






Tylenol or motrin for teething: Tips for Teething Pain: What’s Safe—and What’s Not
Tips for Teething Pain: What’s Safe—and What’s Not
Advice From Our Experts
August 5, 2020
Special thanks to Marie Lafortune, MD, Attending Physician in the Division of General Pediatrics at Children’s Hospital Los Angeles, for contributing to this article.
Teething can be tough on babies—and their parents. It hurts to have those new teeth grow in, and that can lead to a lot of crying, sleepless nights and frustration.
What can you do to make it better? Here’s what you need to know about teething, including what’s safe—and not safe—to give your baby.
When does teething start—and end?
In general, teething starts around 6 months of age, but it varies. It can begin anytime from 6 to 12 months.
Your child will be getting new teeth, off and on, for a couple of years. The two sets of front teeth—typically bottom and then top—come in first. The molars (in the back of the mouth) are the last to appear, sometime between the ages of 1 and 3 years. These tend to be more painful.
Signs and symptoms
- Fussiness and crying. Teething hurts! Your baby has good reason to be fussy, irritable and quick to cry.
- Drooling. Teething stimulates saliva—and drooling. Many babies drool a lot! There isn’t much you can do about this. Just stock up on bibs, and keep your child’s mouth and face as clean and dry as possible.
One note: Many babies drool even before their first teeth come in. Just because you see drooling doesn’t mean your baby is teething.
- Putting things in their mouth. Babies like to do this regardless, but those who are teething will often bite or gnaw on things to ease gum pain.
- Low-grade fever. Teething can sometimes cause a very mild, low-grade fever. Higher fevers—101 F or above—are not caused by teething.
Best remedies for teething pain
- Something cold. Keep a clean, damp washcloth or small damp towel in the fridge.
 Once it’s cold, give it to your baby to hold and gnaw on. (You can knot one end to make it easier.) This is very soothing for sore gums.
Once it’s cold, give it to your baby to hold and gnaw on. (You can knot one end to make it easier.) This is very soothing for sore gums.
 Once it’s cold, give it to your baby to hold and gnaw on. (You can knot one end to make it easier.) This is very soothing for sore gums.
Once it’s cold, give it to your baby to hold and gnaw on. (You can knot one end to make it easier.) This is very soothing for sore gums.Teething rings are also a good option. They should be made of firm rubber. Put the ring in the fridge and give it to your child cold. Do not put it in the freezer—this makes it too hard and too cold.
- Massage. Teething causes gums to be swollen and tender. Using a clean finger, gently rub or massage your baby’s gums for a minute or two to relieve discomfort.
- Pain medicine. The safest choice is acetaminophen (Tylenol) for babies 2 months and older. Ibuprofen is not recommended for children until they are at least 6 months of age. Follow the directions on the label for your child’s age and weight.
- Lots of cuddling and rocking. This really does help!
What to avoid
Many products sold for teething pain don’t work—and some can even hurt your baby. Stay away from:
- Teething necklaces. The Food and Drug Administration issued a warning against these necklaces in December 2018. The beads can break off, and your child could choke on them. Plus, the necklace can get caught on something and strangle your child. (A reminder: Babies should never wear any jewelry!)
- Frozen teething rings. As noted above, these become too hard and cold and can harm your baby’s gums.
- Topical gels. Many gels were taken off the market in 2018 because they contained benzocaine, which is not safe for children under age 2. What about gels without benzocaine? It’s best to pass on these; you can’t truly be sure what’s in them. Besides, remember all that drool? Gels wash away too quickly to have much of an effect.
- Teething tablets. Some tablets contain belladonna, which is toxic in high enough amounts. There have been cases where teething tablets contained more belladonna than stated on the label. Avoid these tablets.
 The Food and Drug Administration issued a warning against these necklaces in December 2018. The beads can break off, and your child could choke on them. Plus, the necklace can get caught on something and strangle your child. (A reminder: Babies should never wear any jewelry!)
The Food and Drug Administration issued a warning against these necklaces in December 2018. The beads can break off, and your child could choke on them. Plus, the necklace can get caught on something and strangle your child. (A reminder: Babies should never wear any jewelry!)When to call the doctor
Teething is a normal—and luckily, temporary—part of baby and toddler life. That said, you know your child best. Be sure to talk to your pediatrician if you feel anything is amiss. Symptoms like high fevers, cough, runny nose and diarrhea are most likely not caused by teething, but by another illness. You should also talk to your doctor if your child hasn’t gotten their first tooth by 16 months of age. When in doubt, see the doctor to check it out.
