






What is physical growth and development: Your Child’s Growth (for Parents)
Your Child’s Growth (for Parents)
What Is Growth?
Physical growth refers to the increases in height and weight and other body changes that happen as kids mature. Hair grows; teeth come in, come out, and come in again; and eventually puberty hits. It’s all part of the growth process.
What’s Normal?
The first year of life is a time of amazing change during which babies, on average, grow 10 inches (25 centimeters) in length and triple their birth weights.
Given all the growth that happens then, new parents might be surprised when their child doesn’t continue to grow so fast after the first year. But no child continues the rate of growth of infancy. After age 1, a baby’s growth in length slows quite a bit. By age 2, growth in height usually continues at a fairly steady rate of about 2½ inches (6 centimeters) per year until adolescence.
No child grows at a perfectly steady rate throughout this period of childhood, though. Weeks or months of slightly slower growth alternate with mini “growth spurts” in most children. Kids actually tend to grow a bit faster in the spring than during other times of the year!
A major growth spurt happens at the time of puberty, usually between 8 to 13 years of age in girls and 10 to 15 years in boys. Puberty lasts about 2 to 5 years. This growth spurt is associated with sexual development, which includes the appearance of pubic and underarm hair, the growth and development of sex organs, and in girls, the start of menstruation.
By the time girls reach age 15 and boys reach age 16 or 17, the growth of puberty has ended for most and they will have reached physical maturity.
At the Doctor’s Office
Beginning in infancy, kids will visit a doctor for regular checkups. During these, the doctor will record height and weight as they compare with that of other kids the same age on a growth chart. This valuable tool can help the doctor determine whether a child is growing at an appropriate rate or whether there might be problems.
How Can Parents Help?
You can do a few things to help your child grow and develop normally. For their overall health and wellness, kids need:
For their overall health and wellness, kids need:
- Enough rest: Sleep patterns vary by age and individual child. But most kids need an average of 10 to 12 hours of sleep per night. Sleep gives growing bodies the rest they need to grow well.
- Good nutrition: A balanced diet full of essential vitamins and minerals will help kids reach their full growth potential.
- Regular exercise: Because obesity is a problem for many kids, parents should make sure that their kids exercise regularly. Bicycling, hiking, in-line skating, sports, or any enjoyable activity that will motivate kids to get moving will promote good health and fitness and help them maintain a healthy weight.
Talking to Kids About Growth
Kids differ in growth and development during childhood. And as with adults, some kids are taller or shorter. Generally, girls hit puberty earlier than boys, though some girls might lag behind their peers in breast development or getting their first period. All of this is usually normal.
All of this is usually normal.
Try not to compare growth among siblings or other children. Drawing attention to height, for example, will only make kids feel self-conscious about their size. Encourage your kids to accept their own growth and development. Explain that some kids grow and develop at different rates — and late bloomers usually catch up eventually.
Kids have many questions about growth, from why their teeth fall out to tough or embarrassing topics like breast development or sweating. Answer questions honestly and even start talks about growth to help kids understand the many changes they’re facing. This will help them accept the changes positively.
If you’re uncomfortable discussing these topics, your kids may think there’s something shameful about the changes they go through and might be less likely to bring their concerns to you.
Kids who are short often face teasing by peers and may need help coping. You can help by supporting your child’s self-esteem. For example, it might be hard for a small boy to make the football team. But focusing on alternatives, such as soccer or tennis, may make him feel better about himself and what he can do. Try to understand your child’s feelings and keep the lines of communication open.
For example, it might be hard for a small boy to make the football team. But focusing on alternatives, such as soccer or tennis, may make him feel better about himself and what he can do. Try to understand your child’s feelings and keep the lines of communication open.
Another way to boost your child’s mood is to encourage activities that don’t focus on height or weight. Special skills and individual qualities, such as musical talent or a love of literature, are things to be proud of too.
What Should I Do if I Think There’s a Problem?
Some parents worry about their child’s growth and development. So it can be reassuring to know that most kids who are short or delayed in development are healthy and normal. Shorter parents tend to have shorter children, for example, and not all kids develop at the same rate.
If you have concerns, talk with your doctor. The doctor can examine your child, ask questions about your family history and, if needed, order tests to see if there’s a medical condition affecting growth. The doctor may check your child’s growth more often or refer your child to a pediatric endocrinologist (a doctor who treats growth disorders).
The doctor may check your child’s growth more often or refer your child to a pediatric endocrinologist (a doctor who treats growth disorders).
Medically reviewed by: Madhu Desiraju, MD
Date reviewed: June 2022
Physical Growth | Encyclopedia.com
Physical growth usually refers to changes in size or mass; so it is correct to say that a child grows in stature (height) or body weight. Even though most people usually think of growth at the level of the whole child, the cells and internal structures that make up the child also grow, primarily by increasing in number or size. Consequently, auxologists (those who study child growth) may be interested in the growth of bones to help understand fractures and osteoporosis; the growth of the heart walls to help understand hypertension (high blood pressure) and heart disease; or the growth of adipose tissue (body fat) to help understand obesity.
