the article we will talk about the causes of increased salivation and how to treat it.
Saliva is involved in the process of digestion and protects the body from bacteria. The process of salivation is not controlled by a person. Usually about 2 liters of saliva are produced per day. Under the influence of certain factors, its amount can greatly increase. In the article we will talk about the causes of increased salivation and how to treat it.
Hypersalivation – what is it
Excessive secretion of salivary glands is scientifically called hypersalivation. This phenomenon is often observed in young children, with time it disappears. If this problem appears in adults, then most likely the reason is the malfunction of the internal organs.
Hypersalivation can also be false. This is when fluid builds up in the mouth because it is difficult to swallow.
Why is there a lot of saliva in my mouth?
Consider the possible causes of increased salivation
|
Diseases of the oral cavity. |
|
|
Gastrointestinal diseases (gastritis, pancreatitis, stomach ulcer, etc.). The problem most often occurs against the background of increased acidity of the stomach. Other reasons that doctors single out: abnormalities in the liver, worms, stress on the pancreas. |
|
|
Diseases of the central nervous system (cerebral palsy, Parkinson’s disease, trigeminal nerve irritation, migraine). A similar condition occurs in violation of the vestibular apparatus, increased blood pressure. |
|
|
ENT diseases, SARS, inflammation of the adenoids. A person begins to breathe mainly through the mouth, as nasal breathing is difficult. The mucous membrane dries up, because of this, the glands begin to work actively. |
|
|
Hormonal changes – thyroid problems, diabetes, menopause, etc. Tobacco smoke irritates the salivary glands. They begin to produce a lot of fluid. That is why smokers have a habit of spitting saliva. |
 These include: stomatitis, gingivitis, glossitis, etc. Bacteria provoke irritation of the salivary glands, hence the excessive release of fluid. If these diseases are not treated, then inflammation of the salivary gland may appear. The designs cause irritation of the mucous membrane, which provokes excessive release of fluid. This problem is especially noticeable in the first two weeks after the installation of the structure, when adaptation occurs.
These include: stomatitis, gingivitis, glossitis, etc. Bacteria provoke irritation of the salivary glands, hence the excessive release of fluid. If these diseases are not treated, then inflammation of the salivary gland may appear. The designs cause irritation of the mucous membrane, which provokes excessive release of fluid. This problem is especially noticeable in the first two weeks after the installation of the structure, when adaptation occurs. 
Salivation during sleep
Sometimes, when waking up, a person notices wet spots on the pillow. This usually happens due to extreme fatigue and sound sleep. However, if salivation in a dream becomes a pattern, you should consult a doctor.
The main factors provoking salivation during sleep.
- Incorrect bite or missing teeth. Saliva flows out because the teeth do not close completely.
- Difficulty in nasal breathing: runny nose, deviated nasal septum, colds. All this makes you breathe through your mouth. Since the lips do not close, the accumulated fluid flows out. This is often accompanied by snoring.
- Sound sleep.

Excessive salivation during pregnancy
Hormonal changes occur in the female body during pregnancy. The main reasons why the expectant mother increases salivation.
- Heartburn. When the acid-base balance in the stomach is disturbed, the body begins to produce a lot of saliva. This is a defensive reaction.
- Reaction to medications.
- Toxicosis. To stop vomiting, the expectant mother tries to swallow saliva less often. Therefore, it may seem that there is more saliva in the mouth than usual.
Large salivation does not threaten the fetus, however, if this is a consequence of any disease, then the pregnant woman should control her condition.
What complications are possible?
- Disturbance of taste perception of food.
- Dehydration of the body.
- Insomnia, disturbance of psycho-emotional state.
- Deterioration of the skin on the face and body.
- Infectious diseases.

Treatment of hypersalivation
There is no single treatment for all cases. However, you can use methods to reduce the activity of the salivary glands – sometimes doctors recommend them as an addition to complex therapy.
- Sorbents intake: activated carbon, polysorb, etc.
- Taking medication prescribed by a doctor.
- exercise therapy, massage (more commonly prescribed for children).
- Botulinum toxin injections.
In rare exceptions, the salivary glands are partially removed, but the downside is that there is a risk of damaging the facial nerve.
Which doctors will help to cope with this illness? Dentist, gastroenterologist, endocrinologist, neurologist, infectious disease specialist, etc.
posted on the website as medical advice
Article updated:
December 25, 2020
The child has a fever and profuse salivation.
 Abundant salivation in a child
Abundant salivation in a child
A rare mother does not care about the constantly flowing saliva in a child, and before letting the situation take its course or taking urgent measures, a caring mother will definitely find out why the child is drooling, using authoritative sources on the net or by contacting a pediatrician . Fortunately, most of the existing causes are not pathological and are due to physiological changes in a growing organism.
Before dealing with the root cause, it is worth explaining what this process is. Salivation (ptyalism) or hypersalivation is an increased secretion of the corresponding fluid by the salivary glands, which for one reason or another gets out of the oral cavity and can cause discomfort. The phenomenon can also be observed in adults in some cases, but hypersalivation in a child, especially under the age of 3 years, is most common.
It is important to understand that this is not an independent disease, but simply a phenomenon, which, however, can be a symptom of a certain disease or pathology.
Why is it bad?
The concept of “bad” in this case is somewhat contradictory, since in most cases there is no serious threat to the baby’s health. However, anyone would prefer that such a problem did not exist. Why?
- ✓
Abundant salivation can irritate the skin of the chin and perioral area, the child develops a rash and disturbing irritation.
- ✓
Excess secret falls on clothing and surrounding objects, the child may feel discomfort, just like people nearby.
- ✓
Children over the age of 3 years may experience psychological discomfort from a similar problem. Peers can joke about him, laugh, the child will be embarrassed by salivation, withdraw into himself.
Causes of hypersalivation
Before you speculate, you need to find out for sure whether the child’s salivary glands really work in “enhanced mode” and produce more secretions than they should. It often happens that there is no violation of the secretory function of the salivary glands at all, and the normally produced saliva flows arbitrarily from the child’s mouth only because the child does not swallow it for some reason. In this case, they speak of false hypersalivation. In other cases, a violation can be recognized by the daily amount of secretion produced, which should not exceed the norm of 2.5 (!!!) liters.
In this case, they speak of false hypersalivation. In other cases, a violation can be recognized by the daily amount of secretion produced, which should not exceed the norm of 2.5 (!!!) liters.
However, let’s take a closer look. So, among the causes of increased salivation are the following:
- Physiological phenomenon as a variant of the norm.
Usually, in children under six months, this phenomenon should not be emphasized, since any specialist in the vast majority of cases will say that this is normal. Salivation (ptyalism) occurs at the level of unconditioned reflexes and soon disappears;
Often characterized by a similar symptom, and it can occur long before the appearance of the top of the tooth above the gum. The soft tissues of the gums are injured, the child may feel itching, express concern, try to “scratch” the gums with improvised objects. In response to irritation, the secretory function of the salivary glands also increases;
- Allergic rhinitis in an allergic child
Violation of the act of swallowing may be due to swelling of the nasopharyngeal mucosa, the child constantly breathes through the mouth, which is constantly open. This condition may be the cause of ptyalism;
This condition may be the cause of ptyalism;
- Swallowing problems and jaw anatomy
Drooling is often the cause of a child having difficulty swallowing (or simply forgetting to swallow) or some anatomical features such as malocclusion;
- Oral infections
The body’s natural defense mechanisms are activated by the presence of pathogens in the mouth, nasopharynx and middle ear area. So the baby’s body fights bacteria, literally washing them out with saliva, which also has a weak antiseptic effect;
- gastrointestinal problems
In most cases, diseases of the digestive system are accompanied by this symptom;
- Neurological disorders
If there is a malfunction of the central nervous system, increased salivation may be observed as a symptom, the causes of which lie in a brain tumor, cerebral palsy and other congenital or acquired diseases;
Often characterized by nocturnal salivation;
- Poisoning by heavy metals and hazardous chemicals
May be the underlying cause of this symptom. In this case, salivation is accompanied by a number of other signs;
In this case, salivation is accompanied by a number of other signs;
when taking lithium-containing drugs, ptyalism is noted as a side effect.
{reklama2}
Control and prevention measures
Physiological ptyalism in infants under six months of age and salivation due to teething do not require action. Since this is not a disorder or disease, it is safer to just wait out this period and help the child deal with it.
- ✓
You can offer your child special teethers and rubberized toys specifically for growing teeth.
- ✓
To occupy the child, to stimulate the process of swallowing saliva, offering him a nipple, a nibbler with a treat.
- ✓
Bibs with a waterproof lining will protect your baby’s clothes from getting wet.
- ✓
Regularly remove saliva from the skin, to prevent the occurrence of a pustular rash, treat vulnerable areas with baby cream.
In some cases, it is necessary to get rid of the root cause if the excessive salivation in the child is the result of an allergic reaction or medication. In this case, you should stop taking the medication or get rid of the allergen.
In this case, you should stop taking the medication or get rid of the allergen.
Gymnastics and massage of the facial muscles in some cases is a very effective measure. In addition, an older child who can already chew and take solid food on his own can be offered solid foods, such as apples, carrots, for additional training of the masticatory muscles.
In any case, if you are worried about the unreasonable salivation of your baby, it is better to dispel these concerns with a visit to the doctor.
The specialist will determine the cause of such a phenomenon, if necessary, prescribe additional studies.
Usually severe pathologies and diseases that cause hypersalivation and ptyalism are already known at birth or some time after. For example, salivation in cerebral palsy is a very common occurrence.
If any disease is detected, appropriate treatment is prescribed. Sometimes it is enough to follow a certain diet and periodically rinse the mouth with medicinal solutions, do not neglect cryotherapy. In some cases, surgery may be required to limit the secretory function of the salivary glands or partially remove them.
In some cases, surgery may be required to limit the secretory function of the salivary glands or partially remove them.
Conclusion
The phenomenon of salivation in a child is most common in the first year of a baby’s life, but can be diagnosed at an older age. In the vast majority of cases, the causes of ptyalism are quite harmless: it can be both the inability to voluntarily swallow saliva due to age, and the erupting teeth that disturb the child.
If this phenomenon bothers you, and you want to be sure that everything is fine with the baby, consult a specialist. Only a doctor can determine the true cause of excessive salivation and give appropriate recommendations for hygiene and treatment.