That said, you know your child best. Be sure to talk to your pediatrician if you feel anything is amiss. Symptoms like high fevers, cough, runny nose and diarrhea are most likely not caused by teething, but by another illness. You should also talk to your doctor if your child hasn’t gotten their first tooth by 16 months of age. When in doubt, see the doctor to check it out.
How Often, Dose, When to Give
You’ve heard that the teething stage is bad, but is it really? Like, can’t you just give a baby a teether or a cold washcloth and move on?
Well — not always. Sometimes teething pain is bad enough to warrant some medicinal relief — and Tylenol is often considered the go-to option, as it’s generally safe for young babies.
But since teething can last a long time (read: months and months on end), you can’t keep your child on a 24/7 infusion of infant Tylenol. Here’s how to know when to give it to your baby, how to use it safely, and how it stacks up against other pain relief options.
You might not remember what it felt like when your 6-year molars or wisdom teeth came in, but let us assure you: Yes, teething is uncomfortable!
To be clear, it might not cause “pain” in the traditional definition of the word. Some experts think teething causes a dull, achy sensation, or possibly even an itchy one — which is why babies turn to chomping and gnawing during the worst bouts of teething in an attempt to soothe their irritated gums.
Some babies are hardly bothered by teething, while others seem more acutely affected. Either way, it’s reasonable to assume your baby will notice something going on in their mouth — and may not like the feeling.
Since babies can’t tell you how they’re feeling, it can be hard to know if or when they’re in pain. But some common symptoms that your baby isn’t feeling well include:
- unusual fussiness or irritability
- extreme clinginess (i.e., not wanting to be put down)
- difficulty sleeping at naps or bedtime
- pulling on their ears
Specific to teething woes, you might also notice an increase in the amount of drooling your baby is doing — hello, 10 bibs per day! — along with sore or swollen gums and a desire to chew on everything within reach.
Some parents think teething can cause fevers, but this isn’t quite true: While teething can increase your child’s body temperature a smidge, it shouldn’t cause a true fever like the kind that could occur with illness.
Officially, the makers of Tylenol advise that parents talk with doctors about medicating kids under 2 years old. We concur — but according to the American Academy of Pediatrics (AAP), you can use your child’s weight to determine the correct dosage if they’re more than 3 months old.
Since teething typically starts between 4 and 6 months, you can give teething babies Tylenol safely.
You can — and should! — always talk with a doctor about the right dosage for your baby’s weight if they’re under 2 years old. These are the general recommendations about dosing based on weight, which may act as a starting point for the conversation with a doc.
- Whether you buy an infant or children’s formula, liquid medication, or tablets, all pediatric Tylenol now contains the same strength of medication per dose: 160 milligrams. This standardization simplifies dosing. For liquid medication, which you’ll likely give your baby, this equals 5 milliliters (mL).
- For infants between 6 and 11 pounds, the typical dosage is 1.25 mL according to the AAP. The dose increases by about 1.25 mL from there for every 5 pounds in weight.
- Older babies may be able to take a chewable or dissolvable tablet, but that’s child-dependent. You can give your child liquid medication when they’re any age.
- You can give your child a new dose every 4 to 6 hours as needed, but you shouldn’t give them more than 5 doses in a 24-hour period, per the AAP.
- It might be better to use Tylenol for teething relief at night or before long naps to distract your child from their discomfort. During the day, you can try to rely on teethers to distract them from the pain. Talk with your pediatrician about giving your child a dose 1 hour before going to sleep, so it’s working in the full effect by bedtime or naptime.
- Remember to always use the measuring device that comes with your package of Tylenol. It’s guaranteed to give you an accurate amount of medication. Other devices may not be standardized to Tylenol’s measuring system.
 This standardization simplifies dosing. For liquid medication, which you’ll likely give your baby, this equals 5 milliliters (mL).
This standardization simplifies dosing. For liquid medication, which you’ll likely give your baby, this equals 5 milliliters (mL). It’s guaranteed to give you an accurate amount of medication. Other devices may not be standardized to Tylenol’s measuring system.
It’s guaranteed to give you an accurate amount of medication. Other devices may not be standardized to Tylenol’s measuring system. In babies more than 6 months old, Motrin is also an option for teething pain relief. Tylenol is often recommended as the first line of defense since you can give it to younger babies and Motrin may cause an upset stomach in some kids.
Tylenol may be tolerated better by your little one, but there’s no major difference in effectiveness in treating teething pain with either medicine. It just comes down to your baby’s age and how well they respond to the active ingredient.
