






Empty uterus at 7 weeks: Blighted Ovum (Anembryonic Pregnancy): Causes & Symptoms
Blighted Ovum (Anembryonic Pregnancy): Causes & Symptoms
Overview
A blighted ovum is when the gestational sac containing the embryo is empty.
What is a blighted ovum?
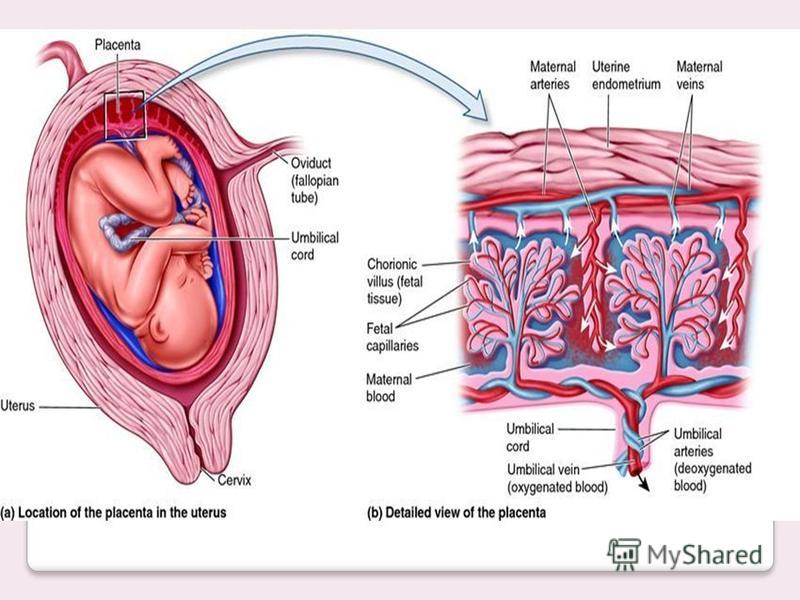
A blighted ovum (also called an anembryonic pregnancy) is a type of early miscarriage that occurs when a fertilized egg implants into the uterus but does not develop into an embryo. The embryo will stop growing, but the gestational sac (where the embryo would develop) continues to grow. The placenta and empty gestational sac will release pregnancy hormones — even without an embryo present. This causes you to have early symptoms of pregnancy or even have a positive pregnancy test. Sometimes it occurs so early in pregnancy that you don’t know you’re pregnant.
When does a blighted ovum happen?
A blighted ovum causes an early miscarriage in the first trimester of pregnancy. During fetal development, a fertilized egg turns into a blastocyte. At around four weeks of pregnancy, this blastocyte implants in the wall of the uterus and develops into an embryo. When you have a blighted ovum, the gestational sac that would hold the embryo continues to grow, even without an embryo present. The following can occur:
- A blighted ovum happens so early in pregnancy, that you never realize you are pregnant.
- You have a positive pregnancy test and signs of pregnancy only to discover a blighted ovum at your first ultrasound.
- You have a positive pregnancy test and signs of pregnancy but then experience a miscarriage.
How common is a blighted ovum pregnancy?
A blighted ovum is the number one cause of first trimester miscarriages.
Symptoms and Causes
What are the symptoms of a blighted ovum?
A blighted ovum can occur so early in pregnancy that you never knew you were pregnant. In other cases, you may experience signs of pregnancy such as a missed menstrual period or a positive pregnancy test. You can have symptoms of early pregnancy, such as breast tenderness and morning sickness.
Other times your symptoms will resemble those of a miscarriage:
- Vaginal bleeding: Spotting (light bleeding), bleeding or passing light gray tissue or blood clots.

- Cramping: Mild to moderate cramping in your pelvic and abdominal region.

The only way to confirm a blighted ovum is through an ultrasound. It will show a gestational sac that is missing an embryo inside.
What causes a blighted ovum?
A blighted ovum is usually caused by chromosomal or genetic problems during cell division. During conception, the egg will begin to divide shortly after being fertilized by sperm. Around ten days later, the cells have formed an embryo. With a blighted ovum, the embryo never forms or stops growing after it’s formed.
How does a blighted ovum miscarriage start?
A blighted ovum miscarriage will cause vaginal bleeding and abdominal cramping. A miscarriage usually feels more intense than your regular menstrual period. You can take an over-the-counter medicine like acetaminophen to relieve cramping. Avoid lifting anything heavy or any strenuous exercise as it can increase your bleeding. You may experience spotting for several weeks after a miscarriage.
Diagnosis and Tests
How is a blighted ovum diagnosed?
Your healthcare provider will diagnose a blighted ovum using transvaginal ultrasound. This happens in the first trimester, usually between seven and nine weeks of pregnancy. An embryo should be visible at this time in pregnancy. With a blighted ovum, the gestational sac will be empty.
- You will lie back on an exam table and place your feet in stirrups like you do for a pelvic exam. Your healthcare provider will put an ultrasound wand into your vagina to see the contents of your uterus.
- A blighted ovum will appear as an empty sac — almost like a bubble.
A blighted ovum is when the gestational sac containing the embryo is empty.
People are often unaware that they have a blighted ovum. This is because your placenta continues to give off hormones, making your body think you are pregnant. This is also why you can still have symptoms of pregnancy, including a positive pregnancy test.
If you’ve already experienced bleeding or signs of a miscarriage, your healthcare provider will use ultrasound to look at the contents of your uterus to diagnose a blighted ovum.
Some healthcare providers will collect a series of blood samples that check the levels of hCG (human chorionic gonadotropin) in your body. HCG is known as the pregnancy hormone because it’s only produced if you are pregnant. The level of hCG in your blood increases rapidly in early pregnancy and reaches its peak around weeks eight to ten. If it’s not rising quickly, it can indicate a miscarriage or other complication. Your provider may decide to test your hCG levels over the course of several days to evaluate how your hCG levels are rising. This can be an effective tool for diagnosing blighted ovum.
Management and Treatment
How is a blighted ovum treated?
For some people, there may be no treatment needed, because your body passes the embryo through your vagina (a miscarriage). If your body does not miscarry the embryo, there are other options to remove the contents of your uterus. Your healthcare provider will talk you through possible treatments:
If your body does not miscarry the embryo, there are other options to remove the contents of your uterus. Your healthcare provider will talk you through possible treatments:
- Dilation & Curettage (D&C): This is a surgical procedure to remove the contents of your uterus. Your healthcare provider will dilate, or open, the cervix and use medical tools and suction to remove the pregnancy tissues from your uterus. This is done under sedation or general anesthesia.
- Natural miscarriage: If it’s safe, you may be able to watch and wait to see if your body eventually releases the pregnancy tissues. It can sometimes take days or weeks for this to start. Your healthcare provider will let you know if this is an option for you. You will experience cramping, abdominal pain and bleeding once the miscarriage begins.
- Medication-induced miscarriage: You may be given a medication called misoprostol to trigger your body to miscarry. This moves the process along and eliminates the time waiting for a miscarriage to start on its own. You will have cramping, abdominal pain and bleeding within 30 minutes to ten hours of taking the medication.
 This moves the process along and eliminates the time waiting for a miscarriage to start on its own. You will have cramping, abdominal pain and bleeding within 30 minutes to ten hours of taking the medication.
This moves the process along and eliminates the time waiting for a miscarriage to start on its own. You will have cramping, abdominal pain and bleeding within 30 minutes to ten hours of taking the medication.A follow-up appointment is usually scheduled four to six weeks after a miscarriage or D&C. You may be given another ultrasound to confirm the uterus is empty. Your healthcare provider will check for signs of infection and make sure there were no complications.
What are the complications of a blighted ovum?
Complications of a blighted ovum are uncommon, but the possible complications could include:
- Excessive bleeding or hemorrhage.
- Infection.
- Scarring (from the D&C procedure).
- Tears in the uterus (from the D&C procedure).
How long does it take to recover from a blighted ovum?
Recovering from a blighted ovum miscarriage or D&C can last from one or two weeks to a month. Cramping generally lasts up to a week, but bleeding can last several weeks. Your bleeding should get lighter until it stops completely.
Your bleeding should get lighter until it stops completely.
You can resume normal activities when you feel comfortable. Bleeding can increase with strenuous activity or exercise. Hormones may remain in your body and delay your menstrual cycle. Most people will get their period within four to six weeks after a blighted ovum.
