






I am five and 3 days pregnant and seen only yolk sac fetal pole not visible: Abnormal Ultrasound in Early Pregnancy
Abnormal Ultrasound in Early Pregnancy
« Back to Articles
Dr. Vishvanath Karande
Jul 03
227 Comments
In a previous blog we discussed the expected ultrasound findings in a normal intrauterine pregnancy. Variations from the expected pattern of development are worrisome or, if major, definitive for early pregnancy failure or miscarriage. These were discussed in a recent review article by Doubilet et al. (N Engl J Med 2013;369:1443-51). Here is a summary:
The criteria most often used to diagnose pregnancy failure are the absence of cardiac activity by the time the embryo has reached a certain length (crown–rump length), the absence of a visible embryo by the time the gestational sac has grown to a certain size (mean sac diameter), and the absence of a visible embryo by a certain point in time.
Crown-rump length (CRL)
A crown–rump length of 5 mm was widely recommended as a positivity criterion for diagnosing failed pregnancy when no cardiac activity is seen. Recent studies have shown that a 5-6 mm cutoff can result in a false positive diagnosis of pregnancy failure. It is now recommended that we use a 7 mm (rather than 5 mm) cut-off for diagnosing failed pregnancy. Thus if the crown-rump length is 7 mm and there is no heart beat visible, it is suspicious for a failed pregnancy.
Gestational sac diameter
It is prudent to use a cutoff of 25 mm (rather than 16 mm) for the mean sac diameter with no visible embryo in diagnosing failed pregnancy (see figure above). This would yield a specificity and positive predictive value of 100% (or as close to 100% as can be determined). When the mean sac diameter is 16 to 24 mm, the lack of an embryo is suspicious for, though not diagnostic of, failed pregnancy
Time based criteria for failed pregnancy
Not all failed pregnancies ever develop a 7-mm embryo or a 25-mm gestational sac, so it is important to have other criteria for diagnosing pregnancy failure. The most useful of such criteria involve non visualization of an embryo by a certain point in time. An alternative approach to predicting pregnancy failure, based on subnormal growth of the gestational sac and embryo, has been shown to be unreliable. Non visualization of an embryo with a heart- beat by 6 weeks after the last menstrual period is suspicious for failed pregnancy, but dating of the last menstrual period (in a pregnancy conceived without medical assistance) is too unreliable for definitive diagnosis of pregnancy failure.
An alternative approach to predicting pregnancy failure, based on subnormal growth of the gestational sac and embryo, has been shown to be unreliable. Non visualization of an embryo with a heart- beat by 6 weeks after the last menstrual period is suspicious for failed pregnancy, but dating of the last menstrual period (in a pregnancy conceived without medical assistance) is too unreliable for definitive diagnosis of pregnancy failure.
The timing of events in early pregnancy — gestational sac at 5 weeks, yolk sac at 5 ½ weeks, and embryo with heartbeat at 6 weeks — is accurate and reproducible, with a variation of about ± ½ week; this consistency explains the time-related criteria for pregnancy failure. For example, if the initial ultrasonogram shows a gestational sac with a yolk sac and a follow-up scan obtained at least 11 days later does not show an embryo with cardiac activity, the diagnosis of failed pregnancy is established.
According to the Society of Radiologists in Ultrasound Multispecialty Consensus Conference on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy, October 2012; the following are guidelines for Transvaginal Ultrasonographic diagnosis of Pregnancy Failure in a Woman with an Intrauterine Pregnancy of Uncertain Viability.