The measurement of body dimensions such as those used in growth studies is called anthropometry. Past growth is usually measured as the size attained at a chronological age, for example the weight of a child at eight years old. Assessment of the rate of growth requires that a body dimension, such as weight, be measured twice over a period, and then the change is expressed in terms of the increment or velocity of growth, for example in pounds or kilograms per year.
Past growth is usually measured as the size attained at a chronological age, for example the weight of a child at eight years old. Assessment of the rate of growth requires that a body dimension, such as weight, be measured twice over a period, and then the change is expressed in terms of the increment or velocity of growth, for example in pounds or kilograms per year.
Some physical changes in childhood are more complicated than just size or mass. These changes include alterations in body structures and functions and can be termed development. Physical developmental changes are as diverse as the closing of the fontanels (soft spots) in a baby’s skull, the erupting of teeth, learning to walk, or the deepening of the voice of boys during adolescence.
Some developmental changes are considered maturational, or indicators of physical maturity. Maturation is the progression of developmental changes toward the characteristics of adults. Physical maturation occurs from the time of conception, but some of the most commonly recognized indicators of maturation become apparent during adolescence. Changes in body shape, breast development in girls, pubic hair development in both genders, and development of facial hair in boys are visible indicators of maturation toward adult appearance of the body, and they signal adult reproductive functioning. The cessation of the growth of long bones, associated with the final attainment of adult stature is also a maturational event.
Changes in body shape, breast development in girls, pubic hair development in both genders, and development of facial hair in boys are visible indicators of maturation toward adult appearance of the body, and they signal adult reproductive functioning. The cessation of the growth of long bones, associated with the final attainment of adult stature is also a maturational event.
Although growth and maturation are certainly related, distinguishing between them is important because some physiological and hormonal processes affect growth and maturation differentially, as do some diseases. It is easy to observe that children of the same size can differ in maturational status and that fully mature individuals (adults) can be of different sizes.
General Patterns
Growth differences between males and females begin before birth and continue until adulthood. Generally, boys are larger than girls throughout gestation, so that when they are born at full term (forty weeks), male newborns usually weigh about 150 grams (5. 3 ounces) more than females, and are about one centimeter (0.4 inches) longer. Even though they are smaller than their male counterparts, female babies are usually more mature skeletally and neurologically at birth.
3 ounces) more than females, and are about one centimeter (0.4 inches) longer. Even though they are smaller than their male counterparts, female babies are usually more mature skeletally and neurologically at birth.
After birth, most body dimensions, such as stature, body circumferences, and weight, follow a similar pattern of growth: a period of very rapid growth in infancy, slower growth during middle childhood, a very rapid growth phase or spurt in adolescence, and a period of rapidly decelerating growth, ending with adult size. Obviously, some body dimensions, such as weight or fatness, can continue to change throughout adulthood. The different phases of postnatal growth can be appreciated more easily by looking at the rates of growth, or velocity, in addition to attained size.
On average, boys are taller and heavier than girls at every postnatal age, except from about nine to thirteen years. The reversal of size differences at these ages results from girls entering their adolescent growth spurt about two years earlier than boys. Boys usually end up about nine to thirteen centimeters (three to five inches) taller and seven to nine kilograms (fifteen to twenty pounds) heavier than girls at eighteen years of age. This is primarily because boys grow approximately two years longer than girls do before their spurt, and because the spurt of boys usually is more intense and lasts a little longer than that of girls.
Boys usually end up about nine to thirteen centimeters (three to five inches) taller and seven to nine kilograms (fifteen to twenty pounds) heavier than girls at eighteen years of age. This is primarily because boys grow approximately two years longer than girls do before their spurt, and because the spurt of boys usually is more intense and lasts a little longer than that of girls.
Timing of Maturation
Different body structures and functions often mature at differing rates, and they achieve adult status at different average chronological ages. For example, the three tiny bones of the inner ear (the incus, malleus, and stapes) are mature before birth, while the last bone to achieve adult status (the clavicle or collarbone) does not do so until approximately twenty-five years of age.
Even within groups of healthy children, there is considerable variation in the timing of the same maturational processes and events. For example, the first menstrual period of girls, or menarche, signals achievement of one aspect of adult reproductive functioning and is a widely used maturational indicator. (The corresponding but less noticeable event in boys is the first production of sperm cells, or spermarche.) The average age at menarche for girls in the United States is approximately 12.8 years of age. About two-thirds of U.S. girls will attain menarche within one year of the average timing, and about 98 percent of all girls within two years. For healthy girls, this variation in the timing of menarche is due to inherited patterns from their parents. Age at menarche (and most other maturational timing) can be delayed by malnutrition and infectious disease, and less commonly by hormonal dysfunction.