It may take longer to recover emotionally from a blighted ovum miscarriage. You may have feelings of sadness, anger or confusion. It’s OK to take time to grieve. Ask your friends and family for support.
Prevention
Can a blighted ovum be prevented?
A blighted ovum can’t be prevented. Some couples may want to do genetic testing on the tissue inside the uterus. This checks for underlying causes of your miscarriage and can be helpful to couples who have experienced multiple pregnancy losses.
Outlook / Prognosis
How soon after a blighted ovum can I get pregnant again?
Most healthcare providers recommend having one or two regular menstrual cycles before trying to conceive again after any type of miscarriage.
What are my chances of having another blighted ovum?
Your chances of having another blighted ovum are low. Most people go on to have healthy, full-term pregnancies. If you experience more than one blighted ovum, your healthcare provider may suggest testing to determine if there is an underlying cause.
Living With
When should I see my healthcare provider?
Call your healthcare provider right away if you have any of these symptoms:
- Excessive bleeding from your vagina.
- Dizziness or fainting.
- Fever that does not go away.
- Symptoms that get worse over time.
- Severe pain that isn’t helped with pain medicine.
When should I go to the ER?
Go to the nearest ER If you experience heavy vaginal bleeding — more than two pads per hour for two consecutive hours — or have symptoms of anemia like dizziness, palpitations or paleness.
What questions should I ask my doctor?
Losing a pregnancy is upsetting and confusing. Do not be embarrassed to ask any questions you have. It’s completely normal to have questions and feel emotional during this time. Some questions you may ask are:
Do not be embarrassed to ask any questions you have. It’s completely normal to have questions and feel emotional during this time. Some questions you may ask are:
- Can I let my body miscarry or should I take medication to induce a miscarriage?
- What are the risks of miscarriage?
- Do I have to have a D&C?
- What are the risks of a D&C?
- How long can I expect to bleed or have cramping?
- Is there any indication this will happen again?
- When can I start trying to conceive?
- Do I need to come back for another ultrasound?
Frequently Asked Questions
Is a blighted ovum considered a miscarriage?
Yes, a blighted ovum is a miscarriage. A miscarriage is a loss of pregnancy before 20 weeks. A blighted ovum is considered an early miscarriage because it occurs before 13 weeks of pregnancy.
How long can you carry a blighted ovum?
The amount of time you can carry a blighted ovum varies. Your placenta will continue to grow and release hormones without an embryo. For some people, a miscarriage can occur within a few days or weeks. Others may still believe they are pregnant only to discover a blighted ovum at their first ultrasound.
Your placenta will continue to grow and release hormones without an embryo. For some people, a miscarriage can occur within a few days or weeks. Others may still believe they are pregnant only to discover a blighted ovum at their first ultrasound.
Can a blighted ovum turn into a baby?
No, an empty gestational sac will not turn into an embryo. The formation of the embryo occurs within two weeks of conception. By the time the gestational sac is formed, the cells should have already formed the embryo. Your healthcare provider will be able to examine your gestational sac to confirm that no embryo has developed.
Do hCG levels rise with blighted ovum?
Yes, most of the time hCG levels will rise, giving you a positive pregnancy test and symptoms of pregnancy. This is because the placenta continues to give off hCG even if an embryo is not present. The hormone hCG is sometimes called the pregnancy hormone because it is only produced if you are pregnant.
Is a blighted ovum more common with IVF?
A blighted ovum is not more common with IVF (In Vitro Fertilization). Your chances of having a blighted ovum with IVF treatment are about the same as they would be with a natural conception.
Your chances of having a blighted ovum with IVF treatment are about the same as they would be with a natural conception.
A note from Cleveland Clinic
Losing a pregnancy is difficult. If you are struggling after a miscarriage, speak with your healthcare provider so they can recommend support groups or counselors. Finding support may help you get through this hard time. Most people who have had a blighted ovum will go on to have a healthy pregnancy.
Not a Miscarriage | PSNet
The Case
A 32-year-old woman, gravida 3, para 1, with a history of Type 2 diabetes mellitus on metformin, presented at 7 and 2/7 weeks by last menstrual period (LMP). The patient reported a history of a primary low transverse cesarean section and a bicornuate uterus. Formal ultrasound revealed an intrauterine gestational sac, with no embryo, and a bicornuate uterus. Beta hCG was 1009 mIU/ml. Hgb A1C was 9.4 g/dL. Her metformin was discontinued and insulin was started.
She was scheduled for a repeat scan approximately 48 hours later, when her hCG would be expected to be over 2000 mIU/ml. At that time, she was spotting, and instead presented to the gynecology clinic. She was seen by an intern who presented the case to an attending and mentioned that the patient had already been found to have an intrauterine pregnancy (IUP) on formal sonogram, but failed to mention her history of a bicornuate uterus. They performed a transvaginal ultrasound, found an empty uterus with a thin stripe, and diagnosed the patient as having a completed spontaneous abortion. At that time, they restarted her metformin.
Several weeks later, the patient went to the family planning clinic for follow-up on a Friday afternoon, at which time a urine pregnancy test was positive. An hCG was checked and found to be 40,000 mIU/ml. She was given a lab slip to return on Monday (before the results were back), as it was unclear whether the urine pregnancy test was positive from an ongoing pregnancy or if she was pregnant again. Her hCG increased, and she was again seen in the gynecology clinic that day, where an ultrasound confirmed a 13 and 3/7 week IUP in the right uterine horn. The patient was then admitted for insulin therapy.
Her hCG increased, and she was again seen in the gynecology clinic that day, where an ultrasound confirmed a 13 and 3/7 week IUP in the right uterine horn. The patient was then admitted for insulin therapy.
In the case at hand, several important systems failed and a patient with a continuing and desired pregnancy was counseled that she had undergone a spontaneous abortion. The failure to recognize a continuing pregnancy could have led to teratogenic exposure to the fetus. Fortunately, this patient was taking only one medication, metformin, which is pregnancy category B and is not known to be associated with specific adverse consequences. Delayed prenatal care could have resulted in a failure to screen this patient for conditions other than diabetes that might complicate pregnancy and to provide counseling on nutrition and dietary modifications in pregnancy. Before describing systems that could have prevented this error, I will first provide a brief background on Mullerian anomalies, early pregnancy ultrasound, and the evaluation of first-trimester bleeding.
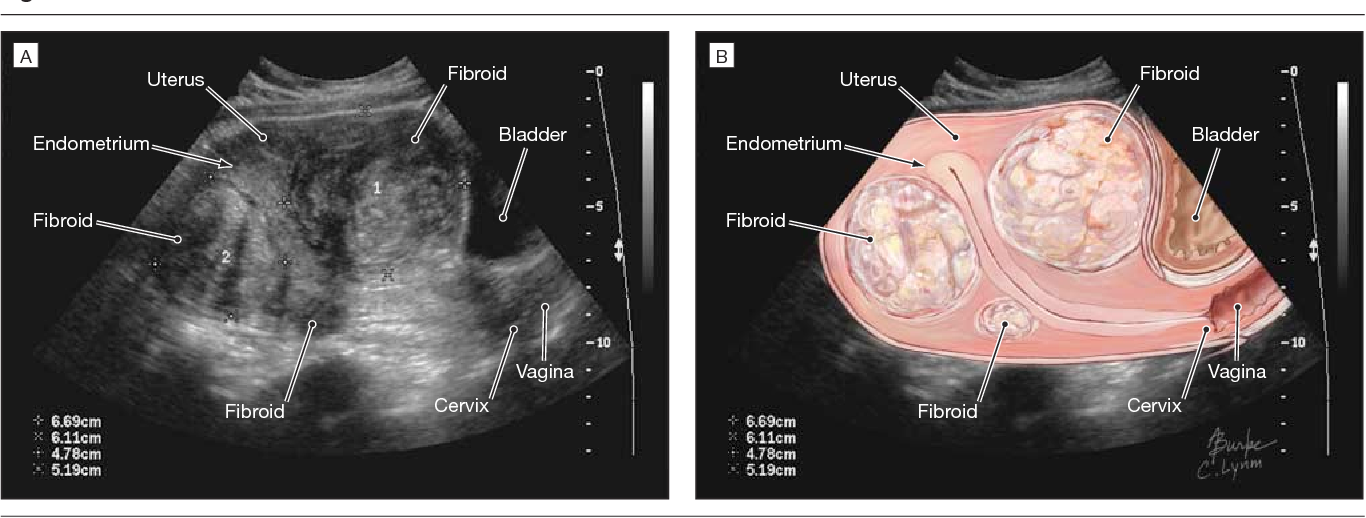
Mullerian Anomalies and Pregnancy The exact rate of Mullerian anomalies is unknown, as those achieving clinical detection are merely a subset of the most severe phenotypes. The most common is a bicornuate uterus (Figure 1), which is caused by incomplete fusion of the bilateral Mullerian systems during embryogenesis. Having a bicornuate uterus is associated with pregnancy complications including midtrimester pregnancy loss, preterm birth, and malpresentation.(1)
The Role of Ultrasound in Early Pregnancy Ultrasound is commonly used in the first trimester to assess gestational age. In many circumstances, it provides more accurate dating information than the last menstrual period.(2) In symptomatic or at risk patients, ultrasound can help distinguish spontaneous abortion from ectopic pregnancy. When no intrauterine pregnancy is visualized and no embryo is seen outside of the uterus, a single or serial measurement of the beta subunit of human chorionic gonadotropin (hCG) may be combined with ultrasound to diagnose an abnormal pregnancy of undetermined location, followed by uterine aspiration to make a definitive diagnosis. (3)
(3)
In this case, an intrauterine gestational sac was demonstrated on the first ultrasound performed (Figure 2). Therefore, no hCG surveillance was indicated to evaluate the possibility of ectopic pregnancy. Nevertheless, some physicians consider hCG patterns to be valuable in distinguishing normal from abnormal intrauterine pregnancies. Plateauing or declining patterns may prompt early intervention (uterine aspiration) in symptomatic patients.