Why does the child drool? This simple but important question worries all mothers without exception. Consider the causes of hypersalivation in infants and possible ways to get rid of this phenomenon.
To answer the question why a child drools and come to a correct solution to this problem, it is necessary to study the properties of saliva and its functions. Saliva is the biological environment of the body, which has a transparent, colorless structure.
Saliva is the biological environment of the body, which has a transparent, colorless structure.
Salivation into the oral cavity is due to the salivary glands. There are several of them in the body: 3 large and many small ones. Main functions of saliva:
- Digestive. Saliva contains enzymes that help break down and digest food.
- Protective. This liquid constantly moisturizes the oral mucosa and does not allow it to dry out. It also removes germs from the surface of the gums and teeth.
- Mineralizing. With its help, tooth enamel is nourished by minerals and does not collapse.
10 Causes of Increased Salivation in Babies
There are a number of factors that contribute to excessive salivation in a child. They can be physiological and pathological.
2 physiological causes
1
Immature swallowing reflex
. If a child is drooling at 2 months, do not worry too much about this. Most likely, this is a natural physiological process in the body of the baby. At this age, the swallowing reflex is still poorly developed in children and they simply cannot swallow all the saliva, so it flows down the chin. If, carefully read the information about its causes, in some cases this is a symptom of serious diseases.
At this age, the swallowing reflex is still poorly developed in children and they simply cannot swallow all the saliva, so it flows down the chin. If, carefully read the information about its causes, in some cases this is a symptom of serious diseases.
At this time, the mother should pay special attention to the hygiene of the baby:
- wipe the baby’s wet mouth with a dry cotton cloth;
- wash the baby with boiled warm water without any means;
- change more often into dry clothes.
Areas of the skin that are exposed to saliva should be lubricated with a nourishing cream for both treatment and prophylaxis
Constant moisture often causes irritation, peeling and rash on the skin around the mouth. In this case, you must first wash the baby with warm water and wipe it with a dry cloth, carefully wetting the moisture, and not rubbing the already painful skin.
Then you need to lubricate the damaged areas of the skin with Bepanthen ointment or its analogue – Pantoderm. Pantoderm is cheaper, take note of this. You can also use regular baby cream.
Pantoderm is cheaper, take note of this. You can also use regular baby cream.
2
First teeth eruption
. Also, the child drools heavily when teething. During this period, the secretory activity of the salivary glands increases greatly and can also cause a rash on the skin around the baby’s mouth due to constant moisture. Why does saliva flow in the baby during the appearance of the first teeth? Increased salivation plays an analgesic role in this case, reducing pain and alleviating the baby’s pain.
Some pediatricians and dentists refute this theory, but most specialists are still inclined to this version. You just need to survive this period, you should not interfere with the situation with medication.
Watch the video about the eruption of the first teeth:
8 pathological factors that cause hypersalivation
If none of these natural causes apply to you, then you are dealing with pathological factors:
1
According to statistics, most often the problem of increased salivation in children is caused by dental problems
, the most common of which is ulcerative stomatitis, an inflammatory disease of the oral cavity.
During ulcerative stomatitis, the mucous membrane becomes covered with painful ulcers. The little man experiences pain when swallowing, so he stops swallowing saliva and it flows out. If you pay attention to this process in a timely manner, then you can get rid of this pathology at an early stage.
Increased salivation in a 2-year-old baby may be caused by malocclusion
. Especially strong signs of hypersalivation appear at night. If examinations of the body and consultations of such specialists as a pediatrician and a neurologist did not give any result, then visit an orthodontist.
After examining and investigating the problem, treatment is prescribed. The sooner treatment is started, the easier it will be to get rid of the problem. In children, bite correction is faster than in adults. And by excluding the cause, the consequence will also disappear – hypersalivation.
2
In some cases, excessive salivation in a child is caused by gingivitis. With this disease, the gums become inflamed and saliva in this case plays a protective role. It is necessary to start therapy in a timely manner so as not to reach the inflammation of the salivary glands themselves.
With this disease, the gums become inflamed and saliva in this case plays a protective role. It is necessary to start therapy in a timely manner so as not to reach the inflammation of the salivary glands themselves.
3
Worm infestation, cerebral palsy, CNS disorders, some diseases of the eyes, ears and throat, malocclusion, diphtheria can also cause high performance of the salivary glands.
4
In case of severe poisoning of both children and adults with substances such as iodine, mercury, pesticides, a lot of saliva is also released. If you have identified these reasons in your case, then it is urgent to take the baby to the hospital.
5
Increased salivation in infants 2 months of age and older may be caused by thrush or oral candidiasis. It is manifested by a white coating on the mucous membrane of the mouth and sores. Examine the baby’s mouth and if these signs are found, take the baby to the hospital.
6
Allergy can also be a cause. Only a doctor can determine it, while parents can only diagnose a runny nose. Do wet cleaning more often in the children’s room, because dust allergies are more common in children than reactions to cats or plants.
Do wet cleaning more often in the children’s room, because dust allergies are more common in children than reactions to cats or plants.
7
Also drooling in a child and in case of problems with the digestive tract
. It is necessary to pass tests to exclude diseases such as hepatitis, gastritis, enteritis and other diseases of the digestive system.
8
Some drugs also contribute to this pathology. In this case, the attending physician must adjust the dose of the medication taken or replace the medication with another one.
All pathological factors that contribute to the release of large amounts of liquid in the mouth require getting rid of the underlying disease that provokes this ailment. When the pathology is eliminated, salivation will return to normal.
8 tips for parents on caring for a baby with physiological hypersalivation
If a newborn is drooling and the reason for this is physiological, then the mother can help her child on her own:
If the child is salivating during teething, relieve his condition by lubricating the gums with a cooling gel or ointment
- Pay attention to clothing. As soon as it becomes wet, it is necessary to immediately change it to a dry one, because a wet cloth can cause irritation and a rash on the baby’s skin. If you have to change clothes too often, then use special collars.
- The most common pacifier will literally save you. In the process of sucking the pacifier, the infant swallows saliva at the level of reflexes.
- If your baby is 3 months old and is drooling due to teething, offer your baby a special teether toy to bring the baby teeth closer. The toy can be cooled in the freezer.
- Reduce the pain of teething with a special cooling gel
. You can also put the rubber teether in the freezer for a while and then offer it to the baby. After a few moments, the pain will subside and the baby will calm down. - To avoid irritation or to get rid of it, use ointments and creams based on vitamins A and E.
- Bathe with decoctions of string or chamomile. They have anti-inflammatory and antiseptic properties, which will help remove signs of irritation on the skin of a little man.
- If your child is already 4 months old, you can ask your pediatrician about the possibility of introducing complementary foods at this age. Solid foods encourage chewing, which stimulates the swallowing reflex.
- Increase your little patient’s water intake to replenish lost fluids.
 As soon as it becomes wet, it is necessary to immediately change it to a dry one, because a wet cloth can cause irritation and a rash on the baby’s skin. If you have to change clothes too often, then use special collars.
As soon as it becomes wet, it is necessary to immediately change it to a dry one, because a wet cloth can cause irritation and a rash on the baby’s skin. If you have to change clothes too often, then use special collars. 
Excessive salivation in children two years of age and older
If the child is 3 years old and drooling, then in any case it is worth going to the hospital. Only specialists can answer the question of why this happens in a child at this age. They will determine whether drug therapy is needed in this case or whether this moment can be waited out.
When getting rid of these manifestations, it is necessary to compare the methods of treatment with the pathology itself. However, you can’t do nothing. Children with this problem may get a speech disorder
, because a large amount of clear liquid makes it difficult to pronounce words well. Subsequently, this can lead to delayed development and sociopathy.
By the age of 2, children can usually swallow. If a child is drooling at 2 years old, and if it is not teething, a speech therapist should be consulted.
At this age, molars may erupt in children. This can cause hypersalivation. As in the case of infants, the problem may arise due to ENT – diseases, diseases of the digestive system, stomatitis, gingivitis, allergies. If the problem manifests itself mainly at night, then the baby may have a helminthic invasion
.
Methods of treatment
If the trouble causing hypersalivation is pathological, then treatment must be carried out without fail in order to prevent exacerbation.
Folk remedies
Folk remedies should be in addition to medical methods. For little children, rinsing the mouth with decoctions of the following herbs can help:
- nettle decoction;
- sage infusion;
- cabbage pickle.
Weed should be selected by your local pediatrician. You can also use infusions by adding them to a bath for bathing with warm water. Here, tinctures of nettle, black elderberry, calendula, St. John’s wort or chamomile are suitable.
You can also use infusions by adding them to a bath for bathing with warm water. Here, tinctures of nettle, black elderberry, calendula, St. John’s wort or chamomile are suitable.
Yes, there are folk methods of dealing with these manifestations. They are especially effective if the cause of hypersalivation is problems with the oral cavity.
You can rinse your mouth with a decoction of chamomile or nettle. But this method should not be used as the main one. It is rather an adjuvant therapy that complements drug treatment. With serious problems, rinsing your mouth with herbs will not cope.
Also, do not forget that the use of folk remedies must be agreed with the attending physician. Many herbs are highly allergenic, so children are not allowed
.
Medicines
Therapy is carried out in two directions:
- Therapy of the underlying pathology, which provoked a strong salivation.
- Relief of the condition of the baby by reducing the pain effect.

If a month-old baby or an older baby is drooling, then drugs are prescribed that lower the function of the salivary glands.
Saliva – an indispensable helper of the baby in the fight against bacteria and viruses
However, they are prescribed in critical situations
, for example, if a newborn chokes at night, which can be fatal.
The very solution to the trouble depends on the cause of the appearance. In cases with colds and stomatitis, therapy will be prescribed by a pediatrician and dentist.
Basic treatments at home
At home, to alleviate the condition of the crumbs, you can act in this way:
- Applying ice cubes to the lip contour. In the case of a newborn, ice should be wrapped in a tissue napkin.
- Mouth rinse with herbs.
- Children aged 9-12 months can be massaged and exercised.
- Introducing solid foods into the diet will help develop the swallowing reflex. If the baby is too small, then a nibbler can be used.
 If the baby is too small, then a nibbler can be used.
If the baby is too small, then a nibbler can be used. Conclusion
It must be remembered that strong salivation is a temporary phenomenon, most often associated with the appearance of teeth in the crumbs and it is worth enduring. After the eruption of the main teeth, your child will feel better. However, it is necessary to exclude other factors that caused this trouble. To do this, record your symptoms so you can report them to your pediatrician.
