C section pain 6 months after: 9 Things No One Tells You About C-Section Recovery — Baby2Body
9 Things No One Tells You About C-Section Recovery — Baby2Body
About one-third of all US births are delivered by a Cesarean section and in the UK it’s approximately one-quarter. Are you surprised by those stats? The growth rate of C-sections has rapidly increased over the last few decades and since 1990 reports indicate that the rates have tripled.
Whether you are electing to have a C-section or if it happens as an emergency, you deserve to feel supported and know what to expect once you go home. However, we have discovered that so many women are not prepared for what the C-section recovery process involves. If you’ve been to an antenatal class, you’ll know that they are primarily focused on vaginal deliveries and the consequent recovery. However, C-sections are more invasive and often entail a longer road to recovery. As they are becoming increasingly common we need to prepare women for what’s to come. And this all begs the question, why aren’t C-sections discussed more often.
We think the stigma that continues to shroud C-sections limits the conversation around the topic. At the end of the day, the best way to give birth is the way where both mom and baby are as healthy and happy as possible. Sometimes that is a vaginal, natural birth. Sometimes it involves an epidural. Sometimes it involves a C-section. Every pregnancy, every baby, and every female body is different, and that leads to so many different birth stories. At Baby2Body, we’re here to meet you exactly where you are, and if you’ve had a C-section or have one planned we want you to feel as prepared for what to expect when you go home.
From poling our audience, we’ve discovered that most of the key recovery aspects (such as not lifting and not driving) are known, but it’s the smaller anecdotal points from personal experience that are not publicly shared. For women having a first-time C-section, those anecdotes can go a long way in helping with preparedness and confidence in going home with baby.
So we’ve pulled together some facts and feedback from our audience on things you may not know about C-Section Recovery, but absolutely should.
1. There will be blood
Although you haven’t had a vaginal delivery you will still experience bleeding after birth. Many women are often surprised by this. It can be less bleeding with a planned C-Section but if you labored and then experienced an emergency Cesarean you can bleed just as much as with a vaginal delivery.
2. It’s going to feel frustrating at times
After a C-section, new mothers often struggle with stress, they must deal with caring for their newborn alongside caring for the painful incision scar and being far less mobile than if they’d had a vaginal delivery. It can make things as simple as getting out of bed very difficult and this frustration added to fluctuating postpartum hormones can be challenging to manage. Being aware of how limited your mobility will be in those first few weeks can help you prepare ahead of time, and get the support you need from your partner, family, or close friends.
3. You might need help feeding baby
Whether you are doing breast or bottle, feeding your baby is a whole lot harder after a C-Section. You will require much more support to lift your baby, and even getting up from a chair is surprisingly hard and a little painful. Remember, the muscles that support your abdomen were separated during your C-section, so you won’t have that abdominal strength to support you. Getting your partner or other family involved is going to be critical to your physical and emotional wellbeing.
4. Trapped gas is really common (and painful)
This is one side effect that isn’t talked about enough, but gas pains after a c section can be excruciating. They will pass within about a week but it can feel like you have a huge amount of air moving around your middle like a big balloon while everything settles back down after the interference of surgery.
5. You may experience numbness
Loss of feeling near the incision is a side effect that many women experience after a C-Section. It’s because small nerves are severed during surgery and it takes time for them to regrow, usually within several months but it can take longer. It’s a strange feeling but one that should pass. However, if you are still experiencing persistent numbness months after your operation then you should seek advice from your healthcare professional.
It’s because small nerves are severed during surgery and it takes time for them to regrow, usually within several months but it can take longer. It’s a strange feeling but one that should pass. However, if you are still experiencing persistent numbness months after your operation then you should seek advice from your healthcare professional.
6. You want to be careful when coughing, sneezing, or laughing
You will find any of the above difficult and painful in the first few days after your C-Section, as these daily actions use your abdominal muscles (that have been split open) and will make you feel like you are straining your incision wound. It’s not a pleasant sensation, but you can help by having a pillow or rolled-up towel nearby so if you feel like you might sneeze or cough then hold the pillow firmly on your scar area to support it as you do so.