Classifying Pregnancies with First-Trimester Bleeding Two classification systems permit us to reliably categorize patients with first-trimester bleeding. The clinical system relies on the pattern of bleeding and pain, uterine size, whether the cervix is open or closed, and (if open) whether tissue is present or not. Putting these data together permits a diagnosis of threatened, inevitable, incomplete, completed, or missed spontaneous abortion. Sonographic classification relies on the sequential appearance of the gestational sac, yolk sac, embryo, and cardiac activity. When thresholds in the normal sequence are breached, a diagnosis of anembryonic pregnancy or early embryonic demise can be made, irrespective of the patient’s symptoms. These two classifications systems are often used together when assessing patients with first trimester bleeding or pain.(4)
When thresholds in the normal sequence are breached, a diagnosis of anembryonic pregnancy or early embryonic demise can be made, irrespective of the patient’s symptoms. These two classifications systems are often used together when assessing patients with first trimester bleeding or pain.(4)
Strategies for Minimizing Diagnostic Errors Several important systems interventions could have prevented the failure to diagnose a continuing pregnancy in this patient.
Optimizing communication of important clinical information. Until patients are equipped with an electronic summary of their lifetime clinical record stored on portable media, health care providers and institutions will need to be vigilant in their communication, especially when records from one visit are not available at the follow-up visit. Diagnosing and treating ectopic pregnancy prior to catastrophic tubal rupture is so important that many obstetricians keep meticulous information on each patient with first trimester bleeding unless and until an intrauterine pregnancy is visualized on ultrasound or passed at the time of miscarriage.
In this patient, an intrauterine pregnancy was visualized at the initial ultrasound assessment. The patient was not followed with the same vigilance as she would have been if a potentially life-threatening ectopic pregnancy was still a possibility. When the patient presented with spotting, a repeat ultrasound examination was performed in the gynecology clinic. The gynecologist had received an incomplete report on the first ultrasound’s findings from a resident caring for the patient because the official report was not yet available. The resident and the patient did not mention her history of a bicornuate uterus. Had there been an ultrasound report available, this history would have been readily apparent and the repeat ultrasound could have been directed to the uterine horn in which the gestational sac had been detected. In this case, failure of communication and proper sign out from one physician to the other increased the risk of an incomplete ultrasound evaluation.
Relying on systematic checklists when ultrasound studies are performed, regardless of the circumstances or operator. Radiologists, gynecologists, and other health care providers credentialed in ultrasound assessment may perform these procedures skillfully. Examiner experience is one predictor of diagnostic accuracy.(5) However, errors can be minimized by the routine use of checklists and meticulous documentation of findings, no matter how experienced the operator.(6) The American Institute of Ultrasound in Medicine and the American College of Obstetricians and Gynecologists provide standards and guidelines for obstetrical ultrasound reports. Unfortunately, radiologists and obstetrician/ gynecologists demonstrate similarly low adherence rates to these guidelines in some settings.(7)
Radiologists, gynecologists, and other health care providers credentialed in ultrasound assessment may perform these procedures skillfully. Examiner experience is one predictor of diagnostic accuracy.(5) However, errors can be minimized by the routine use of checklists and meticulous documentation of findings, no matter how experienced the operator.(6) The American Institute of Ultrasound in Medicine and the American College of Obstetricians and Gynecologists provide standards and guidelines for obstetrical ultrasound reports. Unfortunately, radiologists and obstetrician/ gynecologists demonstrate similarly low adherence rates to these guidelines in some settings.(7)
The repeat ultrasound on this patient was a limited study assessing the progress of the intrauterine pregnancy noted previously. It appears unlikely that a procedural checklist was used. Such checklists may be developed even for studies of limited focus and purpose, to ensure that they are systematically performed. An “empty uterus” was seen. A complete assessment, including the adnexa, would have substantially reduced the risk of not finding the pregnancy in the other uterine horn.
An “empty uterus” was seen. A complete assessment, including the adnexa, would have substantially reduced the risk of not finding the pregnancy in the other uterine horn.
While it is true that this error would probably have been averted if the patient had reminded the team of her bicornuate uterus, several important safety nets also failed. The failure to diagnose a continuing pregnancy in this patient could have been prevented by ensuring complete communication of the relevant history (lifetime clinical record, physician-to-physician sign-out), the timely availability of new clinical information (ultrasound report), and the routine use of systematic procedural checklists for first-trimester ultrasound.
Lee A. Learman, MD, PhD Associate Professor and Residency Program Director UCSF Department of Obstetrics, Gynecology & Reproductive Sciences Director, General Competencies, UCSF Office of Graduate Medical Education
References
1. Ludmir J, Samuels P, Brooks S, Mennuti MT. Pregnancy outcome of patients with uncorrected uterine anomalies managed in a high-risk obstetric setting. Obstet Gynecol. 1990;75:906-910.[ go to PubMed ]
Pregnancy outcome of patients with uncorrected uterine anomalies managed in a high-risk obstetric setting. Obstet Gynecol. 1990;75:906-910.[ go to PubMed ]
2. Savitz DA, Terry JW Jr, Dole N, Thorp JM Jr, Siega-Riz AM, Herring AH. Comparison of pregnancy dating by last menstrual period, ultrasound scanning, and their combination. Am J Obstet Gynecol. 2002;187:1660-6.[ go to PubMed ]
3. Barnhart KT, Katz I, Hummel A, Gracia CR. Presumed diagnosis of ectopic pregnancy. Obstet Gynecol. 2002;100:505-10.[ go to PubMed ]
4. Luise C, Jermy K, May C, Costello G, Collins WP, Bourne TH. Outcome of expectant management of spontaneous first trimester miscarriage: observational study. BMJ. 2002;324:873-5.[ go to PubMed ]
5. Wojak JC, Clayton MJ, Nolan TE. Outcomes of ultrasound diagnosis of ectopic pregnancy. Dependence on observer experience. Invest Radiol. 1995;30:115-7.[ go to PubMed ]
6. Auerbach AD, Murff HJ, Islam SD. Pre-anesthesia checklists to improve patient safety.![]() In: Shojania KG, Duncan BW, McDonald KM, Wachter RM, eds. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43, AHRQ Publication No. 01-E058; July 2001. [ full report available ]
In: Shojania KG, Duncan BW, McDonald KM, Wachter RM, eds. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43, AHRQ Publication No. 01-E058; July 2001. [ full report available ]
7. Smulian JC, Vintzileos AM, Rodis JF, Campbell WA. Community-based obstetrical ultrasound reports: documentation of compliance with suggested minimum standards. J Clin Ultrasound. 1996;24:123-7.[ go to PubMed ]
Figures
Figure 1. Bicornuate Uterus (cross section). The normal uterus has a single cavity without horns. (Inset. Bicornuate uterus.) (Illustration by Chris Gralapp)
Figure 2. Transvaginal view of uterus. Gravid bicornuate uterus, pregnancy in right horn (RH).