We offer you to watch a video about one of the most common diseases among children – stomatitis, its causes, symptoms and treatments:
Attentive parents pay attention to any changes in the behavior and health of their baby when he is still in the womb, not to mention about that amazing period after birth.
Some moms and dads get worried when they see a 2 month old baby drooling and want to know why. Do not worry ahead of time, because after birth, the salivation of the child is only being formed and has some features.
Features of the functioning of the salivary glands in infants
Increased secretion of the salivary glands is called or ptyalism, although this phenomenon is most often called salivation. In the normal state, hypersalivation as a physiological phenomenon is observed in infants from 2-3 months to six months or a little older. This is explained by an interesting process of formation of the functioning of the salivary glands.
After the birth of the baby, he does not function fully. A small amount of oral fluid is released. By about 1-2 months, changes in this process begin to occur, the glands are activated and more saliva is formed. This is a physiological norm. Before this period, this should not be the case, that is, a healthy one-month-old baby cannot have a lot of saliva.
Starts at 2-3 months of age, which can be manifested by salivation. The inflammatory process is reduced by exposure to saliva, which also provides protection. At this stage, excessive salivation will not be eliminated, but you can help the teeth come out and alleviate the condition of the crumbs. Buy, they are placed in the cold and given to a baby who scratches his teeth.
Buy, they are placed in the cold and given to a baby who scratches his teeth.
By the age of three months, babies begin to actively explore the world and put everything in their mouths. Pathogenic bacteria can be found on toys. To this end, nature has provided for an abundant secretion of saliva, which has a bactericidal effect and tries to get rid of infections.
Non-dangerous circumstances
Apparently, at a certain age, excessive salivation in a child is caused by natural, non-dangerous causes:
- Insufficient work of the glands that are responsible for the production of saliva. In children under the age of , the process of formation of the salivary glands
continues, so a lot of saliva can be produced. The baby does not have time to swallow it, it flows out. - In babies up to 2 months, saliva ensures normal swallowing
. - In a three-month-old baby, abundant saliva becomes a harbinger of the appearance of teeth
. - In children who are breastfed, saliva protects the body from germs
. It contains maternal antibodies and prevents the development of stomatitis, tonsillitis, influenza and other diseases. - If a symptom occurs in formula-fed infants, then this is a consequence of the normalization of the digestive process
. Saliva promotes better absorption of mixtures.

Increased salivation in infants, and even more so in an older baby, can be due to certain diseases, so it is important to pay attention to other symptoms and go to the pediatrician.
Diseases as possible causes of salivation in children
Causes of drooling and blistering in babies may be related to certain conditions and diseases of the internal organs:
- Candidiasis
(thrush). The reason is the increased reproduction of Candida fungi. They are activated with a decrease in immunity. Symptoms include: redness, fever, and the appearance of a white coating in the mouth that resembles cottage cheese. - CNS diseases
. Increased salivation manifests some disorders of brain activity, in particular, cerebral palsy. Signs are impaired speech and coordination, weakness, convulsions and fainting. If already in 2-3 months there are such signs and the baby drools heavily with bubbles, you need to be examined by a neurologist. - Worms
. Accompanied by increased salivation at night. Other signs can also indicate the presence of worms: snoring, itching in the anus and in the groin. - Respiratory tract infection
. Accompanied by strong salivation and hyperthermia, coughing, sneezing and runny nose. - Stomatitis
. Inflammatory pathology of the oral mucosa. Accompanied by the formation of vesicles, ulcers on the mucosa. The child feels quite intense pain, which is why he cannot chew food or swallow. Sometimes the cause is inflammation of the gums or salivary glands. - Allergy
. If drooling is pouring after being outside or during flowering, it may be an allergy. - Intoxication
. If the newborn is drooling, the cause may be drug or food poisoning. This condition is accompanied by diarrhea and vomiting, swelling of the mucous membranes, flushing of the face and body.


An examination can help you figure out why a two-month-old or older baby is drooling. Ignoring such a sign can lead to serious consequences.
Symptoms to watch out for
Drooling in a 3-month-old baby and an older baby is most often not a sign of pathology, but there is still a chance. It is important to pay attention to accompanying symptoms that will prompt the cause and further actions:
- The baby always puts various objects into his mouth, he is about six months old and is irritable. It probably is. You can give your child a pacifier, special rubberized rings.
- Abundant salivation is accompanied by pain in the throat, head, nasal congestion with snot, sneezing, coughing, fever – this is SARS or tonsillitis. You need to call a doctor.
- Sores or light spots are observed on the oral mucosa -. Rinse with a solution of soda, take the child to the doctor.
- The child breathes through the mouth with noise, the chin is lowered, fever, a pronounced pain syndrome develops in the throat – swelling of the epiglottis. Occurs in children after 3 years. You should calm the child so as not to aggravate heavy breathing, go to the hospital.
- A sharp fall with a shudder of legs and arms – convulsions. Call an ambulance immediately.
 You need to call a doctor.
You need to call a doctor. What parents should do
The following steps will help relieve the child’s condition:
- put on a bib to keep the jacket from getting wet;
- wipe the baby’s neck and chest;
- use a pacifier: it stimulates swallowing but is addictive;
- remove saliva from the body in time, apply cream to the skin;
- when teething, use special devices.
How to avoid irritation from saliva
The most common cause is teething. To prevent itching and irritation, it is necessary to put a diaper at the head of the bed.
To prevent itching and irritation, it is necessary to put a diaper at the head of the bed.
It is necessary to lubricate the face with cream at the first signs of irritation from saliva. The following drugs can be used:
- Bepanten
– cream for diaper rash and irritation. - Weleda
– ointment based on natural ingredients. You can learn about Weleda toothpastes from. - Pantestine
is a drug that accelerates cell repair.
If the rash develops gradually, more effective skin medicines can be used: Sanosan Baby, Sudocrem and others. They have an effect on the inflammatory process, kill microbes.
It should be noted that drooling is not necessarily the cause of the rash. This is a sign of one of the serious diseases: measles, rubella and others. You need to consult a pediatrician.
How the problem is treated
A pediatrician’s consultation will show if the hypersalivation is pathological and if medication is required. It is important to identify the root cause of salivation. If it cannot be eliminated, treatment is aimed at reducing the severity of symptoms.
It is important to identify the root cause of salivation. If it cannot be eliminated, treatment is aimed at reducing the severity of symptoms.
At the same time, the volume of saliva may be normal, but the child does not swallow it in time. It is important to understand that salivation is a process in which the receptors of the nervous system take part. When a sufficient amount of liquid is collected, a signal is transmitted to the brain to swallow it with the help of receptors. In some cases, the flow of information does not reach the brain, this happens due to sensitivity failures or pathologies of the sensorimotor arc. The number of swallows decreases and the volume of saliva increases.
To correct this problem, correct the sensorimotor arc. It is necessary to create conditions so that the brain begins to receive the necessary information. The most effective way to fight is cryotherapy. An ice stick is passed over the child’s tongue. This helps to reduce or stop hypersalivation. The method does not work immediately, requires perseverance, but is less painful than surgical correction. Anticholinergic drugs are also prescribed, for example, Atropine.
The method does not work immediately, requires perseverance, but is less painful than surgical correction. Anticholinergic drugs are also prescribed, for example, Atropine.
Severe salivation in an older child can lead to impaired speech. This slows down development and negatively affects socialization, so visits to the doctor and treatment should not be postponed.
There are three main pairs of salivary glands in the mouth: submandibular, sublingual and parotid, and about 1000 minor glands. From 500 to 2000 ml of saliva is secreted per day.
The submandibular and sublingual glands secrete saliva through channels into the anterior part of the mouth, under the tongue (Figure 1). The submandibular gland secretes most (about 65%) of the saliva in the mouth, this saliva is watery. The sublingual glands produce some saliva, which is viscous and slimy. The canals of the parotid glands open into the mouth near the second upper molars. These large glands are most active during meals.
General, unconscious control of salivation is carried out by the sympathetic and parasympathetic nervous system (vegetative nervous system).
Main functions of saliva
- Lubricates food to aid in chewing and turns food into a bolus (soft ball) for easier swallowing
- Lubricates the tongue and lips during speech.
- Cleans teeth and gums and helps with oral hygiene.
- Controls acidity in the esophagus
- Destroys microorganisms and cleans toxic substances.
- Facilitates the taste. Initiates the digestion of carbohydrates.
Why do some children drool?
Excessive salivation and drooling may be normal in the first six to eighteen months of life while oral motor function develops. Drooling is considered abnormal for a child over four years of age. Persistent drooling is most common in cerebral palsy or other severe neurological disorders. There is a small group of healthy children who drool before the age of six. This is not an overproduction of saliva, but an inefficient voluntary swallowing of saliva. In this group, there may be high extrinsic saliva loss, intraoral sensory dysfunction, impaired intraoral motor activity, or a combination of these factors. There are 5 degrees of severity of salivation (table 1).
This is not an overproduction of saliva, but an inefficient voluntary swallowing of saliva. In this group, there may be high extrinsic saliva loss, intraoral sensory dysfunction, impaired intraoral motor activity, or a combination of these factors. There are 5 degrees of severity of salivation (table 1).
Severity of salivation
Severity of salivation (according to Thomas-Stonell and Greenberg):
2. Mild – wet lips
3. Moderate – wet lips and chin
4. Severe – wet clothes
5. Profuse – wet clothes, hands and objects
and Greenberg):
1. Never
2. Occasionally
4. Constantly
How to manage salivation?
There are four main methods for managing salivation:
1. Conservative methods
It is important to evaluate the underlying problems that may exacerbate the problem of salivation control, such as the presence of nasal congestion, dental disease, or the use of medications that may be causing the problem. Improving posture with the participation of a physiotherapist. Rearranging the computer screen and input device (keyboard or switch) can also be helpful in achieving improved posture.
Improving posture with the participation of a physiotherapist. Rearranging the computer screen and input device (keyboard or switch) can also be helpful in achieving improved posture.
Conservative methods include behavioral approaches and techniques to improve a child’s sensory awareness. These two strategies can reinforce each other. The behavioral approach involves teaching the child to recognize the feeling of dampness and the ability to either swallow saliva more often or wipe saliva from the lips and chin; helping the child develop the ability to close the lips and suck saliva. Strategies include developing the ability to suck up secretions in the mouth with straws of various thicknesses, as well as liquids of various consistencies. Many children appear to be unaware of saliva in or around the mouth, and may be sloppy in eating. The development of eating habits directly related to saliva control includes control of the length of time the child closes the lips and the development of lateral movements of the tongue during chewing. Lateral chewing is encouraged by placing food of varying density between the molars.