Findings Diagnostic of Pregnancy Failure
- Crown–rump length of ≥7 mm and no heartbeat
- Mean sac diameter of ≥25 mm and no embryo
- Absence of embryo with heartbeat ≥2 wk after a scan that showed a gestational sac without a yolk sac
- Absence of embryo with heartbeat ≥11 days after a scan that showed a gestational sac with a yolk sac
Findings Suspicious for, but Not Diagnostic of, Pregnancy Failure
- Crown–rump length of <7 mm and no heartbeat
- Mean sac diameter of 16–24 mm and no embryo
- Absence of embryo with heartbeat 7–13 days after a scan that showed a gestational sac without a yolk sac
- Absence of embryo with heartbeat 7–10 days after a scan that showed a gestational sac with a yolk sac
- Absence of embryo ≥6 wk after last menstrual period
- Empty amnion (amnion seen adjacent to yolk sac, with no visible embryo)
- Enlarged yolk sac (>7 mm)
- Small gestational sac in relation to the size of the embryo (<5 mm difference between mean sac diameter and crown–rump length)
When there are findings suspicious for pregnancy failure, follow-up ultrasonography at 7 to 10 days to assess the pregnancy for viability is generally appropriate. Treatments for early miscarriage are discussed here.
Treatments for early miscarriage are discussed here.
To see a fertility specialist who is a board-certified physician with high success rates, make an appointment at one of InVia’s four Chicago area fertility clinics.
What to Expect, What You’ll See, and More
If you’re 5 weeks pregnant, you’re undergoing some major changes.
But you likely won’t notice any differences to your body on the outside. On the other hand, your body is already working to nurture a growing embryo, which is quickly developing important things like the brain, heart, spinal cord, and blood vessels.
It’s normal to want to get a glimpse of your baby as soon as you can. With that being said, if you haven’t had previous complications in pregnancy and you’re relatively healthy, it’s better to wait until at least 12 to 14 weeks into pregnancy to schedule your first ultrasound. This is because it’s too early to see the baby’s limbs and organs before this point.
In fact, at 5 weeks, you’ll likely only see the yolk sac and the gestational sac — and many not even that. What you don’t see may unnecessarily worry you, but it’s perfectly normal.
What you don’t see may unnecessarily worry you, but it’s perfectly normal.
Some women may get an early ultrasound during their first trimester to estimate the age of the gestational sac, which usually becomes visible in an ultrasound during the fifth week.
If you have a history of ectopic pregnancy or miscarriage, or if you’ve conceived via in vitro fertilization, your doctor may also want you to have an early ultrasound. In addition, bleeding after a positive pregnancy test might warrant a look at your uterus.
If you’re 5 weeks pregnant, your ultrasound will be done via the vagina as opposed to transabdominal ultrasounds that are typically performed later on in pregnancy.
During a transvaginal ultrasound, a lubricated wand is inserted into your vagina and images translate back to a screen. It shouldn’t be painful, but it may be a little uncomfortable.
Don’t be worried if you can’t see your baby! The embryo is only the size of a peppercorn right now — about 2 millimeters (mm).
At this stage, the only things you’ll likely see are the yolk sac and the gestational sac.
It’s possible that the sonographer might be able to point out the embryo, which at this stage is likely a tiny white curled object.
Surrounding the embryo is the yolk sac, which will look like a small white circle. The yolk sac nourishes the embryo and also helps produce blood cells during the early stages of pregnancy.
The yolk sac is surrounded by a larger black area, known as the gestational sac. The gestational sac contains amniotic fluid and surrounds the embryo. You may see the gestational sac in an ultrasound as early as 4 1/2 to 5 weeks.
The gestational sac increases in diameter by 1.13 mm per day and initially measures 2 to 3 mm in diameter, according to the National Center for Biotechnology Information.
You may get to see the flicker of a little heartbeat, but again, don’t stress if the sonographer can’t see it yet. It’s more common to see the heartbeat at 6 weeks or even later.
Patience is key during pregnancy. Some women may go in for a 5-week ultrasound only to hear that their gestational sac isn’t showing up yet.
There are a few possibilities as to why the gestational sac doesn’t show up during a 5-week ultrasound.
It’s too early
You may have counted the days incorrectly if you’re unable to see the gestational sac. Something as simple as getting the dates wrong may be the reason why you don’t see anything during a 5-week ultrasound.