Blighted ovum | Pregnancy Birth and Baby
Blighted ovum | Pregnancy Birth and Baby
beginning of content
4-minute read
Listen
Key facts
- A blighted ovum is a type of miscarriage that can happen early in a pregnancy.
- A blighted ovum is when a sac and placenta grow, but a baby does not.
- A miscarriage can be extremely upsetting, and you may need support and time to grieve.
- Having a blighted ovum in one pregnancy does not change your chance of having a successful pregnancy in the future.

What is a blighted ovum?
A blighted ovum is a type of miscarriage that can happen early in a pregnancy. It is also called an ‘anembryonic pregnancy’ as there is no embryo (developing baby). In this type of miscarriage, a sac and placenta grow, but there is no baby. Because a blighted ovum still makes pregnancy hormones, it may still show up as a positive pregnancy test.
A blighted ovum will eventually cause a miscarriage, usually at 7 to 12 weeks of pregnancy. Your body realises that the pregnancy is not developing properly and starts to shed blood and tissue from the uterus. You may notice pain in your lower abdomen, or bleeding from your vagina.
How common is miscarriage?
Miscarriage is very common, and up to 1 in 5 people who know that they are pregnant will miscarry before 20 weeks of gestation. The actual rate of miscarriage is even higher, as a very early miscarriage may happen before you even realise that you’re pregnant.
What causes a blighted ovum?
When the egg is fertilised, cells that make the pregnancy sac and placenta start multiplying. But occasionally, the cells that are supposed to develop into a baby don’t multiply.
The cause isn’t known. It isn’t caused by anything you have done.
How and when is blighted ovum diagnosed?
Sometimes, it is picked up during a routine ultrasound. This can be particularly difficult if you’ve gone for an ultrasound expecting good news.
At other times, there may have been bleeding at the start of the pregnancy and an ultrasound is used to investigate the cause.
How is blighted ovum treated?
Your doctor will discuss the options with you.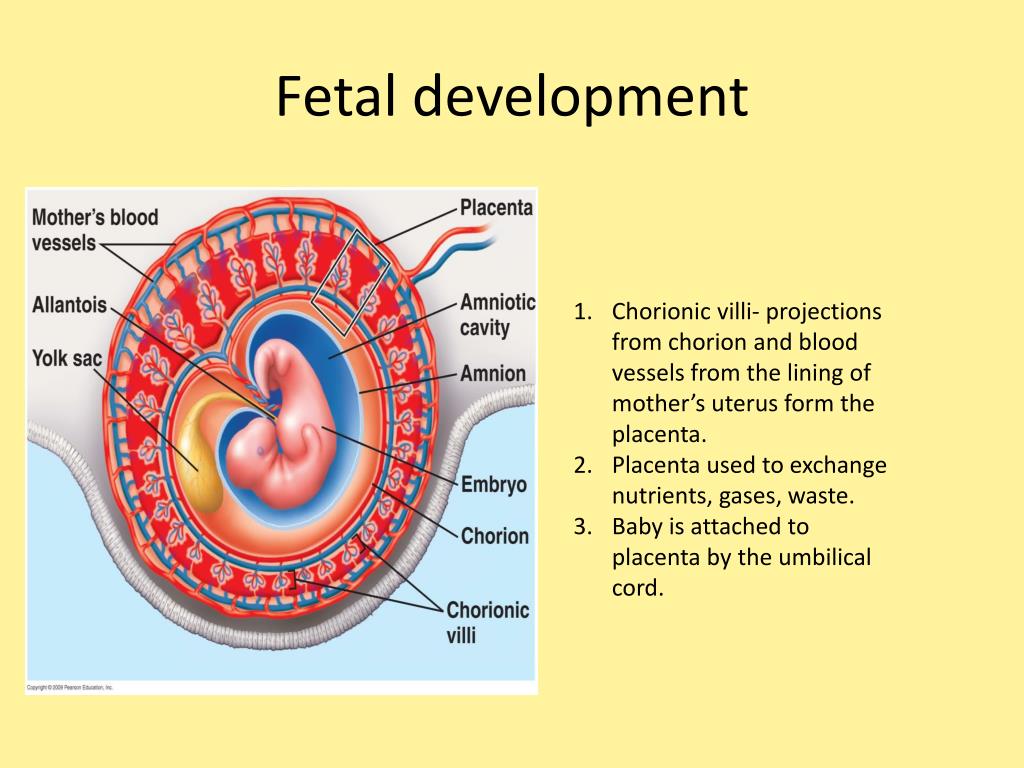 You might choose to allow a natural miscarriage to happen. Once this starts, it can take days or weeks for the bleeding to finish. If the bleeding is getting heavier, if you are in pain or you feel unwell, see your doctor.
You might choose to allow a natural miscarriage to happen. Once this starts, it can take days or weeks for the bleeding to finish. If the bleeding is getting heavier, if you are in pain or you feel unwell, see your doctor.
You could also have a termination by taking medicines or by having a type of surgery known as D & C.
Does it affect my chances of having a baby?
No. Having a blighted ovum in one pregnancy does not alter your chance of having a successful pregnancy in the future.
If you have had one miscarriage, your next pregnancy is likely to be normal. If you have had 3 miscarriages in a row, you should see your doctor to rule out any problems.
Where can I go for support and information?
Speak with your doctor if you are concerned that you may have a blighted ovum.
A miscarriage can be extremely upsetting. If you’ve experienced a miscarriage you may need support and time to grieve. There is no right way to feel after a miscarriage. Different people react to a miscarriage with different emotions, including anger, guilt or relief.
Different people react to a miscarriage with different emotions, including anger, guilt or relief.
Pregnancy, Birth and Baby helpline can offer emotional support and trusted advice to anyone who is dealing with pregnancy loss. Call Pregnancy, Birth and Baby on 1800 882 436 anytime of the day or night.
Sources:
Raising Children
(Miscarriage : what it is and how to cope),
Pink Elephants Network
(What is miscarriage?),
Red Nose
(Reasons for miscarriage)
Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: June 2022
Back To Top
Related pages
- Fathers and miscarriage
- Emotional support after miscarriage
- Miscarriage
- Pregnancy loss
Need more information?
Reasons for Miscarriage | Red Nose Australia
Read more on Red Nose website
Experiencing a pregnancy loss
Losing a baby at any stage of pregnancy can be devastating. Remember, pregnancy loss is more common than you probably think – and it’s not your fault. This article aims to help you deal with the many emotions you will be feeling.
Read more on Pregnancy, Birth & Baby website
Miscarriage
A miscarriage is the loss of a baby, usually during the first three months or first trimester of pregnancy.
Read more on Pregnancy, Birth & Baby website
Pregnancy: miscarriage & stillbirth | Raising Children Network
Have you experienced a miscarriage or stillbirth? Find articles and videos about coping with the grief of losing a pregnancy or having a stillbirth.
Read more on raisingchildren.net.au website
Miscarriage: a guide for men | Raising Children Network
This Dads Guide to Pregnancy covers miscarriage, the grief men might experience after miscarriage, and how to support partners after pregnancy loss.
Read more on raisingchildren.net.au website
The Pink Elephants Support Network – Supporting Your Physical Wellbeing After Miscarriage
Physical Wellbeing can be an important factor when trying to conceive
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network – Supporting Your Emotional Wellbeing After Miscarriage
It can be challenging to maintain a positive outlook after early pregnancy loss
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network – What is Miscarriage?
The vast majority of miscarriages will happen in the first 12 weeks of pregnancy, with some even happening before you knew you would have known you were pregnant
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network – Holistic Options for Miscarriage Management
Some women may find holistic options can help them feel nurtured and empowered on their journey to future pregnancy
Read more on Pink Elephants Support Network website
The Pink Elephants Support Network – Causes of Miscarriage – Pink Elephants
There are a number of possible reasons that a miscarriage may occur, and often it’s not until extensive testing is done that you may find out why
Read more on Pink Elephants Support Network website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now
entering.