Lateral chewing is encouraged by placing food of varying density between the molars.
The success of these methods depends on the team (physician, speech therapist, parents, child), the degree of oral motor ability and the ability to follow instructions.
2. Technical methods.
There are a number of devices that can help your child position their tongue better in their mouth and swallow more effectively. Techniques can be challenging for children and their families, and require close supervision. It can be an effective treatment for children with cerebral palsy who are motivated and able to follow instructions. The device is worn for short periods of time each day and improvements are noticeable after 9 years0003
3. Drug therapy
Anticholinergics, especially benzhexol, benztropine, and glycopyrrolate, successfully dry saliva in some children. These drugs block the transmission of signals from the parasympathetic nervous system to the salivary glands. Side effects, particularly sedation and restlessness, may limit their use. These drugs should be administered gradually in slowly increasing doses, since the effective dose varies from person to person.
Side effects, particularly sedation and restlessness, may limit their use. These drugs should be administered gradually in slowly increasing doses, since the effective dose varies from person to person.
Drug treatment is beneficial for:
- Small children who are still developing oral functions.
- In older children and adults with relatively mild saliva control problems.
- Optional as an alternative to surgery
A new approach to the treatment of salivation is the injection of botulinum toxin into the salivary glands. This method is still in clinical trials, but may be a good way to provide short-term salivation control.
4. Surgical treatment
The surgical approach is used if:
- Salivation is so severe that conservative measures are unlikely to give a satisfactory result.
- The use of conservative approaches is unlikely due to severe mental and/or physical disability.
- The child is older than six years and conservative treatment is not effective. Maturation of rotofacial function can continue up to six years of age in children with developmental disabilities, so surgery is not usually offered before this age.
 Maturation of rotofacial function can continue up to six years of age in children with developmental disabilities, so surgery is not usually offered before this age.
Maturation of rotofacial function can continue up to six years of age in children with developmental disabilities, so surgery is not usually offered before this age.
A range of surgical options include salivary gland denervation, salivary gland removal, salivary duct ligation, and canal repositioning.
The benefits of denervation (transection of the autonomic nerves) are lost within a year, possibly because the nerves regenerate. The nerves that transmit taste sensations are also divided.
Isolated removal of the salivary glands may lead to compensatory hyperactivity of the remaining salivary glands. A severe decrease in saliva production causes dry mouth, increased caries and impaired swallowing.
The currently preferred method is relocation of the submandibular ducts and removal of the sublingual glands. With any saliva control surgical procedure, it is important to ensure that good dental health is maintained for months and years after surgery. All young people who have had surgery should carefully visit the dentist, as there is an increased potential for caries.
All young people who have had surgery should carefully visit the dentist, as there is an increased potential for caries.
Compensation Strategies
Saliva stains clothes, may smell bad if salivation is severe. When the child is small, it is often necessary to change waterproof bibs. As the child gets older, there must be a better way to mask salivation:
- Scarves can be worn around the neck to absorb excess saliva. They can be made from absorbent fabrics such as grouts. Matching scarves can be a tricky way to mask salivation. It’s good to have several scarves of the same color as they need to be changed regularly.
- Towels can be sewn into windbreakers to absorb excess saliva, and waterproof material can be sewn on to keep the skin dry.
- Easily replaceable vests can be worn on the dress.
- A patterned cotton collar can be attached to clothing with Velcro, which can be quickly changed when wet.
- Towel cuffs can be attached to Velcro sleeves to wipe saliva.

Salivation causes a range of physical and psychological complications.
Physical complications include maceration of the fissure around the mouth, secondary infection, dehydration, and bad breath. Psychosocial complications include isolation, barriers to education (eg, inability to use a computer keyboard), and increased dependence on levels of medical care. guardians
and loved ones may show affection for the child, contributing to potentially damaging ostracism from peers.
Often, saliva is profusely secreted from the mouth of a newborn. He constantly sucks his fists and fingers, and his parents begin to worry. Some expect the eruption of the first teeth, while others associate it with some kind of disease. As a rule, few adults know that all babies from birth and by about 8 months still do not know how to swallow saliva. Such a physiological process, which can be observed both day and night, is quite natural. The main thing is to find out the reason and understand why a 2-month-old baby is drooling.
Causes
If profuse salivation was noticed at 2 months, do not rush to see a doctor. At this age, the baby shows interest in his little hands, constantly putting them in his mouth, causing a salivation reflex. Parents immediately look into the child’s mouth and see if he is teething. But it is still very early for the appearance of teeth, usually they begin to appear after 5-6 months.
In infants, it performs several basic functions for the body:
- Remineralizing
– protection for tooth enamel. - Protective
– permanent moisturizing of the oral mucosa, reduces the risk of its drying out, and also helps to remove microorganisms. - Digestive function
– enzymes present in saliva contribute to the rapid digestion of food.
What to do when a newborn drools profusely?
The cause must be determined before any preventive action can be taken. To do this, the mother should carefully examine the mouth of her child for possible inflammation. If there is no redness inside the oral cavity, then it may be a possible cause. Abundant salivation can be observed both in a 2-month-old baby and in older children.
Main symptoms:
- clogged nasal passage
- it is very difficult for the child to breathe.
In addition, when the first teeth erupt in babies, abundant saliva effectively reduces pain. During this period, more than ever, the baby needs to frequently change children’s clothes (suits and underwear), as well as use bibs. After all, from excess moisture, the baby’s chin can get irritated.
If the baby has a rash under the lower lip, then buy special baby creams in the pharmacy that contain vitamins E and A.
When to consult a specialist
A loud cough or wheezing in the chest is one of the signs of increased salivation in infants. In such cases, the mother needs to turn her child on her tummy so that the fluid does not accumulate in his larynx.
If salivation alternates in duration, it is better to contact your pediatrician in order to avoid an infectious exacerbation.
In most cases, this can cause serious illness, such as hypersalivation. It rapidly affects the nervous system of the child, and in some cases, contributes to the development of mental illness.
Advice is important!
Only with a thorough examination, a pediatrician can determine the cause and only after that, prescribe an effective treatment.
If a 2-3 month old baby drools heavily from the mouth, then you shouldn’t worry too much. After all, this is a natural physiological development, which can be observed up to 1-1.5 years.
Over time, the baby will outgrow, and all worries will go away!
Excessive salivation in a 5-year-old child. Why does a baby drool
Mothers and fathers of small children often experience excessive salivation in the crumbs. Of course, parents stoically wipe the baby’s drool, attributing it to age, predicting the rapid appearance of the first teeth, and the like. However, saliva begins to run in a stream already at the age of three months, and the teeth for the first time come out more often by six months.
Let’s try to figure out what, in fact, is associated with abundant saliva in the first year of a child’s life. The salivary glands are formed by the age of two to three months, it is at this time that parents notice that their baby is actively blowing bubbles. As a rule, the baby does not know how to swallow saliva, so it seems to the mother that there are too many of them. While there are no teeth yet, salivary fluid provides comfortable swallowing during breastfeeding and, after the introduction of complementary foods, helps digest food in the stomach due to special enzymes that convert starch into sugar.
At this stage, try to keep your chest dry by changing your blouses often or by wearing a waterproof-lined bib around your neck. Sometimes around the mouth or on the chin it can appear in the form of small pimples resembling a rash, or red spots due to constant moisture.
In this case, lubricate the damaged areas with baby cream at least a couple of times a day (ideal with vitamins A, E, chamomile extract). When wiping with a handkerchief, make gentle blotting movements, do not rub dry already irritated skin.
Saliva is also a kind of antibacterial agent. It contains a special substance that has antimicrobial properties.
Since children put everything into their mouths, saliva has a protective function. Closer to half a year, in a baby, they can really indicate the close appearance or eruption of teeth. Being deep in the gum, the tooth still grows, rising higher to the surface and causing pain to the crumbs. At the same time, saliva effectively moisturizes the gums, thereby softening the discomfort during teething. During this period, do not forget to slip all kinds of teethers on your baby, just keep them clean in the refrigerator door. Not bad help and special cooling gels when teething.
In some children, teething may be quite accompanied (sometimes higher than 39), which indicates that salivary fluid alone was not enough to provide an antiseptic effect.
![]()
Do not worry about this, even if you have to spend several days with the child in the hospital under the supervision of doctors. This condition usually lasts for about three days (sometimes five). This is also the norm, just your baby’s body has its own individual characteristics.
With profuse salivation, parents quite often observe their children in the chest, especially in the morning, after waking up. At the same time, the baby can cough strongly, sometimes this happens not only in the first hours after sleep, but also at night. This fact alarms many mothers, and they immediately run to see a pediatrician in a clinic. Of course, for your own calm, it is better to do this in order to exclude those accompanied by a wet cough, redness and sore throat. But more often than not, the child is really all right. Just an excess of saliva causes congestion in the larynx. In this case, experts recommend putting the baby on the tummy more often.
It is desirable that the baby sleeps on his stomach or side more often.
You can also put a folded diaper or a thin pillow (sold specifically for newborns) under your head. On his back, he can choke and wake up from his own cough.
So, profuse salivation in children of the first year of life is a completely normal phenomenon, but still, sometimes, this fact can be a signal of the presence of other diseases.
Often, increased salivation in children of the first year of life is an eternal companion with a cold, since mouth breathing predominates. Another possible cause is inflammatory diseases of the oral cavity, including and.
In rare cases, more serious illnesses may occur.
Hypersalivation is a medical term that refers to increased salivation due to disorders associated with lesions of the nervous system, mental illness.
Hypersalivation may be the result of brain injury, the presence of a tumor.
In this case, the most careful monitoring of the health of the crumbs and changes in his behavior is required. Increased salivation after a year can lead to impaired speech in a child, hinder the processes of socialization.
If parents are worried about the baby’s drooling, it is better to consult a pediatrician or a pediatric neurologist so as not to make false diagnoses yourself.
In general, increased salivation is considered a healthy physiological process. It can be observed in a child up to one and a half years. So be patient and stock up on bibs, teethers and disposable handkerchiefs.
Drooling is quite common in children under two years of age. But when saliva is produced in too much quantity, it can cause concern for parents.