(The corresponding but less noticeable event in boys is the first production of sperm cells, or spermarche.) The average age at menarche for girls in the United States is approximately 12.8 years of age. About two-thirds of U.S. girls will attain menarche within one year of the average timing, and about 98 percent of all girls within two years. For healthy girls, this variation in the timing of menarche is due to inherited patterns from their parents. Age at menarche (and most other maturational timing) can be delayed by malnutrition and infectious disease, and less commonly by hormonal dysfunction.
The chronological age at which maturational events occur provides a measure of the relative timing of that event in the child’s growth and development. In addition to menarche, other examples of maturational events whose timing may be of interest include onset of ossification of bony centers (visible in X rays), eruption of teeth, first walking, first appearance of pubic hair, the age when the adolescent spurt is at its peak velocity, and the final fusion of the growing centers of long bones.
Of course, these maturational events are really biological processes that occur progressively in the developing child and the “event” is really just an arbitrary point in the developmental process that has been defined by auxologists so that it can be measured more easily. Some maturational processes have been more or less arbitrarily defined in stages or grades so that the progress through the stages can be measured. The progressive development of the secondary sexual characteristics associated with sexual maturation is a common example where such stages have been applied. The development of breasts in girls, penis and scrotum in boys, and pubic hair in both genders have carefully described stages of development that pediatricians and endocrinologists use clinically and that are also used by researchers who are interested in normal and abnormal adolescent growth and maturation.
Nutrition, Health, and the Environment
Physical growth and maturation are often used as indicators of child health because they are sensitive to nutritional deficiencies, infection, and poverty. Growth is a very adaptable process that will slow in the face of extreme nutritional deficiency, for example, as a mechanism to conserve nutrients for body functions essential to the child’s survival. Growth will resume or even catch up at faster rates than normal when the nutritional deficits are remedied. This sensitivity to health and environmental constraints makes growth an excellent indicator of the adequacy of nutrition and the health of individuals and of populations. As basic indicators of health, pediatricians compare the attained stature and weight of children and their rates of growth with the expected values for healthy children or with growth standards.
Growth is a very adaptable process that will slow in the face of extreme nutritional deficiency, for example, as a mechanism to conserve nutrients for body functions essential to the child’s survival. Growth will resume or even catch up at faster rates than normal when the nutritional deficits are remedied. This sensitivity to health and environmental constraints makes growth an excellent indicator of the adequacy of nutrition and the health of individuals and of populations. As basic indicators of health, pediatricians compare the attained stature and weight of children and their rates of growth with the expected values for healthy children or with growth standards.
In public-health studies comparing different populations or countries, the percentage of young children with very short stature (stunting) and the percentage of those whose weight is very low for how tall they are (wasting) are important indicators of nutritional and health conditions affecting children. In such studies, the average age at menarche, or of other maturational events, may be used to indicate the adequacy of general health and nutritional conditions.
Some examples of the average age at menarche from different countries are given in Table 1. Average ages of menarche greater than 13.5 years are usually considered to be associated with some general nutritional or health constraints in the country. In the case of Nepal, these issues are probably complicated by the people living at very high altitude, which may affect growth and maturation because of the reduced availability of oxygen to the body.
When nutritional energy (calories from food) is in excess of what the body uses and what is expended in physical activity, it is stored in adipose tissue. This fat tissue is accumulated within the body and subcutaneously (under the skin). The growth in weight of children and measurements of the thickness of the subcutaneous fat by calipers are used as indicators of overweight and obesity. Sometimes the weight of children is expressed as an index relative to stature (calculated by dividing the weight, in kilograms, by the square of stature, in meters) to yield the body mass index (BMI). BMI standards are also commonly used to define overweight and obesity and to relate these conditions to various health outcomes.
BMI standards are also commonly used to define overweight and obesity and to relate these conditions to various health outcomes.
Physical growth includes many aspects of the biological development of children that can reflect genetics, nutrition, health, and the environment. The aspects of physical growth are central to the child’s progress toward adulthood, and they inevitably interact with psychological, behavioral, and social aspects of the developing child.
See also:MENARCHE; MILESTONES OF DEVELOPMENT; MOTOR DEVELOPMENT; NUTRITION; OBESITY
Bibliography
Buckler, J. M. H. A Reference Manual of Growth and Development, 2nd edition. Oxford: Blackwell Science, 1997.
Eveleth, Phyllis B., and James M. Tanner. Worldwide Variation inHuman Growth, 2nd edition. Cambridge, Eng.: Cambridge University Press, 1990.
Himes, John H., ed. Anthropometric Assessment of Nutritional Status. New York: Wiley, 1991.
Malina, Robert M., and Claude Bouchard. Growth, Maturation, and Physical Activity. Champaign, IL: Human Kinetics, 1991.
Champaign, IL: Human Kinetics, 1991.