OK
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google
Privacy Policy and
Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Anembryony – pregnancy or not?
Unfortunately, not all pregnancies end in childbearing. Reproductive losses in this case can be due to various reasons. And one of them is a non-developing or missed pregnancy. The proportion of this pathology accounts for up to 15-20% of reproductive losses. Currently, there are 2 variants of missed pregnancy: death of the embryo and anembryony. It is important to understand that the differential diagnosis between them does not affect the subsequent treatment tactics, but is taken into account when assessing the prognosis. Anembryony is more often determined, and this condition in many cases is not accompanied by spontaneous abortion and therefore requires artificial termination of a missed pregnancy.
Anembryony – what is it?
Anembryony – is the absence of an embryo in a developing fetal egg. This condition is also called the empty gestational sac syndrome. This is by no means a rare pathology that can be diagnosed in primigravida and in women who already have healthy children.
Many possible causes of anembryony have now been identified. These include:
- Genetic anomalies , which are observed in almost 80% of the pathological condition. They are usually associated with gross and/or multiple chromosomal abnormalities. Moreover, with anembryony, such anomalies are of a qualitative nature, and with the death of the embryo and its abortion, they are predominantly quantitative. Unviable combinations of parental genes or mutations in key areas responsible for the early stages of embryogenesis and the synthesis of the main structural proteins of cell membranes are also possible.
- Some acute viral and bacterial diseases occurring in early pregnancy and leading to damage to embryonic tissues or trophoblast. The most dangerous in this regard are TORCH infections, although other pathogens can also be embryotropic.
- Persistent viral-bacterial infections of the organs of the reproductive system, leading to the development of chronic endometritis . And in most cases, such a pathology occurs without obvious clinical symptoms and is detected after a frozen pregnancy.
- Radiation exposure of to a developing embryo.
- Exogenous intoxications : taking drugs with embryotoxic action, drug addiction, exposure to certain industrial and agricultural poisons (toxins).
- Endocrine disorders in a pregnant woman. And the most critical is the deficiency of progesterone and disorders of its metabolism, which is the main cause of the pathology of endometrial decidualization and abnormal implantation of the fetal egg.
 The most dangerous in this regard are TORCH infections, although other pathogens can also be embryotropic.
The most dangerous in this regard are TORCH infections, although other pathogens can also be embryotropic. In general, the causes of pathology in most cases remain undiagnosed. Usually it is possible to determine only a presumptive etiology.
Usually it is possible to determine only a presumptive etiology.
Genetic diagnosis of aborted tissues can reveal obvious anomalies of hereditary material. But such a study, unfortunately, is carried out in a very small percentage of cases. Basically, it is indicated with a burdened obstetric history in a woman, when she already had frozen or spontaneously interrupted in the early stages of gestation in the past. But even such a diagnosis is not always informative enough, which is associated with the limited possibilities of modern genetics and the high probability of the impact of other etiological factors.
Pathogenesis
Anembryony is a consequence of the cessation of reproduction and differentiation of the embryoblast or inner cell mass – a group of cells that normally give rise to fetal tissues. And this happens at the earliest stages of pregnancy (usually at 2-4 weeks of gestation), and without disturbing the development of the fetal membranes from the trophoblast. As a result, a so-called empty fetal egg is formed, which continues to grow even in the absence of an embryo in it.
As a result, a so-called empty fetal egg is formed, which continues to grow even in the absence of an embryo in it.
Pathogenetically important factors in the development of the disease include:
- Inherited or acquired chromosome aberrations and other genetic abnormalities. They can lead to a gross desynchronization of the development of embryonic tissues, critical changes in the structure of collagen and other proteins, disruption of the induction of differentiation and migration of dividing cells. The most common autosomal trisomy, monosomy, triploidy, tetraploidy.
- Excessive formation of circulating immune complexes in a woman’s body . Their deposition in the walls of small vessels leads to thromboembolism and other critical microcirculation disorders in the area of the implanting egg. Antiphospholipid antibodies are of the greatest clinical importance.
- Excessive activation of T-helpers with an increase in the concentration and aggression of the cytokines secreted by them. These substances are able to have a direct and indirect damaging effect on embryonic tissues with a violation of their proliferation and differentiation. In fact, the fetal egg in this case acts as a target for the cellular link of immunity. The reason for such an abnormal immune response of a woman’s body may be a chronic infection of the endometrium, hormonal abnormalities, and some other endogenous factors.
 These substances are able to have a direct and indirect damaging effect on embryonic tissues with a violation of their proliferation and differentiation. In fact, the fetal egg in this case acts as a target for the cellular link of immunity. The reason for such an abnormal immune response of a woman’s body may be a chronic infection of the endometrium, hormonal abnormalities, and some other endogenous factors.
These substances are able to have a direct and indirect damaging effect on embryonic tissues with a violation of their proliferation and differentiation. In fact, the fetal egg in this case acts as a target for the cellular link of immunity. The reason for such an abnormal immune response of a woman’s body may be a chronic infection of the endometrium, hormonal abnormalities, and some other endogenous factors. It is important to understand that with anembryony in the body of a woman, substances are produced that contribute to the prolongation of pregnancy. Therefore, in a significant proportion of cases, spontaneous abortion does not occur. The patient develops and maintains signs of pregnancy, there is an increase in hCG in the blood serum. Therefore, the basal temperature during anembryony usually does not have characteristic features. And on the first early ultrasound, the fact of successful implantation of the fetal egg in the uterine cavity is confirmed. After all, pregnancy does occur, but it develops without a key component – the embryo.
In the future, rejection of the abnormal fetal egg is possible. In this case, the threat of termination of pregnancy (including with the formation of exfoliating retrochorial hematomas) or spontaneous abortion (miscarriage) can be diagnosed. But often anembryony is diagnosed only during a routine examination, in which case the diagnosis is absolutely unexpected and shocking news. Such a pregnancy requires an artificial interruption.
How does this manifest itself?
Anembryony does not have its own clinical symptoms , all emerging disorders are usually associated with the threat of termination of such a pathological pregnancy. And the warning signs include the presence of clinical manifestations of relative progesterone deficiency, which creates the prerequisites for spontaneous abortion. Therefore, pain in the lower abdomen and bloody discharge can become a reason for contacting a doctor; with anembryony, they can appear at almost any time during the 1st trimester. But often a woman learns about the existing pathology only when conducting a screening ultrasound for a period of 10-14 weeks.
But often a woman learns about the existing pathology only when conducting a screening ultrasound for a period of 10-14 weeks.
Diagnosis
Like other forms of miscarriage, anembryony is detected in the first trimester of gestation. And the main diagnostic tool in this case is ultrasound , because it is this study that allows you to visualize the existing deviations.
At the same time, symptoms can be reliably detected only after the 8th week of gestation. At earlier dates, visualization is often insufficient due to the too small size of the ovum, so an erroneous diagnosis is not ruled out. Therefore If a missed pregnancy and anembryony are suspected, it is recommended to conduct an examination several times, repeating the procedure on expert-class equipment with an interval of 6-8 days. At the same time, the initial diagnosis of an empty fetal egg can be removed if subsequent ultrasound scans can visualize an embryo with signs of a heartbeat and sufficient developmental dynamics.
The main echographic features:
- absence of the yolk sac when the diameter of the fetal egg is 8-25 mm;
- absence of an embryo in a fetal egg with a diameter of more than 25 mm.
Additional signs of a missed pregnancy include an irregular shape of the fetal egg, an insufficient increase in its diameter in dynamics, a weak severity of the decidual reaction, and the absence of a heartbeat at a gestational age of 7 or more weeks. And signs of the threat of its interruption are a change in the tone of the uterus and the appearance of areas of chorion detachment with the appearance of subchorial hematomas.
Anembryony can also be suspected by a dynamic assessment of the level of hCG in the blood. An increase in the level of this hormone along the lower limit of the norm should be the basis for further examination of a woman with an ultrasound scan. It is important to understand that hCG is also produced in the syndrome of an empty ovum. Moreover, its level in this pathology will be almost normal, in contrast to a frozen pregnancy with the death of a normally developing embryo. Therefore, monitoring of indirect signs of pregnancy and the growth of hCG during anembryony cannot be attributed to reliable diagnostic methods.