Roza Serdyuk, chief physician of Okdoctor, a remote telemedicine consultation service, told Letidor when salivation is considered normal and when it can be a symptom of a disease.
Why saliva is needed
Saliva is a clear, colorless liquid that is produced in the oral cavity by the salivary glands.
Its functions are quite diverse:
- Participates in the initial stages of food processing
: under the action of enzymes, gradual digestion of fats begins, enveloping food fragments, which facilitates the further movement of the food bolus through the digestive tract.Thanks to saliva, we can feel the taste of food, we have an appetite.
- Protects
– the substances contained in it prevent the excessive growth of pathogens; protects
tooth enamel from the aggressive influence of acids and alkalis. - Contains substances with analgesic effect
, which is important when teeth appear in babies. - Adjusts self-cleaning mechanisms
mouth and teeth, washing them from food particles and bacteria. - Participates in speech formation
.
What is considered normal
Hypersalivation, the scientific name for increased salivation, is characterized by increased secretion of the salivary glands, as a result of which the child produces too much saliva.
The baby’s salivary glands begin their work in the womb. Their active functioning occurs closer to two months.
In children 3-4 months of age, saliva often flows from the mouth. This is due to immaturity in the control of salivation and ingestion of saliva (physiological salivation). At this age, the child tries to pull all objects into the mouth, thus recognizing the environment. Often, toys are not sterile, and microbes that enter the body begin to attack it.
iconmonstr-quote-5 (1)
In response to such an “invasion”, the active work of the salivary glands begins, which indicates the correct functioning of the immune system.
When a child has a runny nose and has to breathe through his mouth, the work of his internal organs instantly changes. So that when air is inhaled, the mucosa does not dry out, the salivary glands begin to actively produce their secret, which helps to humidify the inhaled air and disinfect it.
There are also cases when a child chokes on saliva and coughs when breathing through the mouth, as they are unable to breathe and swallow the accumulated liquid at the same time.
iconmonstr-quote-5 (1)
For children under two years of age, this condition is considered physiological, it is associated with the appearance of teeth.
When medical attention is required
However, there are pathological conditions that are not physiological and require medical attention.
Pathology of the oral mucosa: eg thrush, stomatitis; viral diseases that affect the salivary glands themselves (viral sialadenitis), the so-called false hypersalivation, when the amount of saliva remains normal, and leakage occurs due to the pain syndrome associated with the above conditions.
Pathology of the nervous system (cerebral palsy, brain tumors, encephalitis, pseudobulbar syndrome (damage to the cranial nerves), etc.).
Problems of the gastrointestinal tract (gastritis, enteritis, etc.).
Worm infestations.
Poisoning by poisons, barbiturates, mercury, lead, etc.
What to do if a child is drooling heavily
The main thing is to recognize whether excessive salivation is a signal of a dangerous illness. This will be helped by a pediatrician who, if necessary, will refer the child to a narrow profile doctor to clarify the diagnosis and correct treatment.
If increased salivation is due to the imminent appearance of teeth, then the following can be recommended to the mother of the child:
Wear baby bibs that do not get wet and protect the baby’s skin from hypothermia during a walk.
In case of skin lesions due to prolonged contact with saliva, lubricate the affected areas with dexpanthenol ointment or creams that contain retinol and vitamin E.
Offer cool teethers to the baby. They will temporarily relieve itching. You can also use anesthetic gels.
Make sure that objects put into the child’s mouth are clean and cannot be swallowed.
If a two-month-old baby suddenly drools, then many parents diligently begin to look for swollen gums or teeth that have already crawled out in his mouth.
But the first teeth in children very, very rarely appear in the third month of life. So why then does the baby drool so much and blow bubbles?
Why does a 2 month old baby drool?
1. Beginning of the functioning of the salivary glands.
This is the most common reason. In the third month, the active work of the salivary glands occurs, a large volume of saliva begins to be produced. And the swallowing reflex is fully formed only by 5 months, so the baby simply cannot swallow so much saliva. Precisely for this reason saliva flows out.
2. We are waiting for the first tooth.
Despite the fact that the first teeth appear after four to six months, the gums can already begin to prepare
to this event. The teeth gradually begin to move in the gum, preparing to come out in a few months. The body begins to produce an increased amount of saliva to moisten the irritated gums. As soon as the first tooth cuts a hole in the gum, the amount of saliva will decrease.
3. Saliva protects the little organism.
It turns out that the baby’s saliva contains special antibacterial substances
. They help to neutralize infections that enter the mouth. This is an extremely useful and necessary property of saliva. Starting from 2 months, a small child begins to put everything in his mouth.
It can be a rattle, your own hands or your mother’s finger. It is abundant saliva that prevents infections and bacteria from entering the baby’s body. Salivary fluid washes the mouth and flows out along with possible bacteria.
4. Allergic reaction.
Approximately 15% of babies are predisposed to such a disease as allergic rhinitis.
Signs of this disease, in addition to profuse salivation, are also swelling of the mucous membrane, watery eyes, sneezing, itching in the nose. The cause of such rhinitis can be dust, flowering plants, pet hair.
If you observe all these symptoms in an infant, you should consult a doctor and get advice and appropriate treatment from him.
5. Diseases of the oral cavity.
Sometimes excessive drooling may indicate oral diseases such as thrush or stomatitis.
In addition to increased salivation in these diseases, the child is restless, capricious, will suck badly and white plaque or plaques can be found on the mucous membranes.
If you experience these symptoms, you should immediately contact your pediatrician and seek treatment advice.
6. Hypersalivation.
Very rare, but excessive salivation may be one of the signs of serious illness
.
In order not to miss the disease, you should carefully monitor the health of the baby, take all the necessary tests and studies according to age.
A consultation with a neurologist and a pediatrician will clarify the picture and relieve parents of unnecessary suspicions.
Many parents become anxious when their little child suddenly has a drool bubbles
. It shouldn’t cause any concern at all. Moreover, it is considered an absolute norm. Blowing bubbles is a new skill for the tiny two month old creature.
How to survive such profuse salivation?
From the beginning of the third month of life, abundant saliva occurs in almost all babies.
And if at first they do not cause any discomfort, then over time, constant drooling wets clothes and can cause inflammation around the mouth and on the chin.
Here are 5 tips for you
, which can and should be used during the “salivary period” of the baby.
- Change wet clothes more often.
And let it add washing to mom, but the baby will always have a comfortable dry breast and neck. - Buy and use a lot of bibs
and change them as needed. In stores, you can now find colorful bibs of various colors and textures. - Wipe baby’s face with sterile gauze or a clean soft handkerchief.
In this case, do not rub the already damaged skin of the child. If, nevertheless, irritation appears on the skin, then cracks and pimples should be lubricated with baby cream or sea buckthorn oil. - If increased salivation is associated with the eruption of the first teeth, then it is necessary to acquire special teethers or teethers.
Various teething gels have proven themselves very well in this case, they significantly reduce pain and cool the gums. - Be patient and get used to your baby’s constant saliva.
After all, children’s drooling is a continuous phenomenon. After six months, active teething will begin and drooling, flowing in a stream, will not disappear anywhere.
Conclusion:
Increased salivation for babies up to a year old is an absolute physiological norm.
If parents are very concerned about this problem, then you can consult a pediatrician about this.
Over time, the drool that flows like a river from your baby’s chin will certainly decrease, and then completely disappear. And you will remember with nostalgia this “dribbling period” in the life of your child.
Why the baby is drooling
? This question begins to bother parents of three, two-month-old and even one-month-old babies. Many mothers and fathers think that the crumbs are teething.
Does salivation really mean that the baby is teething? Let’s figure it out together.
The baby drools at 1 month
At this age, the baby should first of all exclude thrush or fungal stomatitis. With this disease, a white coating appears on the tongue and cheeks and salivation may occur. The pediatrician treats this disease.
The baby drools at 2 or 3 months
From about two months old, the active work of the salivary glands begins in the children, and babies do not know how to swallow saliva. That’s why is drooling
. (Babies won’t learn to swallow saliva until they’re nine months old.)
From about three months, the baby begins to move more confidently with his hands, at first accidentally, and then more and more confidently pushes his fists, and later fingers in his mouth. A little later, he will learn to put it in his mouth and taste everything that he can hold in his hands: toys, a pacifier, random objects. This is how he understands the world.
Salivation and the habit of pushing fists into the mouth in a child up to four or five months does not mean that the child is teething.
Read more about the features of the third month of a baby’s life read
Baby drools at 5 6 or 7 months or older
Six months is the average teething time, but it’s not the same for everyone.
In some children, the first teeth erupt at five, four and even three months. Twice I have seen children born with teeth.
In another part of the babies, on the contrary, teeth are cut later: at seven, eight, nine months and even at 1 year.
In some children this happens unnoticed by the parents. One day they discover teeth in the baby’s mouth. Sometimes the fact that the child already has the first tooth, the mother learns at the examination of the pediatrician.
But, unfortunately, not everyone goes smoothly and imperceptibly.
How can you tell if a child is teething?
- The baby becomes restless, naughty, sleeps restlessly, eats worse.
- The gums in the place where the teeth will soon erupt become red and swollen.
- Erupting teeth cause itching and soreness of the gums, encourage the baby to constantly rub (scratch) the gums. If you touch the gums with a spatula or finger in the place where the teeth are cut, you will notice that this gives the baby pleasure.
- The baby begins to drool, even more intensively than before. Some children get wet clothes on the chest (a bib is required), the skin of the cheeks and chin turns red from irritation with saliva. Increased salivation during teething is associated with an increase in the intensity of blood circulation in the oral cavity.
- Along with increased salivation, a runny nose or loose stools may appear. This is due to more intense blood circulation during this period, not only in the oral cavity, but also in the mucous membranes of the nose and gastrointestinal tract.
- During teething, children may have an increase in body temperature.
- During teething, all or only part of these symptoms can be observed simultaneously, namely, salivation and an obsessive desire of the child to put everything that comes into his mouth in order to relieve itching in irritated gums.
From 6 months to 2 years 6 months teething occurs with short breaks. In some children, this process lengthens, and milk teeth continue to erupt until 3 years and even 4 years. Therefore, salivation or increased salivation can often be observed in a child of this age.
Drooling in a child older than 3 years
Stomatitis in a child
This is a viral, bacterial or fungal disease of the oral cavity in a child, which is often accompanied by increased salivation. But besides salivation, other symptoms of stomatitis are also noted: rashes or plaque in the oral cavity, soreness in the mouth, fever, refusal to eat. Stomatitis most often occurs in children 2-7 years old. If a child has the above symptoms, you need to show him to the doctor.
