






How long does your first period last on nexplanon: Changes to Your Period on NEXPLANON® (etonogestrel implant) 68 mg Radiopaque
Bleeding Pattern Changes and NEXPLANON® (etonogestrel implant) 68 mg
Bleeding Pattern Changes and NEXPLANON® (etonogestrel implant) 68 mg
This site is intended for US health care professionals.
Bleeding Pattern Changes
Bleeding and spotting episodes
Based on data from clinical trials of the non-radiopaque etonogestrel implant (IMPLANON®):
- Women who use NEXPLANON are likely to have changes in their vaginal bleeding patterns. These may include changes in bleeding frequency, intensity, duration, or amenorrhea.
- The bleeding pattern experienced during the first 3 months using NEXPLANON is broadly predictive of the future bleeding pattern for many women.
Bleeding and spotting prevalence
Based on data from clinical trials of the non-radiopaque etonogestrel implant (IMPLANON®):
- In clinical trials
- Women had an average of 17.
7 days of bleeding or spotting every 90 days (N=780)
- 11.1% of women discontinued due to changes in bleeding pattern (N=942)
- Women had an average of 17.
- Abnormal bleeding should be evaluated as needed to exclude pathologic conditions or pregnancy
Percentages of patients with 0, 1–7, 8–21, or >21 days of spotting or bleeding over a 90-day interval while using the non-radiopaque etonogestrel implant (IMPLANON®)
| Total days of spotting or bleeding | Percentage of women | ||
|---|---|---|---|
| Treatment days 91–190 (N=745) | Treatment days 271–360 (N=657) | Treatment days 631–720 (N=547) | |
| 0 days | 19% | 24% | 17% |
| 1–7 days | 15% | 13% | 12% |
| 8–21 days | 30% | 30% | 37% |
| >21 days | 35% | 33% | 35% |
Indications and
Selected Safety Information
Indications
NEXPLANON is indicated for use by women to prevent pregnancy.
Selected Safety Information
CONTRAINDICATIONS
- NEXPLANON should not be used in women who have known or suspected pregnancy; current or past history of thrombosis or thromboembolic disorders; liver tumors, benign or malignant, or active liver disease; undiagnosed abnormal genital bleeding; known or suspected breast cancer, personal history of breast cancer, or other progestin-sensitive cancer, now or in the past; and/or allergic reaction to any of the components of NEXPLANON.
WARNINGS AND PRECAUTIONS
Complications of Insertion and Removal
- NEXPLANON should be inserted subdermally so that it will be palpable after insertion, and this should be confirmed by palpation immediately after insertion. Failure to insert NEXPLANON properly may go unnoticed unless it is palpated immediately after insertion. Undetected failure to insert the implant may lead to an unintended pregnancy. Failure to remove the implant may result in continued effects of etonogestrel, such as compromised fertility, ectopic pregnancy, or persistence or occurrence of a drug-related adverse event.

- Complications related to insertion and removal procedures, such as pain, paresthesias, bleeding, hematoma, scarring, or infection, may occur. If NEXPLANON is inserted deeply (intramuscular or in the fascia), neural or vascular injury may occur. Implant removal may be difficult or impossible if the implant is not inserted correctly, inserted too deeply, not palpable, encased in fibrous tissue, or has migrated. If at any time the implant cannot be palpated, it should be localized and removal is recommended.
- There have been postmarketing reports of implants located within the vessels of the arm and the pulmonary artery, which may be related to deep insertions or intravascular insertions. Endovascular or surgical procedures may be needed for removal.

Changes in Menstrual Bleeding Patterns
- After starting NEXPLANON, women are likely to have changes in their menstrual bleeding pattern. These may include changes in frequency, intensity, or duration. Abnormal bleeding should be evaluated as needed to exclude pathologic conditions or pregnancy. In clinical studies of the non-radiopaque etonogestrel implant, reports of changes in bleeding pattern were the most common reason for stopping treatment (11.1%). Women should be counseled regarding bleeding pattern changes that they may experience.
 Abnormal bleeding should be evaluated as needed to exclude pathologic conditions or pregnancy. In clinical studies of the non-radiopaque etonogestrel implant, reports of changes in bleeding pattern were the most common reason for stopping treatment (11.1%). Women should be counseled regarding bleeding pattern changes that they may experience.