This is common and has everything to do with your human chorionic gonadotropin (hCG) levels. HCG is the same hormone that confirms pregnancy from urine on a pregnancy test.
Your hCG levels should be around 1,500 to 2,000 at 5 weeks pregnant, but it may be difficult to see anything until hCG exceeds 2,000.
Ectopic pregnancy
An ectopic pregnancy may be the reason why you don’t see anything during a 5-week ultrasound. This is less common than having the dates wrong and may be life threatening if not treated.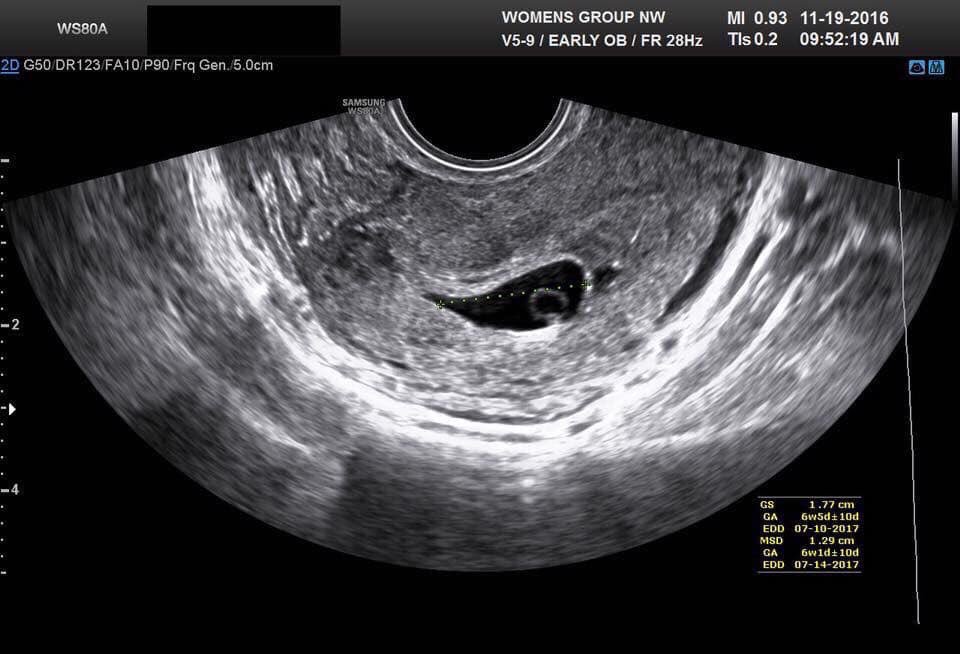
An ectopic pregnancy happens when fertilized eggs implant and grow on the outside main cavity of the uterus. These pregnancies require treatment and may cause heavy bleeding inside the abdomen. Most ectopic pregnancies occur in a Fallopian tube.
See your doctor if you notice any vaginal bleeding or pain in the pelvic area while pregnant.
Miscarriage
Falling hCG levels and the inability to find a gestational sac may also point to an early miscarriage. A miscarriage happens when a fertilized egg doesn’t form properly form an embryo.
Vaginal bleeding is a common sign of a miscarriage but isn’t a unique symptom for miscarriages — vaginal bleeding may mean something else in your pregnancy.
In more rare cases, miscarriages may occur because of problems with your uterus or cervix. See your doctor if you have questions or concerns about miscarriage.
Pregnancy symptoms are impacted by your hCG levels. Common symptoms during the fifth week of pregnancy include:
- metallic taste in your mouth
- tender breasts
- morning sickness
- mood swings
- unusual pregnancy cravings
- constipation
- expanded sense of smell
- increased urination
- white vaginal discharge
- light spotting
- abdominal cramps
- thicker and shinier hair
- bloating
- missed period
You may want to wait a couple of weeks to get your first ultrasound to increase the chances of seeing the gestational sac and embryo.