Change of teeth
From the age of 5-6-7, children change their milk teeth to permanent ones. At this age, teething is rarely accompanied by salivation. the child is already able to control this process. But some parents may note that the child drools during a conversation or sleep, the reason may be the eruption of permanent teeth.
Child drools at night
Children of all ages and adults may drool on the pillow at night.
As a rule, this is associated with a violation of nasal breathing or diseases of the oral cavity.
When nasal breathing is disturbed, a person breathes through the mouth all night, does not swallow saliva, and saliva flows onto the pillow.
Nasal breathing in children is most often disturbed due to enlarged adenoids, rhinitis (infectious or allergic), or due to a deviated nasal septum. To deal with these problems, you need to contact an otolaryngologist.
In diseases of the oral cavity: stomatitis, gingivitis, as well as during teething, saliva production increases and the child is not able to swallow it during sleep. In these cases, you need to contact a pediatrician or dentist.
Now you know why the baby is drooling
. Stay healthy!
The causes of increased salivation in children (hypersalivation) can be different. They are quite harmless, but sometimes require attention and even treatment. And yet, if you notice increased salivation in your crumbs, you should not immediately panic and sound the alarm. The first thing to do is to understand the causes of the problem.
Causes of excessive salivation in children
The process of salivation is absolutely natural and normal. During the day, up to more than two liters of saliva can be produced in the mouth, while the bulk is swallowed. So it should be in the normal state of the child. But what if salivation clearly exceeds the norm?
First of all, it should be remembered that hypersalivation in children under six months of age is a natural process that does not indicate diseases or abnormalities. In older children, increased salivation may have the following causes.
Teething
This cause is harmless and normal, so if the baby is already 6 months old or more, increased salivation should not worry his parents (although you still need to show the child to the doctor – for prevention purposes).
Teething is a difficult and rather painful process. You can alleviate the suffering of the crumbs by giving him a special teether or a silicone toy. Ice also helps a lot – it relieves swelling and eliminates inflammation. An alternative to ice can be a frozen piece of banana or apple wrapped in cheesecloth or nibbler.
Inability to swallow saliva
This pathology is possible in 1-2 years, but it should be gone by 3-4 years. The inability to swallow saliva is often observed in allergy sufferers – due to the constantly stuffy nose, the mouth of such children is always open. The kid uses it for breathing. Consequently, saliva is not swallowed, but flows down the chin.
With this pathology, it is urgent to show the child to an ENT specialist, as well as to consult an allergist and a speech therapist.
Identify the causes of allergies (if the inability to swallow saliva is associated with it) and remove the allergen from the house (wool, flowers, dusty things).
This pathology must be eliminated as soon as possible, because due to excessive salivation, the child may have problems with speech.
Diseases of the oral cavity
Children of all ages may experience a range of inflammatory processes in the throat and mouth. The most common are stomatitis and gingivitis.
- Stomatitis
– a disease in which small ulcers appear on the mucous membrane. Ulcers are covered with a light white coating, may bleed and are very painful. most often occurs due to the ingress of dirt into the oral cavity. Also, excessive consumption of sweets can be the cause. - Gingivitis
– gum disease. Increased salivation in this case is a protective reaction of the body. Gingivitis needs to be treated as early as possible to avoid problems later on.
If any disease of the oral cavity is suspected, the child should be shown to the pediatrician and dentist. Such reasons should be eliminated as soon as possible.
Poisoning
Poisoning is one of the most dangerous causes, which manifests itself through increased salivation in children. The toxic substance can be mercury, iodine, pesticides and other potent substances.
In this case, you should immediately call an ambulance – only experienced doctors will be able to find out how badly the baby was injured and whether he needs hospitalization.
Diseases of the gastrointestinal tract
These diseases include:
- ulcer;
- pancreatitis;
- worms;
- food poisoning;
- infectious diseases and others.
Only a special analysis can detect the presence of a gastrointestinal disease. It will be prescribed by a pediatrician as soon as the child suspects a problem with the tummy.
Diseases of the nervous system
In this case, the child needs to consult a neurologist. It is possible to alleviate the condition and “calm down” excessive salivation with the help of folk remedies. Brew your child herbal teas from chamomile, horsetail, calendula, St. John’s wort. Also an effective remedy is rinsing the mouth with infusion of sage.
How to get rid of excessive salivation?
First of all, it is necessary to find the causes of this deviation and begin to deal with it.
If the child is teething, no additional measures (other than those described above) should be taken. But if the reasons are more serious and consist, for example, in problems with the oral mucosa, then measures must be taken immediately. Currently, there are many medicines for stomatitis and gingivitis, but before using pharmaceutical preparations, you should consult your doctor.
You can alleviate the child’s condition with the help of traditional medicine. For stomatitis, rinsing the mouth with salt water helps well. And with gingivitis, it is recommended to use sea buckthorn oil.
In general, to prevent any diseases accompanied by abundant salivation, it is necessary to strengthen the child’s immunity. For this, a healthy diet, good sleep, lack of stress and worries, and regular walks in the fresh air are best suited.
Conclusion
Even if it seems to you that your baby’s excessive salivation is caused only by teething, it is better not to take risks and immediately take your baby to the doctor. He will reassure you if everything is in order, but if the child has problems, then they should be identified at an early stage and treated immediately.
Hypersalivation in Parkinson’s disease: causes and treatment options
Salivation (sialorrhea, hypersalivation, ptyalism) is characterized by an increase in the amount of saliva with its outflow from the oral cavity through the border of the lips in such a volume that it negatively affects social and household activity and daily life of the patient, leading to damage to the soft tissues of the oral cavity, lips and chin. Parkinson’s disease (PD) is the most common cause of sialorrhea in adults. The frequency of this suffering in PD varies from 45 to 80% [1, 2]. Some researchers note a lower prevalence of sialorrhea – 10%. Initially, salivation disturbs only at night, but later, with the progression of the disease, and in the daytime. Although the association of sialorrhea with PD has been known since the classic monograph by J. Parkinson, the pathophysiology of sialorrhea has not been sufficiently studied.
Functioning of the salivary glands under physiological conditions
Depending on the size, small and large salivary glands are distinguished. Minor salivary glands are localized in the mucous membrane of the lips, cheeks, tongue, hard and soft palate. Large salivary glands are located outside the mouth. Three pairs of major salivary glands (parotid, submandibular, sublingual) produce and secrete saliva. Parotid glands ( glandula parotidea ) are located directly under the skin, in front and downward from the auricle, on the lower jaw, at the posterior edge of the masticatory muscle.
The external carotid artery and its branches pass through the parotid gland. Per day, the parotid glands secrete about 1/3 of the volume secreted by all salivary glands (approximately 0.2-0.7 liters of saliva).
Submandibular salivary gland ( glandula submandibularis ) is located superficially, under the cervical fascia and skin. Medially, it borders on the styloglossus and hyoid-lingual muscles, from above on the lower jaw, and from below it emerges from under its lower edge. In front, the gland is in contact with the posterior edge of the maxillofacial muscle, and laterally adjacent to the facial artery and vein. The submandibular gland secretes saliva containing both mucous and serous (protein) secretions.
The sublingual gland ( glandula sublingualis ) is located immediately under the mucous membrane of the floor of the mouth, on both sides of the tongue, on the upper surface of the maxillohyoid muscle. Laterally it comes into contact with the inner surface of the body of the lower jaw, medially with the genio-lingual, geniohyoid, hyoid-lingual muscles. The sublingual glands secrete saliva containing a serous (protein) secret. It is richer in mucin than the saliva of the parotid and submandibular glands, has a pronounced alkaline reaction and high phosphatase activity [3].
The secretory activity of the salivary glands is regulated by the salivary zone of the cerebral cortex and the nuclei of the brainstem. This zone is excited by signals coming from taste buds. Further, the cortical zones interact with the upper (in the area of the small-celled reticular nucleus) and lower (in the lateral part of the reticular formation) salivary centers of the brainstem.
The secretory activity of the salivary glands is provided by sympathetic and parasympathetic innervation. However, when eating and swallowing, the activity of parasympathetic innervation is mainly activated. Parasympathetic afferent pathways, receiving a signal from the receptors of the pharynx and esophagus, through the system of the vagus nerve and visceral nerves reach the salivary center located in the medulla oblongata [2-4].
Parasympathetic efferentation occurs through two pathways. The glossopharyngeal nerve innervates the ear ganglia and subsequently the parotid gland via the auriculotemporal nerve. The facial nerve innervates the submandibular ganglia through the tympanic string and then through the lingual nerve ensures the functioning of the submandibular and sublingual glands [5] .
The process of salivation is inextricably linked with swallowing. The act of swallowing consists of three phases: oral, pharyngeal and esophageal. The oral phase is voluntary, while the pharyngeal and esophageal phases are involuntary. The act of swallowing begins with the involvement of more than 30 different muscles of the oropharynx to form and move the food bolus into the esophagus. Subsequently, the upper esophageal sphincter (UES) opens and the food bolus passes from the pharynx to the esophagus, and then to the stomach [2, 6]. Central motor control of swallowing is provided by the premotor cortex, primary motor cortex, basal ganglia, pedunculopontine nucleus, and cerebellum. The central neurons project onto the stem centers of swallowing, in particular the nuclei of the solitary tract (common to the facial, glossopharyngeal, and vagus nerves, providing taste sensitivity). Further, these centers regulate the functions of the structures involved in the swallowing process, such as the tongue, muscles of the larynx, pharynx, and upper esophagus. At the same time, the muscles of the tongue are controlled by the nucleus of the hypoglossal nerve; muscles of the larynx, pharynx and upper esophagus are controlled by n . a mbiguous (common for the vagus and glossopharyngeal nerves) [4, 7]. In patients with PD, the oropharyngeal phase of the act of swallowing is predominantly affected.
Function of the salivary glands in PD
Two causes of salivation in P.P. are actively discussed. One of them is a violation of the production of saliva, and the other reason may be its insufficient utilization. Overproduction of saliva can certainly cause salivation. However, many studies have shown [8, 9] that even less saliva is produced in patients with PD than in healthy people. The exact mechanisms causing the decrease in salivation remain unknown [10].