Moreover, its level in this pathology will be almost normal, in contrast to a frozen pregnancy with the death of a normally developing embryo. Therefore, monitoring of indirect signs of pregnancy and the growth of hCG during anembryony cannot be attributed to reliable diagnostic methods.
Varieties
Several variants of the empty ovum syndrome are possible:
- Type I anembryony. The embryo and its remains are not visualized, the size of the fetal egg and uterus does not correspond to the expected gestational age. The diameter of the egg is usually no more than 2.5 mm, and the uterus is enlarged only up to 5-7 weeks of gestation.
- Type II anembryony. There is no embryo, but the fetal egg and uterus correspond to the gestational age.
- Resorption of one or more embryos in multiple pregnancies. At the same time, normally developing and regressing fetal eggs are visualized. According to this type, anembryony often occurs after IVF, if several embryos were implanted in a woman.
 According to this type, anembryony often occurs after IVF, if several embryos were implanted in a woman.
According to this type, anembryony often occurs after IVF, if several embryos were implanted in a woman. All these varieties are determined only with the help of ultrasound, they do not have characteristic clinical features .
What to do?
Confirmed anembryony is an indication for abortion. This does not take into account the gestational age, the woman’s well-being and the presence of signs of a possible spontaneous abortion. An exception is the situation when the anembryony of the second fetal egg is diagnosed in a multiple pregnancy. In this case, a wait-and-see strategy is taken, evaluating the dynamics of the development of the preserved embryo.
Termination of a missed pregnancy is carried out only in a hospital. After the procedure for the evacuation of the fetal egg, the woman should be under medical supervision. In many cases, after it, additional medication and sometimes physiotherapy are prescribed, aimed at normalizing the hormonal background, preventing inflammatory and hemorrhagic complications, and eliminating the detected infection.
Several techniques can be used to perform a medical abortion for this pathology. Can be used:
- medical abortion – termination of pregnancy with the help of hormonal drugs that provoke rejection of the endometrium along with an implanted fetal egg;
- vacuum aspiration of the contents of the uterine cavity;
- curettage is an operation involving the mechanical removal of the fetal egg and endometrium with a special instrument (curette) after the forced expansion of the cervical canal with bougie.
Medical abortion for anembryos is possible only for a period of 6-8 weeks. In later periods of gestation, preference is given to mechanical methods, which requires the use of general anesthesia. The choice of the method of artificial abortion depends on whether the stomach hurts after an abortion, the length of the rehabilitation period, the likelihood of early and late complications.
Examination after induced abortion necessarily includes ultrasound control. This allows you to confirm the complete evacuation of the membranes and endometrium, to exclude undesirable consequences of abortion in the form of hematomas, perforation and endometritis.
This allows you to confirm the complete evacuation of the membranes and endometrium, to exclude undesirable consequences of abortion in the form of hematomas, perforation and endometritis.
Prediction
Can anembryony recur? Can I still have children? These questions concern all patients who have undergone this pathology. Fortunately, in most cases, the condition does not recur, the woman subsequently manages to safely become pregnant and bear the child. But at the same time, she is classified as a risk group for the possible development of complications of pregnancy and childbirth. Therefore, in the first trimester, she is usually assigned dynamic ultrasound control of the development of the fetal egg, determination of the hormonal profile and assessment of the state of the hemostasis system.
Pregnancy after anembryos is theoretically possible already in the next ovarian-menstrual cycle. But it is desirable to let the body recover. Therefore, it is recommended to start planning for re-conception not earlier than 3 months after the induced abortion . If it proceeded with complications, the rehabilitation period, while maintaining reproductive rest, is extended for up to six months. If a woman has chronic endometritis and various infections, 2 months after the completion of treatment, a control examination is carried out and only then the possible timing of re-conception is determined.
Therefore, it is recommended to start planning for re-conception not earlier than 3 months after the induced abortion . If it proceeded with complications, the rehabilitation period, while maintaining reproductive rest, is extended for up to six months. If a woman has chronic endometritis and various infections, 2 months after the completion of treatment, a control examination is carried out and only then the possible timing of re-conception is determined.
Barrier method and hormonal contraception are preferred to prevent pregnancy. The selection of funds in this case is carried out individually. Intrauterine devices immediately after a frozen pregnancy are not used in order to avoid the development of endometritis.
Prevention
Primary prevention of anembryonia includes careful planning of pregnancy with a comprehensive examination. If deviations are found, they are corrected. Of course, such preparation does not allow 100% to exclude the possibility of pathology, but reduces the risk of its development.
Secondary prophylaxis is carried out if the woman has a history of spontaneous abortions and anembryos. The first pregnancy with empty ovum syndrome is a reason for a subsequent examination of a woman for infections and hemostasis disorders. When the situation repeats, a genetic examination of the spouses is also shown to exclude anomalies in their hereditary material. In some cases, subsequent conception is preferably carried out using IVF, which will allow the use of preimplantation diagnosis to detect chromosomal abnormalities in embryos.
Anembryony is diagnosed quite often. And, unfortunately, at the present time it is not yet possible to completely exclude such a pathology already at the stage of pregnancy planning. After all, it can develop even in completely healthy and examined patients. At the same time, a missed missed pregnancy does not mean the impossibility of a repeated successful conception; most women after anembryony manage to safely give birth to a healthy child.
modern diagnostic and treatment methods
A fertilized egg without an embryo is usually found on ultrasound and is a very common condition. According to some reports, the absence of an embryo is diagnosed in 2 out of 10 women who are faced with a missed pregnancy.
Since there is no fetus as such, symptoms typical of early pregnancy disappear – breast swelling, unstable mood, lethargy and nausea. What to do in this case, the gynecologist decides. The choice of treatment method depends on the duration of pregnancy and the state of health of the woman.
What is an “empty pregnancy”
If there is a fertilized egg, but there is no embryo, they speak of a non-vesical drift, which is also called anembryony. The embryo could not be in the uterus initially, or it died for up to 5 weeks. In about a quarter of women, such a pregnancy ends in a miscarriage or freezes.
Slightly more than half of the cases are due to spontaneous uterine cleansing: this should occur within 2 weeks after the detection of anembryony. Otherwise, fragments of the fetal egg must be removed medically or surgically.
Otherwise, fragments of the fetal egg must be removed medically or surgically.
An empty amniotic egg must be removed no later than 2 weeks after its discovery. If it remains in the uterus after this period, there is a high probability of complications and bleeding. For a more detailed consultation, please contact our doctors – they will give all the necessary recommendations by phone and answer all your questions.
Why the ovum is empty: reasons
It is rather difficult to establish the exact cause of anembryonia, it is determined taking into account the existing symptoms and the results of the examination of a pregnant woman. The culprits of this phenomenon can be various factors associated with the characteristics of the mother’s body.
The greatest risk of pregnancy fading occurs in the early stages, when the blastomeres are just beginning to divide, and the embryo is attached to the wall of the uterus.
There are several reasons why an embryo does not develop in a fetal egg:
- gene mutations that do not depend on the genes of the parents;
- endometrial diseases of an atrophic, inflammatory nature;
- defects in the structure of the reproductive organs of the mother;
- violation of blood clotting;
- too tight fixation of the embryo in the uterus;
- weak local immunity of the myometrium;
- a disorder of the contractile function of the uterus due to improper metabolism and chronic inflammatory processes in the uterine tissues;
- folate deficiency.
Gene mutations
This is the leading reason why the gestational sac is empty. Chromosomal abnormalities can appear at different stages:
- When an egg is fertilized by two sperm.
- During further cell division.
The risk of gene mutations increases with a woman’s age.

Endometrial diseases
The absence of an embryo in the fetal egg may be associated with chronic endometritis and the syndrome of regenerative plastic insufficiency of the endometrium. A chronic inflammatory process leads to changes in the work of local immunity, which reduces the susceptibility of mucous membranes.
In addition, with sluggish and prolonged inflammation, erythrocytes stick together in the developing chorionic villi, which ultimately leads to the formation of mini-thrombi.
Defects in the structure of the reproductive organs
We are talking about congenital or acquired structural features due to polyps, fibroids or synechiae. Such diseases are accompanied by hormonal imbalance and changes in the receptivity of the endometrium.
Bleeding disorder
The embryo may die in the early stages of gestation due to lack of nutrition during the formation of blood clots in the intervillous space, when thrombophilia develops for various reasons.