7. You should know about “The Shelf”
Sometimes referred to as the pooch, this is where the skin above your C-Section scar hangs over creating a “shelf”. You will notice it while your tummy returns to normal after birth but some women continue to have it long after birth. The skin around the scar is often pulled much tighter than the looser skin above it which is why the shelf can occur.
You will notice it while your tummy returns to normal after birth but some women continue to have it long after birth. The skin around the scar is often pulled much tighter than the looser skin above it which is why the shelf can occur.
8. Your scar can look uneven
While you might imagine you’re going to have a central and symmetrical scar, this is not always the case. It can be cut higher on one side compared to the other and the scar tissue can be thicker in places. It depends on how your baby was lying and how the scar was closed at the time of surgery. In general, a C-section scar will fade and look much better within 2 weeks, but full healing can take up to 3 months. If you do have thicker areas of scar tissue that bother you then it could be worthwhile seeking help from a scar massage specialist.
9. There can be long-term side effects
Some women do experience symptoms related to their C-section scar long after the operation. Some women feel pain, restriction, or a pulling sensation on or around their scar months or even years after surgery. This is normally due to the build-up of scar tissue which can stick to muscles or even organs and cause pain. Sometimes that scar tissue pain can present as hip or lower back pain, shoulder pain or tension, headaches, or painful periods. If you are experiencing pain long after your C-Section we always advise you to seek advice; and similar to the suggestion above, you may want to seek a specialist in C-Section massage, which can help alleviate these problems.
Some women feel pain, restriction, or a pulling sensation on or around their scar months or even years after surgery. This is normally due to the build-up of scar tissue which can stick to muscles or even organs and cause pain. Sometimes that scar tissue pain can present as hip or lower back pain, shoulder pain or tension, headaches, or painful periods. If you are experiencing pain long after your C-Section we always advise you to seek advice; and similar to the suggestion above, you may want to seek a specialist in C-Section massage, which can help alleviate these problems.
Do you have more questions about C-section recovery? If you’ve had a C-section, what do you wish you were told beforehand to help you feel more prepared? Let us know in the comments below!
Is Your C-Section Scar Causing You Pain?
Your body goes through so many changes not only during pregnancy but after as well. If you’ve had to have a c-section, the recovery can take some time, but what about lingering side effects? That pain in your neck, lower back, or even cramping could be from scar tissue.
These types of reactions are due to the fascial restrictions that are caused when the scar heals. When you have major surgery, your fascia is cut. When your cut is healing, the fascia forms a layer of tissue even tighter than before so the body can protect itself.
Click the link here to read more about scar tissue and how we can help you get back to feeling better with myofascial release.
C-section Scar Tissue Release
“When you are cut for any reason, the physiological mechanism your body has to combat the trauma is to seal the wound quickly and efficiently, eventually producing a scar” (Conquering Mystery Pain, p. 65). Scarring from cuts can lead to adhesions, which are an internal complication directly connected with the scarring process. Adhesions can spread from the scar area throughout the body, and they can reach certain areas of the body that might seem completely unrelated to where the scarring actually took place. Most times, people are not even aware that pain in one area of the body directly correlates to scarring in a completely different area of the body.
Most times, people are not even aware that pain in one area of the body directly correlates to scarring in a completely different area of the body.
This can lead to more complications for women, especially those who have had cesarean sections and episiotomies. Both of these surgeries require tissue to be cut, forming a scar. A lot of women experience pain months after having a cesarean section, and they don’t realize that it is directly related to that surgery and that they need to seek treatment.
Dr. Jess shares more information on scar tissue release and how our team of therapists works to release this fascial restriction. You can check out her book on Amazon for more detailed info on scars!
Scar Tissue Release
Adhesions form scars end up creating soft tissue restrictions, which can lead to symptoms such as pain, sensitivity, numbness, tingling, and dense build-up of tissue. But, one positive thing about adhesions, as opposed to scars, is that they are susceptible to manual change. When adhesions are treated by therapists who specialize in myofascial release therapy, flexibility is returned in the tissue because the MFR therapists are able to help your body achieve healing within the fascia. So, it is very important to note that certain pain or inflammation that you are experiencing could be directly related to scarring, especially if you have had a c-section. It is important to seek treatment from a therapist who specializes in MFR (like Dr. Jess!), as this is where the bulk of your healing will take place.