Wondering what you can do instead of — or along with — giving your baby another dose of Tylenol to help them feel better? There are a few good at-home teething remedies, like:
- offering them teething toys
- letting them chew on a cold washcloth or baby toothbrush
- giving them cool, soft foods to eat, like fruit puree in a mesh feeder (if they’re eating solids)
You can use these at-home remedies as often as necessary, especially if it reduces your need to rely on Tylenol to soothe teething pain. But you should avoid the following remedies to treat your baby’s discomfort, since pediatricians don’t consider these to be safe options:
But you should avoid the following remedies to treat your baby’s discomfort, since pediatricians don’t consider these to be safe options:
- topical teething gels
- homeopathic teething tablets
- amber teething necklaces
The good news is you can manage teething pain at home with a combination of natural remedies and over-the-counter (OTC) infant pain relievers after getting a doctor’s advice on dosing. Teething isn’t something that typically requires a pediatrician appointment.
Certainly, you can give your doctor a call for advice if you’re:
- having a difficult time handling your child’s teething
- feeling like they need pain relief from Tylenol frequently
- wondering what you can do to help
It’s also possible there could be something else going on besides teething. So, if your child seems inconsolable, it’s smart to check in with the pediatrician.
Tylenol, with a 160mg/5mL strength and dosed based off of weight, is generally okay for babies.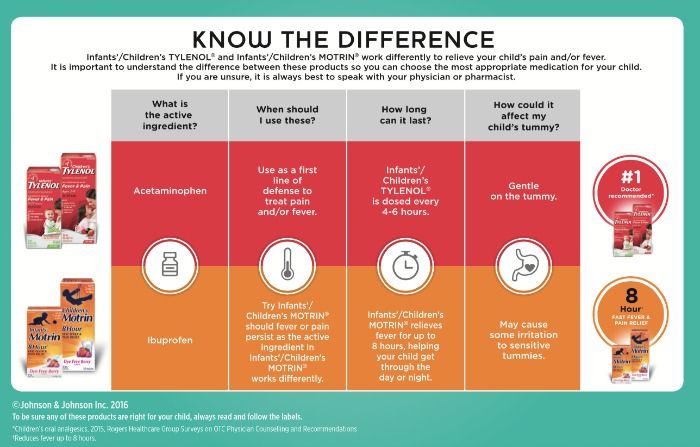 Be sure to ask your doctor for dosing recommendations.
Be sure to ask your doctor for dosing recommendations.
Ibuprofen versus paracetamol (acetaminophen) for pain relief after surgical removal of lower wisdom teeth
Review question
This review by the Cochrane Oral Health Group compared the effectiveness of two commonly used pain relievers, paracetamol and ibuprofen, alone and as a single tablet combination, in relieving pain after surgical removal of lower wisdom teeth.
Relevance
A huge number of wisdom teeth surgeries are performed worldwide, with approximately 63,000 extractions performed annually in England alone in National Health Service (NHS) hospitals. This significantly affects the quality of life of patients and many patients need a break from work. However, despite these consequences, people are most often worried about pain after surgery, which can be very severe. It is assumed that the most pronounced pain is felt three to five hours after surgery. Pain experienced after oral surgery is widely used as a model for measuring the effectiveness of pain medications in general.
Paracetamol and ibuprofen are often used to relieve pain after surgical removal of lower wisdom teeth. In 2010, a new pain reliever (branded as Nuromol) containing paracetamol and ibuprofen in one tablet was licensed for use in the UK.
All drugs studied in this review produced minimal side effects when used correctly for short-term pain relief.
Study profile
The evidence in this review is current to 20 January 2013. This review included seven studies involving 2241 people that directly compared ibuprofen and paracetamol or a combination of the two. All participants underwent mandibular or wisdom teeth extractions that required partial bone removal or caused at least moderate or severe pain. The studies compared painkillers at different doses taken after surgery.
Most of the studies were conducted in the USA and one study was conducted in Puerto Rico. Four of the clinical trials were conducted at clinical research institutions, two at university dental hospitals, and one at a private dental surgery clinic. The age of the participants varied slightly across the studies, but was generally similar and ranged from 15 to 65 years. All studies involved men and women.
The age of the participants varied slightly across the studies, but was generally similar and ranged from 15 to 65 years. All studies involved men and women.
All studies included in this review only looked at information on pain relief and pain intensity after a single dose of pain medication after surgery. Pain is known to continue afterward, and the drugs studied in this review are typically administered every six to eight hours (maximum four times a day).
Main results
Ibuprofen was more effective than paracetamol at all doses studied in this review. Based on limited evidence, the combination of paracetamol and ibuprofen was no more effective than either drug alone when assessed two hours after surgery. However, again based on limited evidence, the combination of these drugs was more effective than their use alone when assessing the effect six hours after surgery. Participants who took the combination remedy were less likely to require emergency medicines.