Tanner, James M. Foetus into Man: Physical Growth from Conception to Maturity. Cambridge, MA: Harvard University Press, 1990.
Tanner, James M., R. H. Whitehouse, and M. Takaishi. “Standards from Birth to Maturity for Height, Weight, Height Velocity, and Weight Velocity: British Children, 1965.” Archives of Disease in Childhood 41 (1966):613-635.
John H.Himes
LaVellGold
Norms of height and weight of children and adolescents
The physical development of a child as a combination of various indicators (length, weight, shape, strength, etc.) characterizing his growth and development is due to a complex of hereditary and social factors. To study the physical development of children and adolescents, a unified method for measuring the human body and its parts has been developed. All anthropometric indicators can be divided into two groups: basic (body length, body weight, chest and head circumference) and additional (other anthropometric indicators, for example, leg length, head height, etc. ). Analysis of the main anthropometric indicators at the time of the examination makes it possible to assess the physical condition of the child, in dynamics – the pace of physical development. At the same time, the features of the physique, the state of the musculoskeletal system, the degree of puberty, etc. are taken into account. Physical development is analyzed by comparing individual or group indicators with average data (standards) characteristic of the corresponding age and gender of the child.
). Analysis of the main anthropometric indicators at the time of the examination makes it possible to assess the physical condition of the child, in dynamics – the pace of physical development. At the same time, the features of the physique, the state of the musculoskeletal system, the degree of puberty, etc. are taken into account. Physical development is analyzed by comparing individual or group indicators with average data (standards) characteristic of the corresponding age and gender of the child.
The value of indicators of a child’s physical development can be explained by a number of arguments. For many chronic diseases of childhood, there are no specific symptoms related to the early stage of the development of the disease, therefore, a violation of physical development is one of the first signs of trouble and serves as an indication for an in-depth examination of the child. Violations of the physical development of children and adolescents may be the result of malnutrition, lack of necessary care, improper or harsh treatment of the child, etc.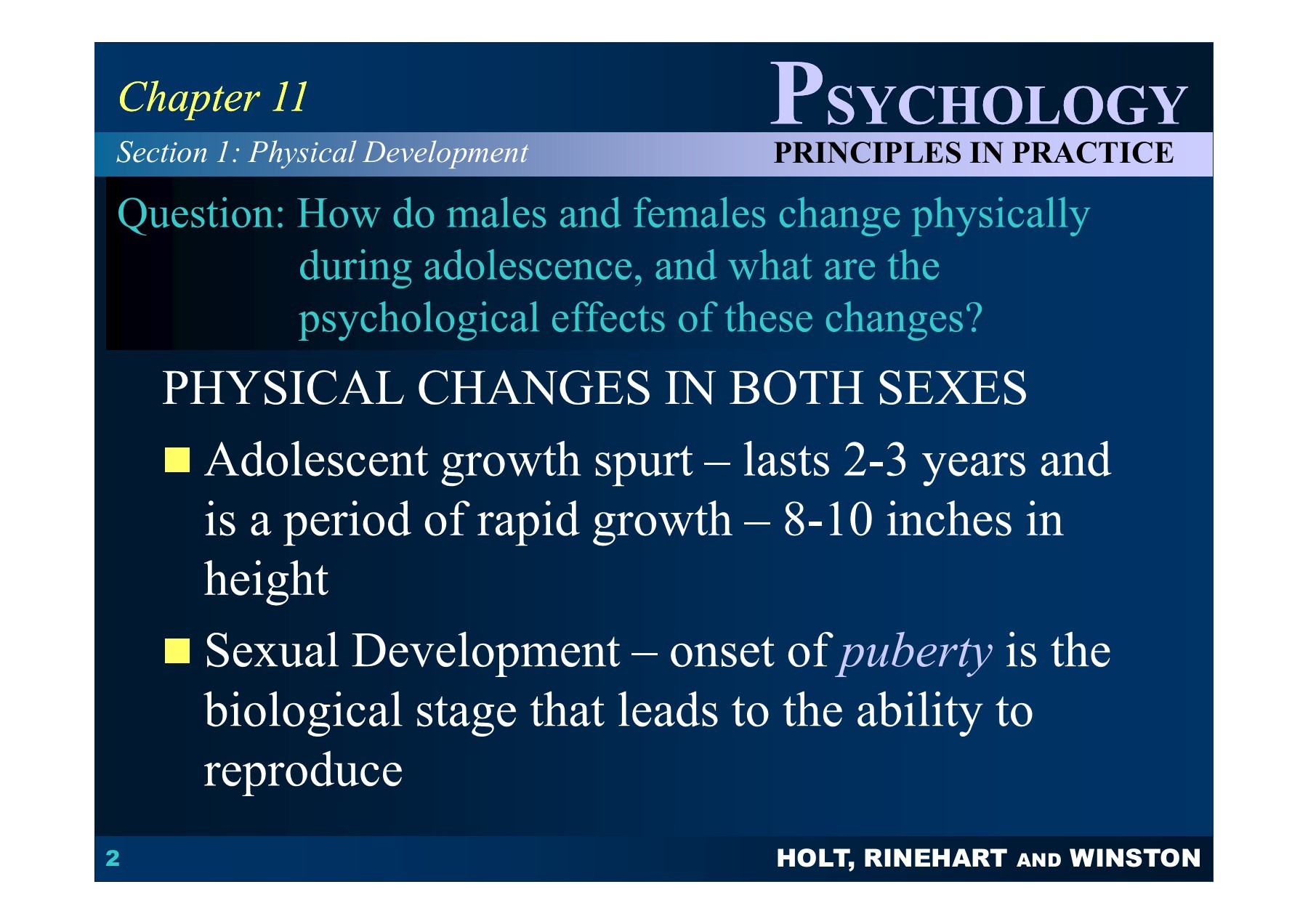 Violations of physical development can cause constitutional features, congenital or hereditary pathology of the developmental apparatus. Such children have imperfect mechanisms of adaptation and anti-infective protection, for example, a lack of body weight in a child may be accompanied by a higher frequency of minor developmental anomalies. Any deviations of anthropometric parameters from the norm at the birth of a child can become one of the reasons for the decrease in immunological resistance, increasing the likelihood of a disease in the first year of life by half, and the probability of death by 4 times. All factors characterizing the growth and development of the child’s body can be divided into genetic and environmental factors. The influence of heredity affects the growth of the child after 2 years of life.