When adhesions are treated by therapists who specialize in myofascial release therapy, flexibility is returned in the tissue because the MFR therapists are able to help your body achieve healing within the fascia. So, it is very important to note that certain pain or inflammation that you are experiencing could be directly related to scarring, especially if you have had a c-section. It is important to seek treatment from a therapist who specializes in MFR (like Dr. Jess!), as this is where the bulk of your healing will take place.
If you have questions you can give us a call at (401) 602-7006 or you can schedule a 20-minute phone consultation to get more information. You can also schedule an appointment by visiting our website.
Tags: womens health, health and wellness, healthy tips, c-section scar, physical therapy, health, wellness, pain relief, women’s health
90,000 Growing pains in children. Causes of occurrence
What it is?
Often, growth pains in the legs include manifestations of discomfort in the absence of organic pathology.
Other names: “recurrent nocturnal limb pain” and “benign limb pain in children” emphasize the features of the condition: nocturnal symptoms that recur and a favorable prognosis.
Meanwhile, the disease disrupts the full sleep of a small person and causes concern for moms and dads.
How often do they meet?
The disorder occurs in different countries: from 10 to 50% of boys and girls turn to a pediatrician, orthopedist, rheumatologist with characteristic complaints.
What are the causes of the condition?
Today there is no consensus why it appears. Meanwhile, it was established that “growth pains” actually have nothing to do with the process of growth.
Importance is given to a combination of factors:
- Excessive mobility and physical activity of children in this age period.
- Increased excitability of the nervous system and impressionability of babies.
 The immature nervous system does not have time to process and interpret the increased number of incoming impulses. At night, at rest, the brain perceives signals of irritation, stretching, pressure as pain.
The immature nervous system does not have time to process and interpret the increased number of incoming impulses. At night, at rest, the brain perceives signals of irritation, stretching, pressure as pain. - Scientists have found that babies who wake up at night crying and complaining of leg twisting have a lower pain threshold. Patients are also hypersensitive to other stimuli.
- A number of studies have found vitamin D deficiency in patients. The problem of this hypovitaminosis is relevant for boys and girls of any age.
 The immature nervous system does not have time to process and interpret the increased number of incoming impulses. At night, at rest, the brain perceives signals of irritation, stretching, pressure as pain.
The immature nervous system does not have time to process and interpret the increased number of incoming impulses. At night, at rest, the brain perceives signals of irritation, stretching, pressure as pain. In some patients, episodes of headaches and abdominal pain are recorded, the cause of which cannot be determined.
The theory that was popular in recent years about the occurrence of bone pain during growth has not been confirmed. Symptoms do not depend on changes in the musculoskeletal system, jumps and rates of increase in body length.
How does the disease manifest itself?
Symptoms of growing pains scare parents. A typical picture is as follows: the child suddenly wakes up a few hours after falling asleep, crying, with complaints of throbbing, pulling pain in the knees, shins, ankles, calf muscles on both sides.
A typical picture is as follows: the child suddenly wakes up a few hours after falling asleep, crying, with complaints of throbbing, pulling pain in the knees, shins, ankles, calf muscles on both sides.
Pain in the arms is less common, in addition to signs of abnormalities in the knees and lower legs.
For preschoolers, dull arching pain is characteristic, for schoolchildren – a feeling of crawling, a desire to move limbs.
Headache and abdominal discomfort are sometimes noted.
The episode lasts 10-20 minutes, intuitively parents try to improve their well-being by massaging, kneading and rubbing their legs until the child calms down and falls asleep. In the morning, the baby wakes up healthy and often does not remember what happened. During the day, the joints do not bother, and after a night or two, the situation is exactly the same.
The frequency of episodes varies from 3-4 times a year to daily, the intensity is from moderate to severe.
Parents note that awakenings are provoked by physical activity, emotional experiences and strong impressions during the day. The problem may disappear for weeks or months and then return.
In the family of patients, similar complaints are mentioned among other relatives.