Abnormal bleeding should be evaluated as needed to exclude pathologic conditions or pregnancy. In clinical studies of the non-radiopaque etonogestrel implant, reports of changes in bleeding pattern were the most common reason for stopping treatment (11.1%). Women should be counseled regarding bleeding pattern changes that they may experience.Ectopic Pregnancies
- Be alert to the possibility of an ectopic pregnancy in women using NEXPLANON who become pregnant or complain of lower abdominal pain.
Thrombotic and Other Vascular Events
- The use of combination hormonal contraceptives increases the risk of vascular events, including arterial events (strokes and myocardial infarctions) or deep venous thrombotic events (venous thromboembolism, deep venous thrombosis, retinal vein thrombosis, and pulmonary embolism). It is recommended that women with risk factors known to increase the risk of venous and arterial thromboembolism be carefully assessed. There have been postmarketing reports of serious arterial thrombotic and venous thromboembolic events, including cases of pulmonary emboli (some fatal), deep vein thrombosis, myocardial infarction, and strokes, in women using etonogestrel implants. NEXPLANON should be removed in the event of a thrombosis. Due to the risk of thromboembolism associated with pregnancy and immediately following delivery, NEXPLANON should not be used prior to 21 days postpartum. Women with a history of thromboembolic disorders should be made aware of the possibility of a recurrence. Consider removal of the NEXPLANON implant in case of long-term immobilization due to surgery or illness.
 There have been postmarketing reports of serious arterial thrombotic and venous thromboembolic events, including cases of pulmonary emboli (some fatal), deep vein thrombosis, myocardial infarction, and strokes, in women using etonogestrel implants. NEXPLANON should be removed in the event of a thrombosis. Due to the risk of thromboembolism associated with pregnancy and immediately following delivery, NEXPLANON should not be used prior to 21 days postpartum. Women with a history of thromboembolic disorders should be made aware of the possibility of a recurrence. Consider removal of the NEXPLANON implant in case of long-term immobilization due to surgery or illness.
There have been postmarketing reports of serious arterial thrombotic and venous thromboembolic events, including cases of pulmonary emboli (some fatal), deep vein thrombosis, myocardial infarction, and strokes, in women using etonogestrel implants. NEXPLANON should be removed in the event of a thrombosis. Due to the risk of thromboembolism associated with pregnancy and immediately following delivery, NEXPLANON should not be used prior to 21 days postpartum. Women with a history of thromboembolic disorders should be made aware of the possibility of a recurrence. Consider removal of the NEXPLANON implant in case of long-term immobilization due to surgery or illness.Ovarian Cysts
- If follicular development occurs, atresia of the follicle is sometimes delayed, and the follicle may continue to grow beyond the size it would attain in a normal cycle. Generally, these enlarged follicles disappear spontaneously. Rarely, surgery may be required.
Carcinoma of the Breast and Reproductive Organs
- Some studies suggest that the use of combination hormonal contraceptives might increase the incidence of breast cancer, and increase the risk of cervical cancer or intraepithelial neoplasia. Women with a family history of breast cancer or who develop breast nodules should be carefully monitored.
 Women with a family history of breast cancer or who develop breast nodules should be carefully monitored.
Women with a family history of breast cancer or who develop breast nodules should be carefully monitored.Liver Disease
- NEXPLANON should be removed if jaundice occurs.
Elevated Blood Pressure
- The NEXPLANON implant should be removed if blood pressure rises significantly and becomes uncontrolled.
Gallbladder Disease
- Studies suggest a small increased relative risk of developing gallbladder disease among combination hormonal contraceptive users. It is not known whether a similar risk exists with progestin-only methods like NEXPLANON.
Carbohydrate and Lipid Metabolic Effects
- Prediabetic and diabetic women using NEXPLANON should be carefully monitored.
Depressed Mood
- Women with a history of depressed mood should be carefully observed. Consideration should be given to removing NEXPLANON in patients who become significantly depressed.
Return to Ovulation
- In clinical trials with the non-radiopaque etonogestrel implant (IMPLANON), the etonogestrel levels in blood decreased below sensitivity of the assay by one week after removal of the implant. In addition, pregnancies were observed to occur as early as 7 to 14 days after removal. Therefore, a woman should re-start contraception immediately after removal of the implant if continued contraceptive protection is desired.