Available information on adverse events in the studies (including nausea, vomiting, headaches and dizziness) indicated that they were comparable between treatment groups. However, the review authors were unable to formally analyze the data because they could not figure out how many adverse events there were.
Quality of evidence
All results (outcomes) comparing ibuprofen with paracetamol were of high quality. This means that further research is unlikely to change our confidence in the estimate of the effect.
When comparing the combination with drugs alone, the quality of the evidence for the proportion of patients with >50% maximal pain relief at two and six hours was rated as moderate due to inaccurate estimates based on single studies. This means that further research is likely to significantly affect our confidence in the estimate of the effect. The quality of the evidence for emergency drug use was rated as high.
If you found this evidence helpful, please consider donating to Cochrane. We are a charity that produces accessible evidence to help people make health and care decisions.
We are a charity that produces accessible evidence to help people make health and care decisions.
Donate
Translation notes:
Translation: Tashtanbekova Cholpon Bolotbekovna. Editing: Yudina Ekaterina Viktorovna. Project coordination for translation into Russian: Cochrane Russia – Cochrane Russia (branch of the Northern Cochrane Center on the basis of Kazan Federal University). For questions related to this translation, please contact us at: [email protected]; [email protected]
🎖▷ Why You Shouldn’t Worry About Weight Gain With Lamictal
If you’re worried that taking Lamictal (lamotrigine) might cause weight gain, there’s good news. It probably won’t affect your weight much. If anything, you’re more likely to lose weight due to Lamictal than gain weight, but either way, the changes are likely to be pretty small.
The effect of Lamictal on weight has been little studied and various clinical trials have found minimal effect. In fact, some researchers even considered the drug as a possible remedy for obesity and as a remedy for overeating. This information should be reassuring for people with bipolar disorder, as many of the medications used to treat this condition can cause weight gain.
In fact, some researchers even considered the drug as a possible remedy for obesity and as a remedy for overeating. This information should be reassuring for people with bipolar disorder, as many of the medications used to treat this condition can cause weight gain.
Findings on Lamictal and weight gain or loss
Lamictal is an anticonvulsant that can be used to treat seizures such as epilepsy. It is also used as a mood stabilizer for bipolar disorder.
In the first clinical trials with the drug, 5 percent of adults with epilepsy lost weight while taking Lamictal, while 1 to 5 percent of patients with bipolar I disorder gained weight while taking the drug. The researchers do not disclose how much weight patients have gained or lost.
Meanwhile, a 2006 study comparing the effects on weight of Lamictal, lithium, and placebo found that some Lamictal-treated patients gained weight, some lost weight, and most remained about the same weight. Weight changes are usually not many pounds anyway. Obese patients taking Lamictal lost an average of four pounds, while the weight of non-obese patients remained virtually unchanged.
Obese patients taking Lamictal lost an average of four pounds, while the weight of non-obese patients remained virtually unchanged.
Relationship between weight gain and other bipolar drugs
Weight gain from medications used to treat bipolar disorder is unfortunately quite common. Some mood stabilizers commonly used for bipolar disorder, especially lithium and Depakote (valproate), carry a high risk of weight gain.
In addition, the atypical antipsychotics Clozaril (clozapine) and Zyprexa (olanzapine) tend to cause significant weight gain in people who take them. Finally, some antidepressants, notably Paxil (paroxetine) and Remeron (mirtazapine), have been associated with weight gain.
Therefore, if you are already overweight, you and your psychiatrist may want to consider additional weight gain when determining your bipolar medication regimen. Based on this, Lamictal may be a good choice.
Lamictal as a possible treatment for obesity
Lamictal has also been studied as a possible treatment for obesity in people without epilepsy or bipolar disorder.
In a small 40-person clinical trial conducted in 2006, researchers randomly assigned participants to receive either lamictal or placebo for up to 26 weeks. Each participant in the study had a body mass index (BMI) between 30 and 40, placing them in the obese group to the level of severe obesity. Those who took Lamictal lost an average of just over 10 pounds. Those who took the placebo lost about 7 pounds in the meantime, so while those who took Lamictal lost more weight, they didn’t lose all that much more.
Another study in 2009 looked at Lamictal as a remedy for overeating. This study involved 51 people with the condition that 26 of them received Lamictal, and 25 – placebo.
Those who took Lamictal lost more weight than those who took placebo (about 2.5 pounds vs. about one third of a pound) and did have significant improvements in blood sugar and cholesterol lab test results. However, Lamictal did not appear to affect other aspects of the eating disorder when compared to placebo.