What is important to know?
- There are no signs of illness during the daytime. No matter how hard the night passes, in the morning the child feels healthy. General well-being also does not suffer: normal temperature is maintained, there are no violations from organs and systems.
- Damage or inflammation of the joints and muscles is not determined by examination: there is no swelling, deformation or discoloration of the skin, the patient can perform all the normal range of motion of the arms and legs.
- Additional examination methods and laboratory tests show no pathology.
How to make a diagnosis?
Suspect the disease allows a colorful description of the attack and the presence of characteristic criteria:
- repeated nocturnal episodes: more than once a month for at least 3 months;
- bilateral character;
- high intensity: baby wakes up and cries
- after days of increased physical activity
- no visible changes on physical examination
- excellent health of the patient in the daytime.

The diagnosis is established on the basis of clinical signs after the exclusion of other pathology, primarily arthritis.
When carefully examining a small person, pay attention to:
- musculoskeletal disorders: change in movement, joint swelling or tenderness to pressure on bones;
- skin changes that occur in rheumatology: with juvenile dermatomyositis, systemic lupus erythematosus, psoriasis;
- gait, which demonstrates abnormalities in lesions of the nervous and musculoskeletal systems;
- an increase in the size of the lymph nodes, liver, spleen is alarming in terms of the tumor process.
The results of laboratory tests and instrumental methods of examination help to confirm the diagnosis.
What diagnostic methods are used?
Changes in tissues are not determined during this process, so instrumental diagnostics is necessary to exclude other, serious pathologies.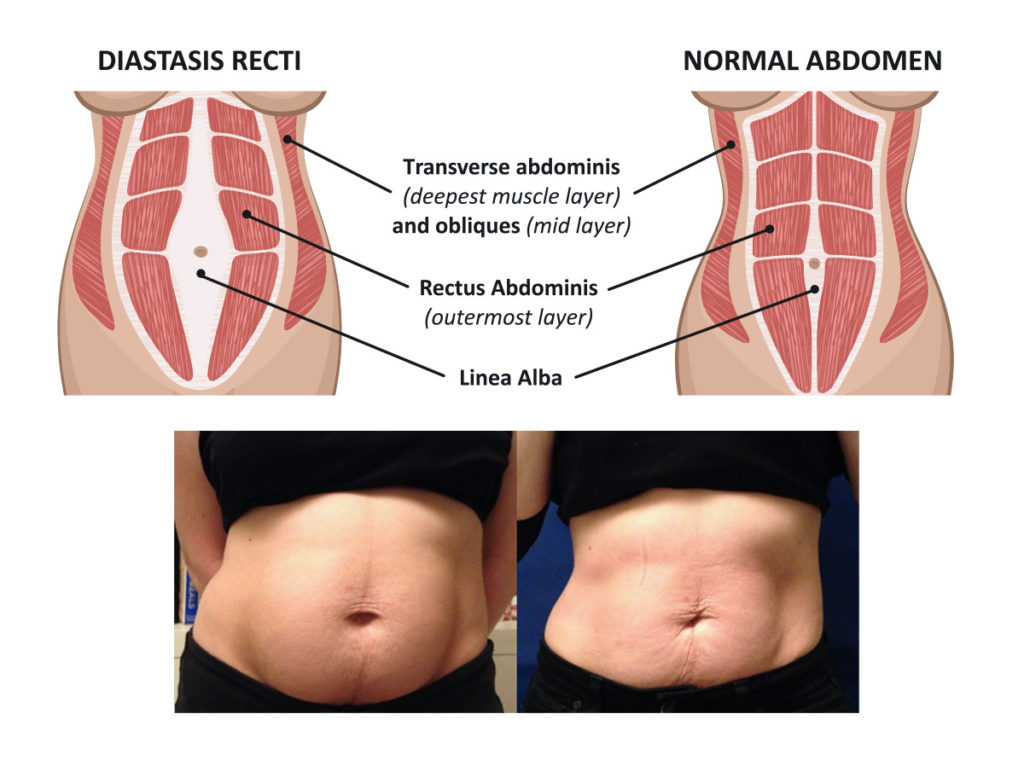
The standard examination plan for recurring nocturnal discomfort in the limbs includes clinical and biochemical blood tests with the determination of indicators of the function of internal organs, the level of C-reactive protein, the main marker of inflammation.