Fluid Retention
- Hormonal contraceptives may cause some degree of fluid retention. They should be prescribed with caution, and only with careful monitoring, in patients with conditions which might be aggravated by fluid retention. It is unknown if NEXPLANON causes fluid retention.
Contact Lenses
- Contact lens wearers who develop visual changes or changes in lens tolerance should be assessed by an ophthalmologist.
Broken or Bent Implant
- There have been reports of broken or bent implants, which may be related to external forces (e. g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm. Based on in vitro data, when an implant is broken or bent, the release rate of etonogestrel may be slightly increased. When an implant is removed, it is important to remove it in its entirety.
 g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm. Based on in vitro data, when an implant is broken or bent, the release rate of etonogestrel may be slightly increased. When an implant is removed, it is important to remove it in its entirety.
g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm. Based on in vitro data, when an implant is broken or bent, the release rate of etonogestrel may be slightly increased. When an implant is removed, it is important to remove it in its entirety.ADVERSE REACTIONS
Clinical Trial Experience
- The most common adverse reaction causing discontinuation of use of the implant in clinical trials was change in menstrual bleeding patterns, specifically irregular menses (11.1%). The most common adverse reactions (≥10%) reported in clinical trials were headache (24.9%), vaginitis (14.5%), weight increase (13.7%), acne (13.5%), breast pain (12.8%), abdominal pain (10.9%), and pharyngitis (10.5%).
Effects of Other Drugs on Hormonal Contraceptives
Substances decreasing the plasma concentrations of hormonal contraceptives and potentially diminishing the efficacy of hormonal contraceptives:
- Drugs or herbal products that induce certain enzymes, including cytochrome P450 3A4 (CYP3A4), may decrease the plasma concentrations of hormonal contraceptives and potentially diminish the effectiveness of hormonal contraceptives or increase breakthrough bleeding. Women should use an alternative non-hormonal method of contraception or a back-up method when enzyme inducers are used with hormonal contraceptives, and to continue back-up non-hormonal contraception for 28 days after discontinuing the enzyme inducer to ensure contraceptive reliability.
 Women should use an alternative non-hormonal method of contraception or a back-up method when enzyme inducers are used with hormonal contraceptives, and to continue back-up non-hormonal contraception for 28 days after discontinuing the enzyme inducer to ensure contraceptive reliability.
Women should use an alternative non-hormonal method of contraception or a back-up method when enzyme inducers are used with hormonal contraceptives, and to continue back-up non-hormonal contraception for 28 days after discontinuing the enzyme inducer to ensure contraceptive reliability.Substances increasing the plasma concentrations of hormonal contraceptives:
- Co-administration of certain hormonal contraceptives and strong or moderate CYP3A4 inhibitors may increase the serum concentrations of progestins, including etonogestrel.
Human Immunodeficiency Virus (HIV)/Hepatitis C Virus (HCV) protease inhibitors and non-nucleoside reverse transcriptase inhibitors:
- Significant changes (increase or decrease) in the plasma concentrations of progestin have been noted in cases of co-administration with HIV protease inhibitors, HCV protease inhibitors, or with non-nucleoside reverse transcriptase inhibitors. These changes may be clinically relevant.
Effects of Hormonal Contraceptives on Other Drugs
- Hormonal contraceptives may affect the metabolism of other drugs. Consequently, plasma concentrations may either increase (for example, cyclosporine) or decrease (for example, lamotrigine).
USE IN SPECIFIC POPULATIONS
Pregnancy
- Rule out pregnancy before inserting NEXPLANON.
Lactation
- Small amounts of contraceptive steroids and/or metabolites, including etonogestrel are present in human milk. No significant adverse effects have been observed in the production or quality of breast milk, or on the physical and psychomotor development of breastfed infants.
- Hormonal contraceptives, including etonogestrel, can reduce milk production in breastfeeding mothers. This is less likely to occur once breastfeeding is well-established; however, it can occur at any time in some women.
Pediatric Use
- Safety and efficacy of NEXPLANON have been established in women of reproductive age and are expected to be the same for postpubertal adolescents. However, no studies have been conducted in women less than 18 years of age. Use of this product before menarche is not indicated.