Embryo too tight
Excessively deep implantation of the embryo occurs in 2 cases: if it is actively growing, and the uterine myometrium is not sufficiently prepared for implantation of the embryo, or if the endometrium is functionally immature.
Weak local immunity
The reactivity of the myometrium is one of the possible reasons that the fetal egg turned out to be without an embryo. It persists in the uterus due to an insufficient immune response, which normally causes the embryo to be rejected as a foreign body.
Contractile function disorder
An empty fetal sac is not rejected in some chronic pathologies of the uterus, accompanied by a violation of the formation of receptors for substances that stimulate uterine contractions (uterotonic). Very often, the contractility of the uterus falls due to improper interstitial metabolism.
Folic acid deficiency
This acid is a direct participant in the process of division of cellular DNA. If it is not enough in the early stages of gestation, the chromosomes diverge and arrange themselves incorrectly.
If it is not enough in the early stages of gestation, the chromosomes diverge and arrange themselves incorrectly.
Pregnancy without embryo: species
A fetus without an embryo is of 2 types:
- On ultrasound, the embryo is not visible, the fetal sac measures a maximum of 2.5 cm, the volume of the uterus corresponds to 5-7 weeks, which is not consistent with the date of actual conception. Subsequent studies on an ultrasound machine do not record an increase in the uterus.
- The fetal egg is empty, its size and volume of the uterus correspond to the gestational age. However, the fertilized egg grows, but the embryo does not.
Empty ovum after IVF
Embryo resorption is possible after in vitro fertilization, in which several fetal eggs (PY) are implanted into the woman’s uterus. This increases the chances of successful conception.
As a rule, only one embryo takes root, although sometimes 2 or more embryos are implanted in the wall of the uterus. However, not all of them continue to develop, some of the fetal sacs are absorbed or excreted from the body naturally.
However, not all of them continue to develop, some of the fetal sacs are absorbed or excreted from the body naturally.
Signs of an empty gestational sac without an embryo
In the absence of a fetus, there is a regression of symptoms typical of early gestation – nausea, pain in the mammary glands, sleep problems, etc. The woman feels like before pregnancy and ceases to react sharply to smells, and also loses her recent craving for a certain unusual food.
Case study:
The woman had no doubt that she was pregnant, and experienced symptoms typical of her condition – nausea, engorgement of the mammary glands, and tightness of the abdomen. When the symptoms suddenly disappeared, she did not attach any importance to this. On a planned ultrasound, the doctor saw an empty fetal egg at 6 weeks and prescribed the necessary treatment.
However, the fact that there is no toxicosis and other symptoms does not unequivocally indicate an empty fetal egg or the absence of an embryo. Similar signs can be with a frozen pregnancy.
Similar signs can be with a frozen pregnancy.
But if the decay of the tissues of the embryo begins, then there are pronounced symptoms of intoxication:
- rise in temperature;
- nausea turning into vomiting;
- body aches;
- weakness;
- lower abdominal pain;
- bleeding of varying intensity.
The onset of embryo rejection can be suspected by the appearance of vaginal discharge mixed with blood.
Complications
If the uterus does not contract well, or there are problems with blood clotting, bleeding begins. By itself, it is not capable of stopping, the help of a doctor is needed. In addition, bleeding can cause infection of the uterine cavity and anemia.
In some cases, the fertilized egg decomposes asymptomatically, or the process causes mild discomfort. Empty amniotic membranes spontaneously separate from the endometrium and leave the body naturally.
But more often, an amniotic egg without an embryo remains in the uterus and provokes serious complications that often threaten health and even life. If left untreated, chronic endometritis can develop.
Anembryony is sometimes complicated by infertility and miscarriage in the future.
If the gestational sac continues to grow for 2 weeks or more, the inflammation symptoms described above occur. We advise you to contact our doctors, since the inflammatory process can spread to the entire uterus and nearby tissues. By phone, the doctor will give recommendations and instruct about further actions.
Fetal egg without embryo: diagnostics
An empty egg during pregnancy is detected by ultrasound. Ultrasound allows you to detect the presence of an embryo for a period of 6-7 weeks, before it is not visualized due to its small size and literally merges with neighboring structures.
Therefore, sonography is performed at 6-7 weeks and confirms (or refutes) the fact of conception. Up to this point, the presence of the embryo is determined by the level of hCG – human chorionic gonadropin.
Up to this point, the presence of the embryo is determined by the level of hCG – human chorionic gonadropin.
Case study:
The woman, suspecting pregnancy, passed the test for hCG. Its level was increased and amounted to 50 mU/ml. However, ultrasound revealed the absence of an embryo in the egg. A re-examination 2 weeks later confirmed the diagnosis of anembryony.
HCG is called the hormone of pregnancy, its production starts 6-7 days after the attachment of the chorion – the fetal membrane of the embryo – to the uterus. In normal pregnancy, the concentration of hCG increases with the growth of the fetus.
hCG with an empty fetal egg
If there is no embryo in the egg, then the level of hCG, as a rule, grows more slowly or becomes less. This indicator can serve as an indirect confirmation of an undeveloped pregnancy, along with an insufficient content of progesterone in the blood.
HCG values at the lower limit of the norm are the reason for the appointment of ultrasound, since gonadropin is synthesized even in the absence of an embryo. Moreover, its level is usually within the normal range, in contrast to a missed pregnancy with a dead fetus.
Moreover, its level is usually within the normal range, in contrast to a missed pregnancy with a dead fetus.
Attention! The hCG parameter cannot be considered a reliable diagnostic criterion for anembryony. Therefore, even if hCG is growing, but there is no fetal egg, it is too early to diagnose an empty pregnancy. After all, the growth of the placenta does not stop immediately.
Why does a fertilized egg grow, but there is no embryo in it
The formation of the body of the embryo and its outer membranes begins at the blastula stage. When it enters the uterine cavity, its outer cells produce specific enzymes that partially dissolve the endometrium and facilitate implantation.
After insertion into the wall of the uterus, the embryo, together with the amniotic membranes, develops synchronously with the gradual formation of the placenta and fetus.
With anembryony, a fetal egg grows, that is, only the outer shell that produces hCG. And the embryo either does not form at all, or its formation is completed at the initial stages. This is due to incorrect test data showing the development of pregnancy.
And the embryo either does not form at all, or its formation is completed at the initial stages. This is due to incorrect test data showing the development of pregnancy.
However, after some time, hCG still ceases to stand out and decreases.
What to do if there is no embryo in the ovum
If the fertilized egg does not grow due to the absence of an embryo, it is necessary to artificially terminate the pregnancy. Obstetricians and gynecologists do not recommend waiting until the situation resolves itself, and treat with one of three methods:
|
Term |
Methodology |
Peculiarities |
Flaws |
|
6-8 weeks |
medical abortion |
Taking medications – Mifepraston, Misoprazole |
After 8 weeks, incomplete rejection of the fetus is possible with the development of complications |
|
Up to 5 weeks |
Vacuum aspiration (mini-abortion) |
The fertilized egg is pulled out (aspirated) by means of a vacuum pump |
There is a risk of incomplete abortion, ultrasound control after the procedure is necessary |
|
6-12 weeks |
Curettage (curettage) |
The uterine cavity at the site of attachment of the fetal egg is mechanically scraped with an iron curette |
The likelihood of serious complications – bleeding, infections, ruptures, perforations of the cervix and uterus |
The most effective and safe is medical abortion with the use of drugs that provoke uterine contractions and inhibit endometrial progesterone receptors.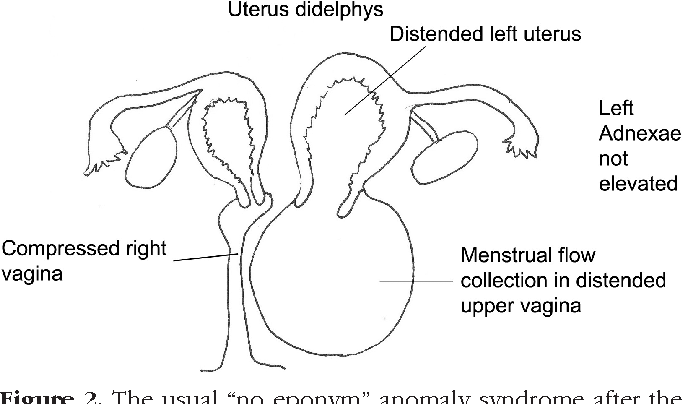
Medical expulsion of the fetus does not damage the mucous membranes of the uterus and does not carry any risks in the future.