Violations of physical development can cause constitutional features, congenital or hereditary pathology of the developmental apparatus. Such children have imperfect mechanisms of adaptation and anti-infective protection, for example, a lack of body weight in a child may be accompanied by a higher frequency of minor developmental anomalies. Any deviations of anthropometric parameters from the norm at the birth of a child can become one of the reasons for the decrease in immunological resistance, increasing the likelihood of a disease in the first year of life by half, and the probability of death by 4 times. All factors characterizing the growth and development of the child’s body can be divided into genetic and environmental factors. The influence of heredity affects the growth of the child after 2 years of life.
Hereditary factors mainly determine the rate and possible limit of a child’s growth under optimal environmental conditions.
The influence of environmental factors on the growth rate of the child’s body can be traced very clearly. Among these factors, nutrition and vitamin sufficiency, motor mode and emotional stress, acute and chronic diseases, the influence of climatic and geographical conditions, etc. are distinguished. At the same time, environmental factors can slow down or accelerate growth processes, but in general the growth trend is quite stable, it obeys the conservation law growth. A variety of adverse influences that disrupt the individual growth rate of a child can subsequently be neutralized by the phenomenon of “catch-up or compensatory growth.” What happens to the physical development of your baby from the moment of birth to its full maturity? We observe the growth and development of a child in the first year of life: How can we understand if he is healthy, is everything okay with him? Remember: the health of a child is judged primarily by its weight, height and head circumference. On average, a newborn’s body weight is 3.0-3.5 kg, body length 50 cm, head circumference 35 cm. But do not expect your baby to necessarily meet this standard.
Among these factors, nutrition and vitamin sufficiency, motor mode and emotional stress, acute and chronic diseases, the influence of climatic and geographical conditions, etc. are distinguished. At the same time, environmental factors can slow down or accelerate growth processes, but in general the growth trend is quite stable, it obeys the conservation law growth. A variety of adverse influences that disrupt the individual growth rate of a child can subsequently be neutralized by the phenomenon of “catch-up or compensatory growth.” What happens to the physical development of your baby from the moment of birth to its full maturity? We observe the growth and development of a child in the first year of life: How can we understand if he is healthy, is everything okay with him? Remember: the health of a child is judged primarily by its weight, height and head circumference. On average, a newborn’s body weight is 3.0-3.5 kg, body length 50 cm, head circumference 35 cm. But do not expect your baby to necessarily meet this standard. Children are considered normal if their indicators are within the following limits: body weight 2.5-4.5 kg, length 45-55 cm, head circumference 33-37 cm. Immediately after birth, babies lose some weight, and then regain it and start adding. Further weight gain as well as height and head circumference are important indicators of your child’s condition. By the end of the 1st year of life, body length increases by 47% in relation to body length at birth.
Children are considered normal if their indicators are within the following limits: body weight 2.5-4.5 kg, length 45-55 cm, head circumference 33-37 cm. Immediately after birth, babies lose some weight, and then regain it and start adding. Further weight gain as well as height and head circumference are important indicators of your child’s condition. By the end of the 1st year of life, body length increases by 47% in relation to body length at birth.