 However, no studies have been conducted in women less than 18 years of age. Use of this product before menarche is not indicated.
However, no studies have been conducted in women less than 18 years of age. Use of this product before menarche is not indicated.Overweight Women
- The efficacy of NEXPLANON in women who weighed more than 130% of their ideal body weight has not been defined because such women were not studied in clinical trials. Serum concentrations of etonogestrel are inversely related to body weight and decrease with time after implant insertion. Therefore, NEXPLANON may be less effective in overweight women.
PATIENT COUNSELING INFORMATION
- Counsel women to contact their health care provider immediately if, at any time, they are unable to palpate the implant.
- NEXPLANON does not protect against HIV or other STDs.
Before prescribing NEXPLANON, please read the accompanying Prescribing Information. The Patient Information also is available.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Arcu arcu in dictum eu blandit amet proin netus. Nulla mattis vitae fringilla purus dolor convallis urna. Lectus ut lacus a rutrum.
Arcu arcu in dictum eu blandit amet proin netus. Nulla mattis vitae fringilla purus dolor convallis urna. Lectus ut lacus a rutrum.
Contraceptive implant | NHS inform
The contraceptive implant is a thin, flexible rod about 4cm long. It’s inserted under the skin of your upper arm by a professional.
The implant stops the release of an egg from the ovary by slowly releasing progestogen into your body. Progestogen also thickens the cervical mucus and thins the womb lining. This makes it harder for sperm to move through your cervix, and less likely for your womb to accept a fertilised egg.
At a glance: the implant
If implanted correctly, it’s more than 99% effective. Fewer than 1 woman in 1,000 who have the implant as contraception for 3 years will get pregnant.
It’s very useful for women who know they don’t want to get pregnant for a while. Once the implant is in place, you don’t have to think about contraception for 3 years.
It can be useful for women who can’t use contraception that contains oestrogen.
It’s very useful for women who find it difficult to take a pill at the same time every day.
If you have side effects or want to have a baby, the implant can be taken out.
Your natural fertility returns very quickly after removal.
When it’s first put in, you may feel some bruising, tenderness or swelling around the implant.
In the first year after the implant is fitted, your periods may become irregular, lighter, heavier or longer. This usually settles down after a few months.
Your periods may stop (amenorrhoea). This isn’t harmful.
Some medications can make the implant less effective. You should use extra contraception when taking these medications.
The implant does not protect against sexually transmitted infections (STIs). Use condoms as well as the implant to protect yourself against STIs.
There is no evidence to show that the implant causes weight gain.
How the implant works
The implant steadily releases the hormone progestogen into your bloodstream. Progestogen is like the natural hormone progesterone.
Progestogen is like the natural hormone progesterone.
The continuous release of progestogen:
- stops a woman releasing an egg every month (ovulation)
- thickens the mucus from the cervix (entrance to the womb), making it difficult for sperm to pass through to the womb and reach an unfertilised egg
- makes the lining of the womb thinner so that it is unable to support a fertilised egg
The implant can be put in at any time during your menstrual cycle, as long as you and your doctor are reasonably sure you are not pregnant. In Scotland, Nexplanon is the only contraceptive implant currently in use.
Nexplanon is a small, thin, flexible tube about 4cm long. It’s implanted under the skin of your upper arm by a doctor or nurse. A local anaesthetic is used to numb the area. The small wound made in your arm is closed with a dressing and does not need stitches. Nexplanon works for 3 years.
The implant can be removed at any time by a specially trained doctor or nurse. It only takes a few minutes to remove, using a local anaesthetic. As soon as the implant has been removed, you’ll no longer be protected against pregnancy.
It only takes a few minutes to remove, using a local anaesthetic. As soon as the implant has been removed, you’ll no longer be protected against pregnancy.
When it starts to work
If the implant is fitted during the first 5 days of your menstrual cycle, you’ll be immediately protected against becoming pregnant. If it’s fitted on any other day of your menstrual cycle, you will not be protected against pregnancy for up to 7 days. You should use another method during this time, such as condoms.
After giving birth
You can have the contraceptive implant fitted after you have given birth, usually after 3 weeks.
If it’s fitted on or before day 21 after the birth, you’ll be immediately protected against becoming pregnant.