With the help of a general urine test, metabolic disorders are detected. If an infection is suspected, the serum is examined for antibodies to bacteria.
Radiography determines bone damage, ultrasound – pathology of soft tissues. Instrumental methods of examination are prescribed according to indications.
Which doctor should I contact?
A child who has pain in the legs or arms needs a face-to-face examination by a rheumatologist to rule out arthritis.
Situations that require immediate medical attention:
- pain on one side;
- symptoms are present in the morning, afternoon or evening;
- external manifestations of ill health: swelling of soft tissues, fever or discoloration of the skin, impossibility of movement;
- first-time manifestations younger than three and older than 12 years.

How is the disease treated?
Your son or daughter has been diagnosed with growing pains, what should I do?
Firstly, the parent needs to understand and explain to the child the nature of what is happening in an accessible language. This will reduce anxiety and relieve the baby of fear.
Changing the mode will help: reduce physical activity and transfer the time of sports to the first half of the day.
After lunch and in the evening, give preference to calm games. Extend your bedtime rituals and add relaxing treatments: A warm bath, soothing soft music, dimmed lights, or warm milk can help your baby.
During attacks, with light massaging movements, stroke, rub and knead the areas where there are unpleasant sensations. To alleviate the condition, dry heat helps: apply a towel or heating pad heated on the radiator to your feet. If necessary, have your son or daughter sit on your lap or lie down next to you until the child calms down.
In most cases, the measures taken are sufficient.
If the episodes are daily or intense, the doctor prescribes age-appropriate ibuprofen at the time of the attack or before going to bed.
When vitamin D deficiency is detected, it is necessary to take a therapeutic dose of the drug under the supervision of a doctor.
Is the disease dangerous?
The process does not change the growth and development of a small person, does not destroy bones and joints, and does not lead to other chronic diseases.
Anxiety causes the sensations themselves and nocturnal awakenings, however, they also disturb the parent to a greater extent.
Growing pains in teens disappear at 90% of cases. One in 20 patients persists into adulthood.
The danger is represented by serious violations with similar manifestations, which are disguised as a benign process.
You should be alerted if
- a pathological process prevents the baby from getting enough sleep and functioning normally: to study, play, explore the world around;
- symptoms are noted in the morning or in the afternoon, their intensity increases;
- discomfort associated with a traumatic event;
- there is swelling, redness, rash or skin changes in the painful area;
- developed fever, change in appetite, weakness and fatigue.

Conclusion
Growth pains are a benign condition that does not affect growth and development, which develops in 1-5 out of 10 children – preschoolers and younger schoolchildren. The main manifestation is a recurring nocturnal pain in both legs, from which the child wakes up. The phenomenon is temporary and does not harm the general health of a small person.
If you suspect a pathological process, contact your pediatrician and visit a rheumatologist to rule out inflammation in the joints.
Sources:
- Cassidy JT. Progress in diagnosis and understanding chronic pain syndromes in children and adolescents // Adolesc Med, 1998
- Pavone V, Lionetti E, Gargano V, et al. Growing pains: a study of 30 cases and a review of the literature // J Pediatr Orthop, 2011
- Sarycheva L.V., Growing pains in children. Are we sick or growing? // GKUZ NSO RCMP, 2009
- Korovina N.A., Tvorogova T. M., Gavryushova L.P., Vorobieva A.S. Safety criteria for the use of calcium preparations for the prevention of osteopenia in adolescents // Russian Medical Academy of Postgraduate Education, 2006
- Saggese G., Baroncelli G.I., Btrtelloni S. // J. Pediatr. Endocrinol. Metab, 2001
 M., Gavryushova L.P., Vorobieva A.S. Safety criteria for the use of calcium preparations for the prevention of osteopenia in adolescents // Russian Medical Academy of Postgraduate Education, 2006
M., Gavryushova L.P., Vorobieva A.S. Safety criteria for the use of calcium preparations for the prevention of osteopenia in adolescents // Russian Medical Academy of Postgraduate Education, 2006 Diastasis of the rectus abdominis muscles and diastasis of the womb. Solvable problems of pregnancy. Interview with Doctor of Medical Sciences, Professor M.A. Chechnyova
— What is muscle diastasis and what is pubic diastasis?