Weight gain of a child in the first year of life: by 4-5 months, body weight doubles, by the 1st year it increases 3 times. The head circumference of a child in the first 6 months of life increases by approximately 1 cm per month, but if the father of the child is large and the mother is small, the growth rate of the head circumference may be above the norm, and in the opposite ratio – below the norm. The circumference of the chest of newborns is less than the circumference of the head, these dimensions are equalized only by the age of one. In the first month of life, the child must be weighed daily. Thus, you monitor the development of lactation and fix the daily weight gain. Body weight is the most sensitive indicator of a child’s health: whether he fell ill, whether his appetite worsened, whether his sleep was disturbed, whether you made any errors in care – all this will immediately be reflected in grams. A sign of nutritional adequacy is normotrophy – the correspondence of body weight due to a given body length of a child. If the weight of the baby has decreased by more than 10%, this is already a sign of malnutrition (malnutrition). Equally alarming is excess weight – parotrophy (excessive nutrition). But the increase in the growth of the child is a more stable indicator, and its violations often indicate the presence of the disease.
In the first month of life, the child must be weighed daily. Thus, you monitor the development of lactation and fix the daily weight gain. Body weight is the most sensitive indicator of a child’s health: whether he fell ill, whether his appetite worsened, whether his sleep was disturbed, whether you made any errors in care – all this will immediately be reflected in grams. A sign of nutritional adequacy is normotrophy – the correspondence of body weight due to a given body length of a child. If the weight of the baby has decreased by more than 10%, this is already a sign of malnutrition (malnutrition). Equally alarming is excess weight – parotrophy (excessive nutrition). But the increase in the growth of the child is a more stable indicator, and its violations often indicate the presence of the disease.
Assess the rate of development of your child in the first year of life, prescribe additional examinations in case of violations of the rate of weight gain, body length, head and chest circumference, correct nutrition, if necessary, a pediatrician will be able to, therefore the cooperation of parents is so important with a doctor from the very first year of a baby’s life.
It must be remembered that during the first month the pediatrician examines the child weekly, then, if the development of the baby corresponds to normal indicators, monthly. Assessment of the physical development of a child from one to 10 years. After your baby is one year old, he begins to grow by leaps and bounds. In the second year of life, he adds about 2.5-4.0 kg, and growth increases by 10-15 cm. At the age of 3 to 5 years, the baby adds 2 kg and 3 kg per year.
The head circumference of a child from 51 cm at the age of 5 increases to 53-54 cm at the age of 12. At 5-8 years old, the first traction occurs. But not all children grow in the same way – depending on a variety of factors, such as genetic ones. Children of undersized parents are usually smaller than their peers, but the processes of puberty they still occur on time. Faster growth than that of peers, with normal body proportions, is characteristic of children of tall parents. In some babies, the growth rate slows down from the second year of life, but after 2-3 years it accelerates again to normal. They have both growth and the onset of puberty delayed by a period during which growth was retarded, but final growth is in line with genetic potential. You must understand: the growth rate of the child should not correspond to any exact parameters, the criteria for “normality” are not at all rigid, but nevertheless, deviations in the growth rate of the child can also be pathological: for example, grossly out of proportion to age or accompanied by a violation of proportions body. Such cases require expert advice. It is also necessary to control body weight. As mentioned above, the lack and excess of body weight requires close monitoring of pediatricians, endocrinologists. In children with reduced body weight, there is a decrease in the immunological reactivity of the body, which leads to frequent colds. And excess everything is a risk factor for acquiring obesity in the future and all the serious diseases associated with it: atherosclerosis, heart disease, colon cancer, etc.
They have both growth and the onset of puberty delayed by a period during which growth was retarded, but final growth is in line with genetic potential. You must understand: the growth rate of the child should not correspond to any exact parameters, the criteria for “normality” are not at all rigid, but nevertheless, deviations in the growth rate of the child can also be pathological: for example, grossly out of proportion to age or accompanied by a violation of proportions body. Such cases require expert advice. It is also necessary to control body weight. As mentioned above, the lack and excess of body weight requires close monitoring of pediatricians, endocrinologists. In children with reduced body weight, there is a decrease in the immunological reactivity of the body, which leads to frequent colds. And excess everything is a risk factor for acquiring obesity in the future and all the serious diseases associated with it: atherosclerosis, heart disease, colon cancer, etc.
- Increase in the recommended amount of food;
- Quenching a child’s thirst with milk, sugary drinks or formula;
- Excessive (more than 50-100 ml per day) consumption of sweet fruit juices and nectars;
- Use of excess high-calorie foods – fat, sweets, baked cottage cheese;
- Calming the child with food;
- Familial overeating that distorts the child’s development of a real sense of need for food;
- Force-feeding, inculcating the habit of eating everything on the plate.