Decreased salivary secretion in PD may reflect involvement of the brainstem salivary nucleus, cranial autonomic ganglia. One possible explanation is a dopamine deficiency. Experimental studies in animal models have shown that dopamine modulates saliva secretion [11, 12]. Studies in rats have shown that activation of central and peripheral dopamine receptors induces salivation [11]. It is known that damage to the striatum, globus pallidus, and the descending pathway to the lateral part of the reticular formation of the midbrain can significantly reduce salivation [13]. Pathological anatomical studies revealed the presence of Lewy bodies in patients with PD both in vegetative formations (in the superior cervical ganglion, sympathetic trunk of the cervix, peripheral vagus nerve) and in the submandibular gland [14]. Despite the fact that Lewy bodies are found in the peripheral ganglia, involvement in the process of degeneration of the cranial parasympathetic ganglia has not been established. It has been confirmed that dopamine stimulates salivation, even against the background of administration of the peripheral D2-receptor blocker domperidone, which is indirect evidence of the involvement of higher levels of regulation in this system, including the basal ganglia and the brainstem, which may be responsible for reducing salivation in these patients [15] .
Studies of the intensity of production and the rate of excretion of saliva of the parotid glands by scintigraphy did not show a difference in the production of saliva, but the rate of saliva excretion to discrete stimuli in patients with PD was significantly higher compared to healthy ones [16, 17]. Thus, an increase in salivation does not make a major contribution to the pathophysiology of salivation in B.P. However, an increase in the rate of excretion partially increases sialorrhea.
In PD, the function of the hematosalivary barrier is impaired, its permeability to calcium, magnesium and zinc increases, and the concentration of copper in saliva decreases. Taking levodopa brings the permeability of the hematosalivary barrier closer to functional compliance with healthy ones [18]. Thus, dopamine regulation of not only the volume of secreted saliva, but also the ratio of its mucosal and serous components and elemental composition is not excluded.
Swallowing dysfunction may be one of the leading causes of salivation in PD patients. It is known that the dorsal motor nucleus of the vagus nerve is affected already in the early stages of PD, although other central regulators of swallowing remain intact for a long time. At the same time, the pedunculopontine nucleus of the tegmentum, which modulates the activity of the nuclei of the medulla oblongata, is also affected quite early in PD.
Double core regulates the function of the striated muscles of the pharynx and upper esophagus. The dorsal motor nucleus of the vagus nerve controls the intermuscular nerve plexuses of the smooth muscles of the esophagus. While the intermuscular nerve plexuses and the dorsal nucleus are affected at an early stage of PD, the pathology of the oral and pharyngeal stages in patients with PD at the onset of the disease is associated not with the involvement of the double nucleus, but with a violation of the supramedullary control of swallowing.
Oropharyngeal phase disorder found in PD may contribute to the accumulation of saliva in the oral cavity. Oropharyngeal dysphagia is thought to result from bradykinesia. Animal studies have shown that after injection of 6-hydroxydopamine (6-OHDA) in experimental rats, the rate of tongue protrusion slows down, and the average duration of tongue pressure becomes significantly longer compared to the control group [19]. Another study [20] showed that the maximum pressure of the tongue in patients with severe stages of PD was weaker compared to patients with initial or moderate stages, and the transit time of the food bolus in the oropharynx negatively correlates with the speed of tongue movement. Both studies reflect the fact that patients with PD have bradykinesia in the oropharyngeal phase of swallowing and dysfunction of the muscles of the tongue.
Thus, tongue control dysfunction contributes to dysphagia and possibly causes salivation. A videofluorographic study in modeling parkinsonism in rats (after an injection of 6-OHDA) showed a slower progression of the food bolus compared to the control group [21].
A study using barium in patients with drooling in PD demonstrated a direct correlation between the severity of dysphagia and the severity of sialorrhea [22]. Scintigraphy showed the presence of subclinical manifestations of dysphagia in all patients with sialorrhea. Patients’ complaints about salivation aggravated swallowing disorders [17]. Thus, oropharyngeal dysphagia may be the main pathophysiological factor in drooling in PD.
Another cause of drooling may be dysmotility of the upper esophagus. The data of the manometric study provided evidence of disturbances in the relaxation of the UES in patients with PD compared with the control group.
Often, a manifestation of PD is a violation of swallowing of a dystonic nature [23]. In this case, dysfunction of the pharyngeal-cricoid muscles leads to dysphagia. The pharyngocricoid muscles are the upper sphincters of the esophagus. Accordingly, impairment of their ability to adequately relax during swallowing may lead to impaired ability to swallow solid food. This condition is often called crico-pharyngeal achalasia and is characterized by insufficient relaxation of the upper esophageal sphincter in terms of duration and severity.
However, this factor cannot be the only cause of dysphagia, and if the patient has sufficient pharyngeal propulsion, swallowing will not suffer significantly [24, 25]. Probably, there is a combination of violations of the oropharyngeal and esophageal phases of swallowing.
Hypomimia, involuntary opening of the mouth, stoop or hanging head can also lead to saliva incontinence in the mouth [26]. At the same time, there is no evidence that drug-induced dyskinesias can cause salivation. Thus, today three main mechanisms of sialorrhea in PD are considered: increased secretion of saliva, inability to retain saliva in the oral cavity (hypomymia, involuntary opening of the mouth, stoop or hanging head), deterioration of salivary clearance (lingual bradykinesia, oropharyngeal dysphagia, dysfunction of the upper sphincter esophagus).
Epidemiology and maladaptation
On average, 50% of patients with PD complain of salivation, subclinical sialorrhea is objectified (videofluoroscopy) in 90% [2, 7]. Salivation is present in 86% of patients with dysphagia and only 40% without it [27].
Patients suffering from profuse salivation, have difficulty articulating speech and swallowing, have bad breath. The constant leakage of saliva from the oral cavity forces one to resort to the use of handkerchiefs or towels, leading to perioral cracking, irritation, and maceration of the skin. Wetting and soiling of clothes and bedding increases the burden on caregivers. Psychologically, excessive salivation can lead to low self-esteem and social isolation.
Methods of treatment
Treatment of sialorrhea in PD includes methods aimed at reducing saliva production with the appointment of acetylcholine transport blockers, cholinesterase inhibitors; the use of clozapine and quetiapine; improvement of motor symptoms of PD with dopaminergic agents and surgical neuromodulation. However, the effectiveness of these methods is only partial, and new pharmacological and non-pharmacological approaches to the treatment of sialorrhea are needed. For this purpose, various groups of drugs are being studied, including anticholinergics, adrenergic receptor antagonists, botulinum toxins (BTX).
Anticholinergics. Selective action requires blockers of M3-cholinergic receptors, predominantly localized in the salivary glands. Thus, side effects such as confusion, hallucinations, constipation, urinary retention, drowsiness can be avoided. For this purpose, sublingual atropine [28], sublingual ipratropine bromide spray [29], oral glycopyrrolate [30], oral tropical tropamide [31] were studied. According to the current MDS guidelines for the use of anticholinergic drugs for the treatment of salivation in PD, glycopyrrolate is effective, but proven efficacy persists for 1 week and there is insufficient data on its tolerability. There is also insufficient information on the efficacy and tolerability of ipratropin.
Adrenergic agonists may partially reduce sialorrhea. Clozapine, yohimbine, and α-2-adrenergic receptor antagonists have been described in the literature with salivation as a side effect. Based on this, α-2-adrenergic receptor agonists should reduce salivation. In particular, clonidine reduced sialorrhea in a small randomized, double-blind, placebo-controlled study involving 32 patients [32]. Oral modafinil 100 mg daily also reduces salivation. However, modafinil is an α-1-adrenergic receptor agonist, and the decrease in salivation is most likely due not to the suppression of saliva production, but to a decrease in dysphagia [32]. Thus, there are currently no recommendations for the use of α-2-adrenergic receptor agonists in the treatment of hypersalivation, but clonidine and modafinil can be considered as promising agents.
Botulinum Therapy
The main mechanism of action of BTX is the inhibition of the release of acetylcholine. Local injections into the salivary glands inhibit cholinergic parasympathetic and postganglionic sympathetic activity, causing a decrease in salivary secretion. Two serotypes of BTX are being studied to reduce sialorrhea: serotype A and serotype B. Two types of BTX type A, onabotulinumtoxin and abobotulinumtoxin, are used in the treatment of sialorrhea.
Studies on onabotulinum toxin of various designs were conducted (description of observations, open, open case-control, randomized placebo-controlled) [33-38]. In all these studies, injections were made into the parotid salivary gland. One of them [37] included patients not only with PD, but also with multisystem atrophy and dementia with Lewy bodies. Two studies [33, 36] used ultrasound guidance. One study [33] showed no difference in the effectiveness of injections with and without ultrasound guidance. The therapeutic effect was assessed after 1-16 weeks. BTX was administered in doses of 5 to 50 U into the parotid gland and 5 U into the submandibular gland with a significant decrease in salivation and an effect duration of up to 4 months.
Abobotulinum toxin (dysport) was injected into the parotid salivary gland in all studies. In some of them [39], BTX was additionally injected into the submandibular salivary gland. Most studies did not use additional methods of injection control. Only two of them [39, 40] used ultrasound guidance. The duration of the evaluation of the results ranged from 1 to 4 weeks. All studies have demonstrated the effectiveness of abobotulinum toxin at doses of 75-146.2 U when injected into each parotid and 78.7 U into each submandibular salivary gland. Salivation significantly decreased in patients not only with PD, but also with multisystem atrophy, corticobasal degeneration, and with amyotrophic lateral sclerosis [41]. Both according to objective assessment methods and subjective feelings of patients, the therapeutic effect persisted for 1-4 months. Additionally, it was found that there were no significant differences in therapeutic effects between drug injections into the parotid or submandibular glands [26].
BTX type B (rimabotulinum toxin, not registered in Russia) was also injected mainly into the parotid salivary gland [42-47], ultrasound guidance was used in two studies [31, 45]. All studies have proven the effectiveness of BTX type B at doses of 500-2000 and 250 IU when injected into the parotid and submandibular glands, respectively, with an average duration of effect of 4.8 months.
The objective of one of the studies was to compare BTX types B and A (randomized, placebo-controlled, cross-over, ultrasound-guided) [48]. Either 100 units of abobotulinum toxin or 1000 units of rimabotulinum toxin were injected into the parotid gland, either 25 units of abobotulinum toxin or 250 units of rimabotulinum toxin were injected into the submandibular gland. When evaluating salivation using the DSFS (Drooling Severity Scale and Frequency Scale) and DRS (Drooling Rating Scale) methods, 1 month after the injection, the result was better in the group that received BTX type B, but after 2 months the results were equal.