— Pregnancy is an amazing and wonderful time, but it is also a period of additional loads, which undoubtedly becomes a test of strength for the female body.
The previously existing everyday point of view that pregnancy rejuvenates and gives strength is not confirmed by anything. During the bearing of a child, significant additional loads are placed on the mother’s body, which often lead to the manifestation of problems that were invisible before pregnancy.
Diastasis of the rectus abdominis muscles is a divergence of the inner edges of the muscles along the white line of the abdomen (connective tissue structure) at a distance of more than 27 mm. Pubic diastasis is one of the manifestations of pregnancy-associated pelvic girdle pain. This pathology affects the entire pelvic ring, sacroiliac joints and symphysis. And they certainly have common causes for the appearance.
The formation of such problems is facilitated by a decrease in the strength of connective tissue collagen. One of the reasons is an innate predisposition, the so-called connective tissue dysplasia, when the tissues are very elastic, extensible. During pregnancy, the body of a woman increases the production of the hormone relaxin, which reduces the synthesis of collagen and enhances its breakdown. This is provided by nature to create maximum elasticity of the birth canal. However, other structures, such as the anterior abdominal wall and the pubic symphysis, also fall under the action of relaxin.
— How does diastasis of the muscles and diastasis of the pubis affect pregnancy and childbirth?
– Divergence of the rectus abdominis muscles is observed in approximately 40% of pregnant women. During pregnancy, it does not give serious complications that threaten the life of the mother or the condition of the fetus. However, the inferiority of the work of the rectus abdominis muscles forces the redistribution of the load on the back muscles, which can lead to lumbar-pelvic pain and, accordingly, discomfort in the back. During childbirth, the abdominal muscles are involved in attempts, and the violation of their anatomy and function can affect the birth act.
With diastasis of the pubis, things are more complicated. As already mentioned, this is only one of the manifestations of a violation of the structure and function of the pubic joint (symphysiopathy) during pregnancy. It occurs in about 50% of pregnant women in varying degrees of severity: in 25% of cases it leads to restriction of the mobility of the pregnant woman, in 8% – to severe disorders up to disability.
With symphysiopathy, the ligaments of the pubic articulation and cartilage that connect the pubic bones suffer. All this leads to severe pain in the pubic joint, pelvic bones, lower back, as well as to a violation of gait and the inability to stand up or lie down without outside help. Women with pelvic girdle pain syndrome experience significant levels of discomfort, disability, and depression, with associated social and economic problems. These include impaired sexual activity during pregnancy, chronic pain syndrome, risk of venous thromboembolism due to prolonged immobility, and even seeking early induction of labor or caesarean section to stop pain.
During childbirth, this patient may experience a rupture of the pubic symphysis and may require surgery to repair it.
— How to prevent the development of muscle and pelvic diastasis during pregnancy and childbirth? What factors increase the likelihood of its development?
– There is no recipe that will be one hundred percent. There is a wonderful term in the medical literature called “lifestyle modification”. Whatever diseases we study, be it symphysiopathy, diabetes mellitus or preeclampsia, the risk group for pathology is always overweight women. You need to prepare for pregnancy, you need to be in good physical shape. During pregnancy, weight gain should be monitored. The recommendation to “eat for two” is not just wrong, but extremely harmful. Pregnant women should maintain reasonable physical activity. Weak and flabby abdominal muscles, combined with the large size of the fetus, undoubtedly increase the risk of diastasis.
There is a wonderful term in the medical literature called “lifestyle modification”. Whatever diseases we study, be it symphysiopathy, diabetes mellitus or preeclampsia, the risk group for pathology is always overweight women. You need to prepare for pregnancy, you need to be in good physical shape. During pregnancy, weight gain should be monitored. The recommendation to “eat for two” is not just wrong, but extremely harmful. Pregnant women should maintain reasonable physical activity. Weak and flabby abdominal muscles, combined with the large size of the fetus, undoubtedly increase the risk of diastasis.