If it’s fitted after day 21, you’ll need to use extra contraception, such as condoms, for the following 7 days.
It’s safe to use the implant while you are breastfeeding.
After a miscarriage or abortion
The implant can be fitted immediately after a miscarriage or an abortion, and you’ll be protected against pregnancy straight away.
Who can use the implant?
Most women can be fitted with the contraceptive implant. It may not be suitable if you don’t want irregular bleeding, or if you have a hormone dependent cancer such as breast cancer.
Advantages and disadvantages of the implant
The main advantages of the contraceptive implant are:
- it works for 3 years
- it does not interrupt sex
- it’s suitable if you can’t use oestrogen-based contraception, such as the combined contraceptive pill, contraceptive patch or vaginal ring
- you don’t have to remember to take a pill every day
- it’s safe to use while you are breastfeeding
- your fertility should return to normal as soon as the implant is removed
- after the contraceptive implant has been inserted, you should be able to carry out normal activities
Disadvantages
Using a contraceptive implant may have some disadvantages. You should consider these carefully before deciding if it’s right for you.
Your periods may change significantly while using a contraceptive implant. Around 20% of women using the implant will have no bleeding, but almost 50% will have infrequent or prolonged bleeding. Bleeding patterns often remain irregular.
These changes are not harmful. If the bleeding is a problem, your GP may be able to give you tablets to help.
Other side effects that some women report are:
- headaches
- acne
- nausea
- breast tenderness
- changes in mood
- loss of sex drive
These side effects usually stop after the first few months. If you have prolonged or severe headaches or other side effects, tell your doctor.
Will other medicines affect the implant?
Some medicines can reduce the implant’s effectiveness. These include:
- medication for HIV
- medication for epilepsy
- complementary remedies, such as St John’s Wort
- an antibiotic called rifabutin (which can be used to treat tuberculosis)
- an antibiotic called rifampicin (which can be used to treat several conditions, including tuberculosis and meningitis)
These are called enzyme-inducing drugs. If you are using these medicines for a short while, you should use extra contraception during the course of treatment and for 28 days afterwards. The extra contraception could be condoms, or a single dose of the contraceptive injection. The implant can remain in place if you have the injection.
If you are using these medicines for a short while, you should use extra contraception during the course of treatment and for 28 days afterwards. The extra contraception could be condoms, or a single dose of the contraceptive injection. The implant can remain in place if you have the injection.
If you’re taking enzyme-inducing drugs long term, you may prefer another method of contraception.
Always tell your doctor that you are using an implant if you are prescribed any medicines. Ask your doctor or nurse for more details about the implant and other medication.
Risks of the implant
In rare cases, the area of skin where the implant has been fitted can become infected. If this happens, the area will be cleaned and may be treated with antibiotics.
Where can you get the implant?
Most types of contraception are available for free in the UK. Contraception is free to all women and men through the NHS. Places where you can get contraception include:
- most GP practices – talk to your GP or practice nurse as not all practices fit implants
- sexual health clinics – they also offer contraceptive and STI testing services
- some young people’s services
Implants are usually removed by the service or practice where it was fitted. If not, your GP or sexual health service can advise on where implants removal is provided in your area.
If not, your GP or sexual health service can advise on where implants removal is provided in your area.
Contraception services are free and confidential, including for people under the age of 16.
If you’re under 16 and want contraception, the doctor, nurse or pharmacists won’t tell your parents (or carer). They’ll provide you with contraception as long as they believe you fully understand the information you’re given and are able to use the contraception safely.
Doctors and nurses have a responsibility to make sure that you are safe and free from harm. They’ll encourage you to consider telling your parents (or carer), but they won’t make you. The only time that a professional will not be able to keep confidentiality is if they believe you’re at risk of serious harm, such as abuse. If this was the case they would usually discuss it with you first.
The period of the first menstruation: how long does the first menstruation last
Features of the cycle immediately after the first menstruation
The first menstruation (menarche) in girls usually begins at the age of 11-14 years. Such a rather large variation is explained by the fact that the physiological characteristics of the structure of the adolescent’s organism, which are inherited, as well as some other factors, can affect the time of the onset of menstruation. During the first period, bleeding is usually weak and short – only about 2-3 days. How long the first menstruation lasts is affected by the girl’s health, physique, etc.