According to the MDS guidelines, BTX are effective in the symptomatic treatment of sialorrhea in PD [49]. The therapeutic effect begins 1 week after the injection and lasts 3-5 months. Ultrasound-guided injections may be more accurate. There were no differences in the effectiveness of BTX types, A and B. Typical side effects in the form of dry mouth are mild.
Cicopharyngeal dysphagia can also be successfully treated with BTX injections. Several injection techniques have been described, including both percutaneous and endoscopic techniques [50, 51]. The introduction of BTX type, A, 30 U in dysphagia into the pharynocricoid muscle under the control of electromyography and esophagoscopy leads to a decrease in swallowing disorders after 48 hours: swallowing function improves, hyperactivity of the pharynocricoid muscle decreases according to electromyography [52]. The dysphagia usually returns 22 weeks after the injection. During these weeks of improvement in swallowing, patients regain the lost body weight [51, 53]. This fact is important in improving the quality of life of patients.
Non-pharmacological treatments
Various non-pharmacological treatments are offered, such as chewing gum, behavior modification, radiotherapy, and surgery. However, only 2 studies on this topic have been published. L. Marks et al. [54] conducted a randomized placebo-controlled trial involving 6 patients with BP. Patients were required to perform voluntary swallowing every time they heard a sound. This modified behavior resulted in a significant reduction in sialorrhea as measured by DRS. At the same time, the results, which reached a maximum after 1 month after training, turned out to be minimal after 3 months. The authors concluded that patient motivation and voluntary control of swallowing should be taken into account and used in the treatment of patients with sialorrhea.
Another study used bilateral 12 Gy radiotherapy to the parotid and upper submandibular glands [5]. Hypersalivation significantly decreased after 1 month after radiotherapy, and the effect persisted up to 1 year. The most commonly reported adverse events were decreased taste and dry mouth. However, 75% of adverse events were transient.
We did not find any studies on the effect of surgical neuromodulation in the literature. It is possible that in some cases, when chronic stimulation of the basal ganglia causes deterioration in swallowing, salivation may increase [56]. A recent study [57] showed an adverse effect of bilateral stimulation of the subthalamic nucleus.
The conclusion can be considered the statement that there are no current recommendations on the use of non-pharmacological methods in the treatment of sialorrhea in B.P. However, behavior modification and, in refractory cases, radiotherapy can be considered as additional components of the overall therapy package.
In conclusion, salivation causes negative consequences for the life of both PD patients and their caregivers. While it is probably not overproduction of saliva that plays the leading role in sialorrhea, but swallowing disorders, most treatments are aimed at reducing secretion. Botulinum toxin injections into the major salivary glands are currently the most effective treatment. The issues of the pathophysiology of ptyalism, the standardization of diagnostic criteria, methods for assessing severity, and the development of a strategy for the treatment of sialorrhea in PD require further study.
Causes of profuse salivation in a child
If the child is a year old, profuse salivation is considered normal. All this will pass as soon as he grows up. However, in older children, hypersalivation may indicate the development of an unpleasant disease. The article discusses the causes that cause profuse salivation.
False hypersalivation
Abundant salivation in a child who goes to kindergarten or school can adversely affect social adaptation. The fact is that other children, as a rule, begin to tease, and this will inevitably lead to mental disorders and, accordingly, aggravate the situation.
But before taking action, it is important to see a doctor. Only he can correctly diagnose. The fact is that hypersalivation is false. Most often, it is provoked by injuries of the tongue, inflammatory processes in the oral cavity or bulbar nerve fibers. These pathologies reduce the swallowing function, so it may seem that there is more saliva than usual. Everything returns to normal once the root cause problem is resolved. In the case of false hypersalivation, profuse salivation is a consequence of the disease.
Causes of excessive salivation in a child
Hypersalivation can develop in children of any age. Doctors believe that it can be provoked by:
- Physiological changes. There are no deviations from the norm or pathologies in this process. These changes include adolescence with hormonal changes and the appearance of the first teeth.
- Pathologies of complex genesis. These reasons can have serious consequences. If a child is diagnosed with swallowing disorders, neurological diseases, rickets, inflammation of the nerves, muscle paralysis, then it is necessary to constantly be observed by a doctor.
Only a specialist can determine the exact cause. To make a diagnosis, he will need not only to examine the child, but also to know the full clinical picture. How does pathology manifest itself, what features does it have? Parents can answer these questions. And, of course, you will need an examination and testing.
Physiological changes
As mentioned above, physiological changes occurring in the body are considered normal. Abundant salivation in a child of 2 months and up to a year, as well as in adolescents, should not cause concern to parents. Of course, it is necessary to observe in order not to miss the development of any pathology. Let’s look at when hypersalivation is considered the norm.
Teething
As you know, newborn babies do not have teeth. They begin to erupt at about 3 months. Abundant salivation in a child for this reason can last up to 18 months. Why is teething accompanied by increased salivation? The human body is designed in a special way. It has a self-protection function. It is she who causes profuse salivation at the time of teething.
When a tooth breaks through the gum, a small wound forms. And saliva flushes it out so that an infection does not develop. In scientific language, this is called internal sanitation of the oral cavity.
In addition to a large amount of saliva, the child also has other symptoms:
- loss of appetite;
- fever;
- capricious behavior;
- decreased activity, fatigue.
Hormonal changes
Why did my child start salivating profusely at the age of 12? This question worries many parents. And the answer is simple. It is at this age that hormonal changes begin. Girls get their period and boys ejaculate in the morning. It is these factors that indicate that their body is preparing for adulthood.
Many parents think that adolescence is 15-16 years old. But it’s not. The restructuring of metabolic processes begins 3-4 years earlier. During this period, in addition to an increased amount of saliva, acne and sweating are also observed.
In order to help a teenager to more easily endure these changes, you will need to contact a specialist. He will tell you how to properly care for your body, select a balanced diet and prescribe homeopathic remedies. As soon as the hormonal background stabilizes, hypersalivation will disappear on its own.
Inability to swallow saliva
This pathology is rarely diagnosed. May occur in a child as young as 2 years old. Abundant salivation, drinking avidly, uncontrolled appetite, problems with breastfeeding – all these symptoms indicate that the baby does not know how to swallow saliva. If the pathology is detected in time and therapy is started immediately, then it will be possible to get rid of the problem by 3-4 years.
Diseases of the oral cavity
Unfortunately, small children, getting to know the world around them, put all objects into their mouths. This inevitably leads to the development of unpleasant diseases. The most common is stomatitis. Also, excessive salivation in a child at the age of 3 can cause spastic disorders, neurological abnormalities, and inflammation of the glossopharyngeal nerve.
The parent can independently determine the development of such pathologies. It is necessary to regularly examine the oral cavity. If the child has reddened, a white coating and swelling have appeared, then it is important to immediately consult a pediatrician. Neurological disorders are manifested by frequent convulsions, lethargy, and a sluggish reaction to everything that happens around. Due to the fact that such a child has a developmental delay, he cannot swallow saliva, so it will flow profusely from the mouth. With such a problem, you need to make an appointment with a neurologist.
Rickets
Abundant salivation in a child may appear if he has a lack of elements such as phosphorus and calcium. The disease is referred to as rickets. It has many unpleasant symptoms and is aggravated by serious consequences. The child, in addition to profuse salivation, will also suffer from excessive sweating, arrhythmias, problems with the gastrointestinal tract, and baldness. In addition, over time, the size of the abdomen and head increases, and the spine and legs are strongly curved. If at the initial stage a medical correction is carried out, then the general condition of the child will improve, and the bones will get stronger.
Poisoning
The most dangerous cause of excessive salivation in a child is poisoning. It is important to understand that it can lead to serious consequences or even death. Parents need to keep an eye on their children, especially if substances such as pesticides, iodine, thinner, mercury, liquid bleach, and others are stored at home. In no case should you self-medicate. If there is a suspicion of poisoning with a potent substance, call an ambulance. Only doctors will be able to determine the severity and decide whether there is a need for hospitalization. Symptoms that occur after taking a harmful substance are vomiting, excessive salivation, nausea, loose stools, weakness, pallor of the skin.
Factors
Thus, it is possible to identify the main causes that can provoke excessive salivation in a child. Some of them have already been described above. The process of eruption of milk teeth is considered the most harmless. The greatest amount of saliva is formed in the period from 4 to 7 months. There are no pathologies in this, this is how the body reacts to this process.
But if profuse salivation has begun in a child aged 2 years and older, then it is necessary to check the oral cavity for the formation of infectious wounds and inflammatory processes. The most common cause of this pathology is stomatitis. With it, the mucosa is damaged, which provokes an increase in the amount of saliva. Another disease is gingivitis. It is diagnosed in those children who have inflamed gums. In this case, excessive salivation is not a symptom, but simply a defensive reaction.
This problem also occurs in cases of parasitic infestation (clay infestation). In order to get rid of the increased separation of saliva, it is necessary to treat the underlying pathology. Also, children diagnosed with cerebral palsy or colds suffer from hypersalvation.
What to do
Abundant salivation in a child 2 months and older can be both a norm and a deviation. It is from this that we must build on, deciding what to do when we find such a problem. If the reasons are related to physiological changes, then parents do not need to worry. Everything will pass by itself. But in the case of a disease, a symptom of which is an abundant separation of saliva, it is urgent to make an appointment with a doctor, and in some situations, call an ambulance.
It will take no more than ten minutes for the doctor to confirm hypersalvation. If there is a suspicion of a specific disease, then an examination by a highly specialized specialist, for example, a dentist, a neuropathologist, is additionally prescribed. The latter will not only make an accurate diagnosis, but also prescribe an effective treatment. Alternatively, anticholinergics may be prescribed. They are designed to reduce the activity of the nervous system. Thanks to the intake of such drugs, its effect on the mucous membrane is reduced, respectively, the amount of saliva will decrease.
In case of nervous disorders, drug therapy is supplemented with special therapeutic exercises and homeopathic preparations with anthropin. Facial massage also gives good results. It relaxes muscle tension. In rare cases, radiation therapy may be prescribed.
If it is not possible to find out the cause of excessive salivation, and the chin and skin around the face are reddened and painful to the touch, then it is recommended to use ointments or creams.