Your pediatrician and endocrinologist will be able to establish the correct diet, give recommendations on the daily diet. Please remember that in the second year of life, the pediatrician examines the child once a quarter, from the third year of life once every six months, in the fourth year and then once a year. Your child is between 10 and 15 years old. A uniform increase in the growth of preschoolers is replaced by its sharp acceleration in adolescence. At 10-13 years old (for girls) and at 12-15 years old (for boys) there is a second traction and at the same time an increase in body weight. The maximum growth rate in girls usually occurs at 12 years of age. The increase in height at this age is approximately 8 cm per year. The maximum increase in body weight in girls usually occurs later at 13 years of age. In boys, the maximum growth rate usually occurs at 14-15 years of age and is approximately 10 cm per year. The maximum increase in the body of a boy usually occurs with a maximum increase in height. The probable final height depends on the height of the parents. It can be calculated using the following formula: Boy’s height = 1/2 x (father’s height + mother’s height) + 6.5 cm Girl’s height = 1/2 x (father’s height + mother’s height) – 6.5 cm. Possible error must be taken into account – the final height can be 8.5 cm more or less.
The probable final height depends on the height of the parents. It can be calculated using the following formula: Boy’s height = 1/2 x (father’s height + mother’s height) + 6.5 cm Girl’s height = 1/2 x (father’s height + mother’s height) – 6.5 cm. Possible error must be taken into account – the final height can be 8.5 cm more or less.
Boys themselves and their parents are often concerned about the delay in growth acceleration, while girls, on the contrary, are worried about excessively rapid growth. However, you need to worry only if the child’s growth parameters differ significantly from the parameters indicated in special tables and graphs. In such a situation, it is necessary to contact an endocrinologist.
Remember – there are methods that can influence these processes. One of the most important features of the physical development of children and adolescents is the uneven change in growth rate. In children, the distal segments of the body grow at a faster rate and in a shorter time than the upper and proximal segments. So, for example, during the period of postnatal stretching, the child’s foot increases more significantly than the lower leg, and the lower leg – more than the thigh. Against this background, the increase in neck length or head height will be minimal. In certain periods, this feature of the child’s growth leads to a certain disproportion, some clumsiness in movements and gait. And only during puberty, the growth rate of the trunk will be much greater than the rate of stretching of the lower limbs. Thus, the physical development of children and adolescents should be constantly in the field of view of pediatricians and healthcare organizers. Physical development subtly reflects the health of the generation, the well-being of the environment, and makes it possible to predict the longevity and resilience of the population.
So, for example, during the period of postnatal stretching, the child’s foot increases more significantly than the lower leg, and the lower leg – more than the thigh. Against this background, the increase in neck length or head height will be minimal. In certain periods, this feature of the child’s growth leads to a certain disproportion, some clumsiness in movements and gait. And only during puberty, the growth rate of the trunk will be much greater than the rate of stretching of the lower limbs. Thus, the physical development of children and adolescents should be constantly in the field of view of pediatricians and healthcare organizers. Physical development subtly reflects the health of the generation, the well-being of the environment, and makes it possible to predict the longevity and resilience of the population.
Author of the material: pediatrician of the clinic on Nikulinskaya Ilyina I.D.
13.03.2017
Physical retardation is a significant lag of the child according to anthropometric criteria from their peers. Often this condition is characterized by a delay in the development of motor abilities and cognitive skills.
Often this condition is characterized by a delay in the development of motor abilities and cognitive skills.
Anthropometric data (height, weight, chest circumference, head circumference, etc.) are assessed using centile tables compiled specifically for children of different ages and genders. If the anthropometric data of a child go beyond the 3rd-5th centile, or for a short period of time there has been a significant decrease in them (for example, from a level of more than the 75th percentile to a level less than the 25th), we can talk about a delay in physical development. There is a traditional distinction between physical developmental delay due to the presence of diseases (organic) and physical developmental delay associated with psychological and social factors (psychosocial, inorganic), observed in children under the age of five.