Such a rather large variation is explained by the fact that the physiological characteristics of the structure of the adolescent’s organism, which are inherited, as well as some other factors, can affect the time of the onset of menstruation. During the first period, bleeding is usually weak and short – only about 2-3 days. How long the first menstruation lasts is affected by the girl’s health, physique, etc.
After that, there comes a period when the cycle is irregular (that is, menstruation comes a few days earlier, sometimes later). This is due to the fact that the process of production of female hormones in the body stabilizes for about a year. At this age, it is impossible to say exactly how many days the girl’s first period will go: in general, this value ranges from 3 to 5 days.
Usually around 14-15 years of age, the menstrual cycle becomes stable. From now on, every girl is advised to keep track of when menstruation occurs and how long they last. If your periods are too short (less than 2 days) or too long (more than 7 days), you should visit a gynecologist.
How many days does a normal cycle last?
Many believe that the duration of the menstrual cycle (the time from the onset of one bleeding to the onset of another) should be exactly 28 days, but this is a delusion. Its duration is individual for each woman and can change throughout life. Normally, the duration of the menstrual cycle is from 21 days and no more than 35 days. If your cycles last less than 21 or more than 35 days, you should consult a gynecologist, because this situation may be a signal of a malfunction of the ovaries.
It is also necessary that the cycle is regular. Some girls face a problem when they cannot predict the time of the next menstruation. This phenomenon is normal for young girls immediately after menarche and for women after childbirth, but in all other cases this may indicate a violation in the body. These may include, for example, the consequences of nervous tension, inflammatory diseases, etc.
Possible deviations
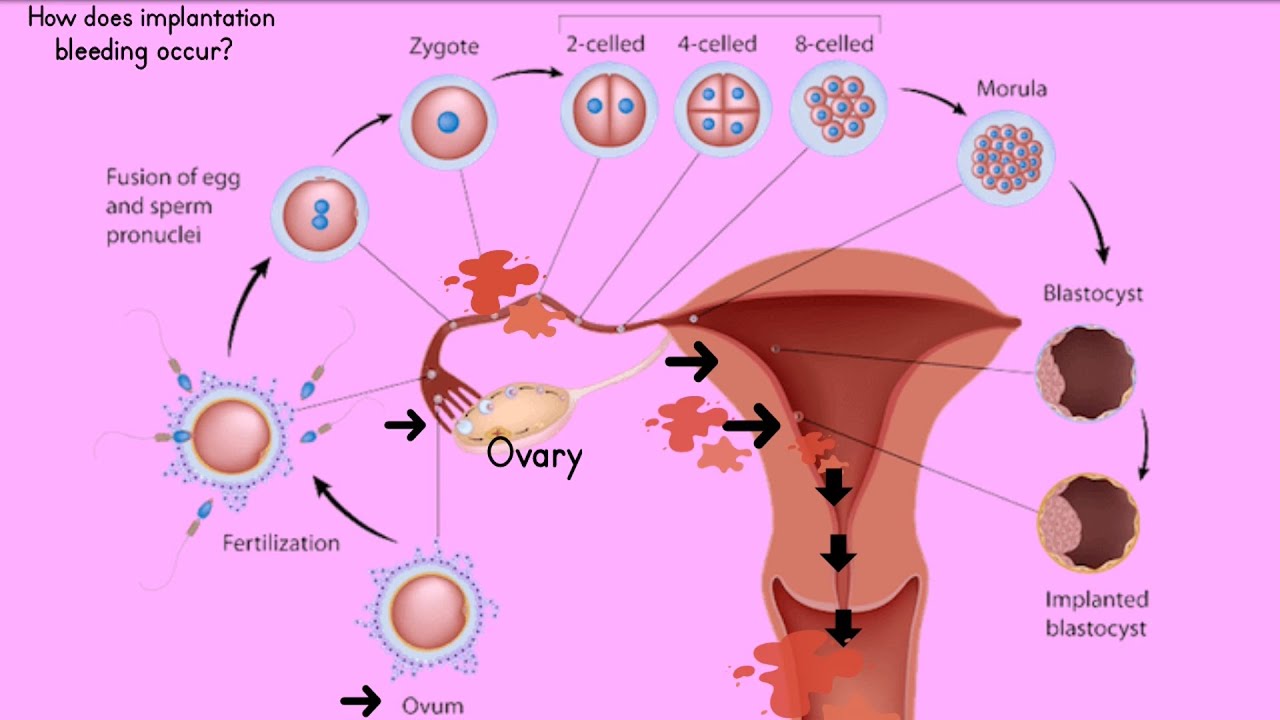
Girls. Adolescent girls may experience light spotting a few days before and after their period. They usually disappear by themselves at the age of 15-16, after which they never appear again. However, if such “extraordinary” discharges are noticed at a later age, this may be a sign that the cycle is seriously disturbed as a result of physiological changes. The causes may be inflammatory diseases of the pelvic organs, various neoplasms, etc. In addition, discharge may be a sign of the so-called implantation bleeding – one of the signs of pregnancy. 1
Adolescent girls may experience light spotting a few days before and after their period. They usually disappear by themselves at the age of 15-16, after which they never appear again. However, if such “extraordinary” discharges are noticed at a later age, this may be a sign that the cycle is seriously disturbed as a result of physiological changes. The causes may be inflammatory diseases of the pelvic organs, various neoplasms, etc. In addition, discharge may be a sign of the so-called implantation bleeding – one of the signs of pregnancy. 1