The risk factors for symphysiopathy in numerous studies are heavy physical labor and previous injuries of the pelvic bones. Factors such as time elapsed from previous pregnancies, smoking, use of hormonal contraception, epidural anesthesia, mother’s ethnicity, number of previous pregnancies, bone density, weight and gestational age of the fetus (post-term fetus) are not associated with an increased risk of symphysiopathy.
– How to diagnose diastasis recti and diastasis pubis?
— In most cases, diastasis rectus abdominis can be diagnosed clinically. It happens that inspection, palpation and simple measurements are enough.
In the standing position, you can see the divergence of the muscles when the woman does not have subcutaneous fat. In this case, diastasis is defined as a vertical defect between the rectus muscles.
With tension of the abdominal press, a longitudinal protrusion is observed in the diastasis zone. Such a protrusion is especially noticeable if the patient in the supine position is asked to raise her head and legs. If necessary, you can measure the width of the defect simply with a ruler.
Ultrasound may be the most accurate diagnostic method. With ultrasound, the inner edges of the rectus muscles are clearly visible and the distance between them at different levels can be measured.
Computed tomography is used in the diagnosis of diastasis extremely rarely, mainly in scientific research.
For the diagnosis of symphysiopathy and diastasis pubis there is no one test as a “gold standard”.
The first place, of course, is the questioning and examination of the patient. We pay attention to the gait of the pregnant woman, to how she sits down, lies down and how she gets up. Symphysiopathy is characterized by a “duck gait”, when a pregnant woman rolls from foot to foot. On palpation in the area of the womb, pain and swelling are noted. The so-called pain provocative tests are used, for example, a mat-test (pulling up an imaginary rug, mat with your foot towards you).
The following questionnaires are used to assess the quality of life, the level of pain and disability: Health-Related Quality of Life (HRQL), Oswestry Disability Index (ODI), Disability Rating Index (DRI), Edinburgh Postpartum Depression Scale (EPDS), Pregnancy Mobility Index (PMI), and Pelvic Ring Score (PGQ).
Of the instrumental methods, ultrasound is the most widely used, less often computed or magnetic resonance imaging. Ultrasound allows you to assess the condition of the ligaments of the pubic joint and the interpubic disc, the severity of the changes and the risk of natural childbirth.
Ultrasound allows you to assess the condition of the ligaments of the pubic joint and the interpubic disc, the severity of the changes and the risk of natural childbirth.
— What is the treatment for diastasis recti or pubis?
— Primary prevention: when planning and during pregnancy, it is necessary to strengthen all muscle groups of the pelvic girdle, as well as the pelvic diaphragm.
More often, diastasis of the rectus muscles disappears on its own during the first months after childbirth. Special physical exercises to correct the work of muscles, to tone them and restore their basic functions should be performed under the guidance of a competent instructor. There are types of physical exercises that can, on the contrary, worsen the situation with diastasis of the rectus abdominis muscles. In some cases, when there is no effect from physiotherapy exercises, it is necessary to resort to surgical correction of the defect. Currently, both endoscopic and open surgery are practiced. The choice of method depends on the size and localization of the defect.
The choice of method depends on the size and localization of the defect.
With symphysiopathy, therapeutic exercises reduce lumbar and pelvic pain. Acupuncture and wearing a pelvic bandage have a positive effect on symphysiopathy.
Initial treatment for pubic symphysis should be conservative even if symptoms are severe. Treatment includes bed rest and the use of a pelvic brace or corset that tightens the pelvis. Early appointment of physiotherapy with dosed therapeutic exercises will help to avoid complications associated with prolonged immobilization. Walking should be done with assistive devices such as walkers.
In most cases (up to 93%), the symptoms of dysfunction of the pelvic ring, including the pubic joint, progressively subside and completely disappear six months after birth. In other cases, it persists, becoming chronic. However, if the diastasis exceeds 40 mm, then surgical treatment may be required. Most studies recommend surgery only after failure of conservative treatment, inadequate enlargement of diastasis, or its recurrence.