Symptoms of delayed physical development of the child
The severity of manifestations can range from a slight delay in growth and body weight, to severe manifestations, including loss of the subcutaneous fat layer, reduction in muscle mass, dermatitis, hair loss, the development of recurrent infections.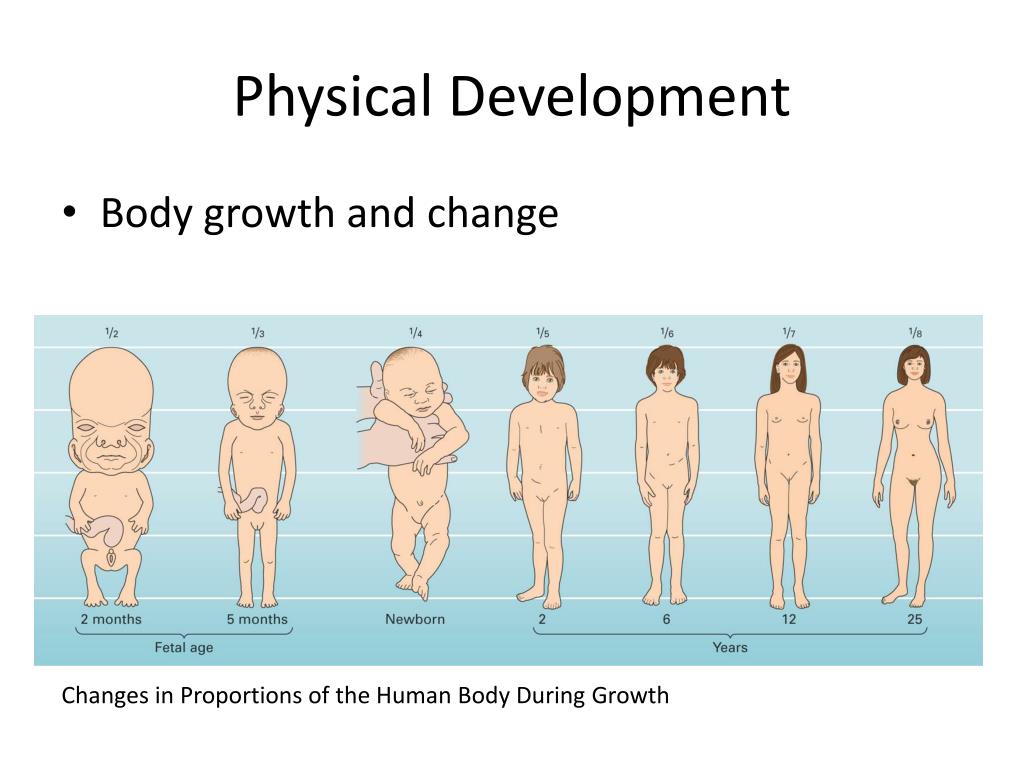 In the most severe cases, protein-energy (marasmus) or protein depletion (kwashiorkor) develops. Delayed physical development in developed countries is most often characterized by minimal impairments diagnosed in a polyclinic setting. In developing countries, more severe manifestations requiring inpatient treatment are more common.
In the most severe cases, protein-energy (marasmus) or protein depletion (kwashiorkor) develops. Delayed physical development in developed countries is most often characterized by minimal impairments diagnosed in a polyclinic setting. In developing countries, more severe manifestations requiring inpatient treatment are more common.
The degree of delay can be set for each anthropometric parameter (height, body weight, weight-height index) as a percentage of the average statistical age standards. In the presence of concomitant diseases, it is necessary to repeatedly determine anthropometric parameters in dynamics. In the case of premature babies, the degree of prematurity is also taken into account, since up to one or two years old, when comparing anthropometric data, it is necessary to adjust the age.
Lagging can be characterized as mild, moderate or severe with a body weight equal to 75-90, 60-74 and less than 60% of the due, height – 90-95, 85-89 and less than 85% of the due, weight-height index – 81 -90, 70-80 and less than 70% of the due. The lag in mass usually outstrips the lag in growth. In chronic malnutrition, there is a synchronous growth retardation and weight gain.
The lag in mass usually outstrips the lag in growth. In chronic malnutrition, there is a synchronous growth retardation and weight gain.
If physical development is delayed, laboratory examination is usually not very informative, therefore it is recommended to limit yourself to the most basic analyzes. These include general clinical tests of blood, urine, and blood. It is important to assess the bone age of the child. For this, an x-ray of the hands is performed with the capture of l / carpal joints. The presence of ossification points (nuclei) is analyzed. Bone age can correspond to the passport age, lag behind it or get ahead of it. Thanks to this study, it is possible to identify family short stature, in which the bone age corresponds to the passport one, to suggest the presence of endocrine diseases or dietary abnormalities, which makes it possible to determine the range of further examination.
Treatment of delayed physical development of a child
When making a diagnosis, it is necessary to take into account the history and clinical manifestations, as well as assess the relationship between the child and his parents, which plays an important role. For successful treatment, a thorough assessment of the child’s nutritional characteristics, identification of social problems, economic difficulties, and conflict situations in the family is required. It is necessary to promote the formation of a favorable atmosphere in the family, the preparation of a proper diet. With an organic delay in physical development, an important role is played by the correctly selected therapy of the underlying disease. Features of nutrition are determined by the severity of the delay in physical development, as well as the nature of the underlying disease.
For successful treatment, a thorough assessment of the child’s nutritional characteristics, identification of social problems, economic difficulties, and conflict situations in the family is required. It is necessary to promote the formation of a favorable atmosphere in the family, the preparation of a proper diet. With an organic delay in physical development, an important role is played by the correctly selected therapy of the underlying disease. Features of nutrition are determined by the severity of the delay in physical development, as well as the nature of the underlying disease.
Hospitalization is carried out in case of a pronounced delay in physical development, in case of exhaustion, the need for examination, and also when there are suspicions of the inadequacy of the attitude of parents towards their child. If the reason for the delay is a disease, a selection of therapy is carried out in the hospital.
By contacting our CMC, you can be sure of professional and high-quality assistance from our leading specialists.