Women. Violation of the duration of menstruation and the duration of the cycle often occurs after childbirth. The absence of bleeding in the first months and irregular periods throughout the year are quite normal for this period. 2 Menstruation can be irregular not only in girls after menarche, as mentioned above, but also in women after 55 years of age during menopause. At this age, the reproductive function gradually fades and over time, menstruation completely stops.
Literature
- Kuznetsova I.V., Bril Yu.A., Simonovskaya Kh.Yu. Retrochorial hematomas. Evolution of Consciousness I.M. Sechenov First Moscow State Medical University StatusPraesens. Gynecology, obstetrics, barren marriage. 2015; 5(28): 89-95
- Jabbarova Yu.K., Rakhmankulova N.G. Lactational amenorrhea as a method of postpartum contraception Tashkent Medical Academy ENJ “Biology and Integrative Medicine”. 2016; 5 (September-October) *https://cyberleninka.ru/article/n/laktatsionnaya-amenoreya-kak-sposob-poslerodovoy-kontratseptsii/viewer*
First period in girls: when it starts, signs, what to do
Why do menstruation occur?
The causes of menarche lie in the hormonal changes that occur in the body during puberty 1.2 .
The brain has a small but very important gland – the hypothalamus, which controls the work of the entire endocrine system 1,2 . When a girl enters adolescence, her hypothalamus releases releasing factors (from the English. Release – release) into the blood and thereby starts the process of puberty 1.2 .
Release – release) into the blood and thereby starts the process of puberty 1.2 .
Releasing factors act on another gland of the brain – the pituitary gland, which, in turn, begins to synthesize luteinizing hormone (LH) and follicle-stimulating hormone (FSH) 1.2 . It is they who activate the work of the ovaries and the production of sex hormones estrogen and progesterone.
Under the influence of estrogen and progesterone, the uterus prepares for pregnancy every month. The inner mucosa of the uterus grows, loosens and turns into a “feather bed”, ready at any moment to receive a fetal egg. If pregnancy does not occur, the uterus gets rid of the unnecessary inner layer, it comes out along with the menstrual blood and everything starts all over again.
Harbingers of the first menstruation:
Female sex hormones – estrogens and progesterone – constantly circulate in the blood of a woman in different amounts 1.2 . In addition to the uterus, they affect other organs and systems 1. 2 . You will notice changes in them much earlier than the menarche happens. Moreover, by their appearance you will be able to judge how soon the first menstruation will be.
2 . You will notice changes in them much earlier than the menarche happens. Moreover, by their appearance you will be able to judge how soon the first menstruation will be.
| Breast engorgement | the very first sign that you are going through puberty 2 . The nipple becomes convex and slightly enlarged in diameter – this usually occurs 2 years before menarche 2.3 . For doctors, this is a kind of benchmark. If menstruation does not start, there is cause for alarm 3 |
| The appearance of pubic hairs | the second harbinger of menstruation in girls. Usually the first hairs “break through” simultaneously with the enlargement of the nipples 2 . But in the armpits, hair appears much later – about six months before menarche 2 |
| Growth spurt | occurs approximately one and a half years before the first menstruation 2 . During this period, you may become much taller than your peers with a later onset of sexual development. As soon as the growth slows down, wait for the first menstruation 2 During this period, you may become much taller than your peers with a later onset of sexual development. As soon as the growth slows down, wait for the first menstruation 2 |
| Unreasonable health changes | weakness, daytime drowsiness, sudden mood swings, headaches, light dizziness, nausea, severity and even pain in the abdomen may indicate an approaching menstruation. These are not necessarily signs, but in some women they appear regularly a few days before menstruation 3 |
- tampons absorb fluid inside the body, avoiding odor and discomfort;
- tampons are an invisible protection because they are invisible under clothes and are not felt inside the body;
- tampons reliably protect against leakage during menstruation;
- tampons make it possible to lead an active lifestyle (play sports, dance and even swim).
At what age do girls start menstruating?
In girls of European race, the age of menarche often occurs at 12-13 years, less often menstruation occurs at 10-11 years and 13-14 years 1,2,3 . In the last 100-150 years, scientists have observed a marked decrease in the age at which puberty begins2. Therefore, menstruation in a girl of 9-10 years old no longer frightens doctors and parents 2.3 . Rather, the absence of menstruation at the age of 14.5 years is alarming 2.3 .
In the last 100-150 years, scientists have observed a marked decrease in the age at which puberty begins2. Therefore, menstruation in a girl of 9-10 years old no longer frightens doctors and parents 2.3 . Rather, the absence of menstruation at the age of 14.5 years is alarming 2.3 .
All the figures we have given are averages. Yours might be a little different. Many factors influence the onset of menarche:
- Genetics. If your mother’s menstruation started later than her peers, then there is a chance that you will have to wait a bit 2 .
- Race. Early menarche is typical for representatives of the Negroid race, Hispanics, and for Caucasians and Asians, menstruation begins later 2 .
- Nutrition. Good nutrition promotes the formation of menstruation, but the diet delays puberty 2 .
- Body weight. Slightly plump girls have periods earlier than 2 . But if the body weight significantly exceeds the norm, there is a delay in the appearance of menstruation 2
What are the first periods?
Menstruation can last from 2 to 7 days – all individually 2. 3 . When menstruation just begins, there is little blood from the vagina and it has a dark red color. Then it becomes larger, and it becomes brighter. Sometimes, if menstruation is heavy, small blood clots sometimes appear in the discharge. There is no need to worry about this: in this way the body limits blood loss 2 .
3 . When menstruation just begins, there is little blood from the vagina and it has a dark red color. Then it becomes larger, and it becomes brighter. Sometimes, if menstruation is heavy, small blood clots sometimes appear in the discharge. There is no need to worry about this: in this way the body limits blood loss 2 .
In the last days of menstruation, the amount of discharge decreases, they again become dark, sometimes almost black. This happens because little blood is released from the uterus, it is retained in the vagina and oxidized 2.3 .
How much blood is released during menstruation? All girls are different. Some lose only 20 ml of blood per day 3 . In others, the volume of blood loss approaches 80 ml 3 . On average, the amount of blood lost per day is 30 ml 3 , which is about the amount that 4 small 2 o.b.® swabs can absorb. Over time, you will learn how to select hygiene products, taking into account your individual characteristics. And in order not to miss the beginning of menstruation, we recommend that you use
And in order not to miss the beginning of menstruation, we recommend that you use
on days when discharge may begin. They will protect your clothes and make you feel more confident.
Periods come cyclically, about once a month. The interval between the first day of one menstruation and the first day of the next menstruation is called the menstrual cycle.0019 1 . Its duration can be from 21 to 35 days 3 . At the same time, each woman’s cycle should be stable with a fluctuation of +/- 2 days 3 .
The first 12-18 months after menarche, menstruation is often irregular, the interval between them can either be shortened or lengthened up to 45 days 3 . The nature of menstruation can also change. At first they are often profuse and painful 3 . But gradually, within 2-3 years, everything returns to normal 3 .
To control your cycle, we recommend that you keep a special menstruation diary or use an application on your phone for this, and in the event of “abnormal” situations, always contact your mother or doctor.