Vacuum aspiration can be performed for up to 12 weeks, according to WHO recommendations. However, in Russia, most often it is done no later than 5 weeks.
Rehabilitation
A single case of anembryony does not raise questions and does not pose a danger. However, if it recurs, or the pregnancy is terminated in the early stages for another reason, it is necessary to establish why the embryo does not develop.
For this, a comprehensive examination and rehabilitation treatment is carried out. Basically, women are diagnosed with chronic endometritis, which can have vivid manifestations or be asymptomatic. Therefore, first of all, antibiotic therapy is prescribed.
In the treatment of endometrial diseases, drugs of several groups are also used:
- anti-inflammatory;
- immunostimulants;
- enzymes;
-
hormones.

Taking combined contraceptives is recommended for 3-6 months in order to restore hormonal levels.
Attention! A new conception should be planned only after a full preconception preparation.
FAQ
Can there be a 15 mm PJ?
+
Yes, it is usually seen at 6.5 weeks. The child develops the brain and nervous system. When the fetal egg reaches 15 mm, facial features, eye sockets, and nasolabial folds begin to form.
Can a fertilized egg grow without an embryo?
+
Yes, this is type 2 anembryony, which can last up to 11 weeks. The size of the egg can reach 5 cm.
What if the fertilized egg is smaller than the embryo? The size of the PY is 2 weeks behind!
+
This is normal, no need to worry. The situation will stabilize after a while, there is no danger to the fetus.
Expert opinion:
A fetal egg without an embryo can be in an absolutely healthy woman. But even in the absence of any pathologies, it is necessary to take a break and resume attempts to conceive a child no earlier than after 2-3 cycles.
Non-developing pregnancy – price in St. Petersburg
-
Services
-
In Vitro Fertilization (IVF)
-
Pregnancy management and prenatal diagnosis
-
Biopsy of the endometrium
-
Prostate treatment
-
Diabetes mellitus in pregnancy
-
Endocrine (hormonal) infertility in women
-
Oocyte donation
-
IVF for polycystic ovaries
-
Center for Complex Pathologies
-
Biopsy of the cervix
-
Treatment of cystitis in women and men
-
PRP therapy for the uterus and ovaries
-
Sperm donation
-
Embryo cryopreservation
-
Screening ultrasound in the first trimester
-
Pediatric gynecology
-
Treatment of urethritis
-
Fertilization of eggs and cultivation of embryos
-
Screening ultrasound in the second trimester
-
cervical dysplasia
-
Treatment of varicocele
-
Videocolposcopy
-
Pregnancy management programs
-
IVF according to compulsory medical insurance for residents of the regions
-
Expert ultrasound 3D/4D during pregnancy
-
Non-invasive prenatal genetic test
-
Preimplantation genetic testing
-
IVF under CHI for residents of St.
Petersburg
-
IVF according to compulsory medical insurance in the Leningrad region
-
Infertility treatment
-
ultrasonic cavitation
-
Transfer of embryos into the uterus
-
Screening ultrasound in the third trimester
-
Erosion of the cervix (ectopia)
-
Implatest – Endometrial Receptivity Study
-
Colposcopy
-
Endometrial polyp
-
Laparoscopy of an ovarian cyst
-
Fetal cardiotocography (fetal CTG)
-
Hysteroscopy
-
Office hysteroscopy
-
Office hysteroscopy diagnostic
-
Office hysteroscopy with endometrial biopsy
-
Laboratory diagnostics
-
Day hospital
-
Follicle puncture
-
Stimulation of superovulation
-
Treatment of preeclampsia
-
Ultrasound examination of folliculogenesis with biophysical profile of the uterus
-
Hysteroresectoscopy
-
Hysterosalpingography
-
Fallopian tube laparoscopy
-
Laparoscopy in gynecology
-
Laser vaporization of the cervix
-
Treatment of endometriosis
-
Treatment of an ovarian cyst
-
Laparoscopy of uterine fibroids
-
Non-developing pregnancy
-
Pathology of the endometrium
-
Pathology of the cervix
-
Treatment of an endometrial polyp
-
Polyp of the cervix
-
Preventive examination by a gynecologist
-
radio wave surgery
-
polycystic ovary syndrome
-
Ultrasound hysterosalpinography (USGSG)
-
human papillomavirus
-
Vulvovaginal candidiasis
-
Frozen pregnancy
-
-
Specialists
-
Service cost
-
Reviews
-
Stock
 Petersburg
Petersburg
Sign up
8 812 565-18-40
An expert approach to happiness!
Our branches
Auxiliary
reproductive technologies
Obstetrics
and gynecology
Medical center
fetuses
Urology
and andrology
Assisted Reproductive Technologies
obstetrics and gynecology
Center for Fetal Medicine
Urology and Andrology
St. Petersburg, Torez avenue, 72
Petersburg, Torez avenue, 72
Center for Reproduction and Family Planning Medica in St. PetersburgServicesNon-developing pregnancy
Is there a chance to become parents after a “frozen” pregnancy? And is there any way to prevent it? What can be done to prevent something like this from happening again?
Enroll
Non-developing pregnancy is the spontaneous death of the embryo in the womb, which most often occurs in the first trimester of pregnancy. There is a risk of fetal death in the second and third trimesters, but it is much lower.
It is the risk of stopping the development of the fetal egg that makes the first 12 weeks of pregnancy the most critical. As a rule, the woman herself does not immediately understand what happened. The first signs of the freezing of the fetal egg can appear only 2-3 weeks after the tragedy, when it begins to be torn away from the uterine mucosa. The fetal egg can leave the woman’s body on its own, but in some cases, part of the fetal membranes remains in the uterus.
The fetal egg can leave the woman’s body on its own, but in some cases, part of the fetal membranes remains in the uterus.
Read more
About direction
At the Center for Reproduction and Family Planning “MEDICA” future parents:
Independently (if desired) choose an obstetrician-gynecologist who will conduct the pregnancy;
Together with the doctor, they choose the optimal pregnancy management program;
They receive the most attentive, caring attitude and are always surrounded by warmth and care;
Do not stand in queues, but get an appointment with specialists at the appointed time;
They are constantly in contact with their obstetrician-gynecologist, they can always contact him personally and ask any questions;
Together with an obstetrician-gynecologist, they decide where to give birth and what tactics of childbirth to choose.
Cost of services
Full price list for referral services
Obstetrician-gynecologist, primary appointment
2 350 ₽
Enroll
Obstetrician-gynecologist, repeated appointment
2 100 ₽
Enroll
Obstetrician-gynecologist (highest category / candidate of medical sciences / doctor of medical sciences), initial appointment
2 900 ₽
Enroll
Obstetrician-gynecologist (highest category / candidate of medical sciences / doctor of medical sciences), repeated appointment
2 500 ₽
Enroll
show more
Video
Embryo biopsy
Oocyte vitrification and delayed motherhood program – childbirth (,) must not be (,) delayed 18+
Reproductologist Elena Tanchuk about indications for ART (assisted reproductive technologies)
Human papillomavirus (HPV) and cervical cancer – diagnosis, treatment, prevention. Samoilova Svetlana Gennadievna
Samoilova Svetlana Gennadievna
Treatment of infertility in different age periods. Yusupova Oksana Nikolaevna CPS Medica 18+
Hormonal contraceptives COCs – truth and myths. Kovaleva Natalia Sergeevna CPS Medica 18+
Hysterosalpingography (HSG) at the Center for Reproduction and Family Planning Medica
The female factor in infertility. Tanchuk Elena Valerievna. Reproduction Center Medica 18+
Frozen pregnancies – why pregnancy does not develop. Bokach Olga Mikhailovna
Sexually transmitted infections (STIs) – types, transmission, diagnosis. Sheikhov Magomedsadiq 18+
How to plan a healthy pregnancy. Yusupova Oksana Nikolaevna
Yusupova Oksana Nikolaevna
Cryopreservation of germ cells and embryos. Kozhevnikov Igor Valerievich
Treatment of infertility in different age periods. Yusupova Oksana Nikolaevna CPS Medica 18+
The menstrual cycle – the norm and pathology. Danielyan Roza Martunovna. CPS Medica. 18+
Male fertility – when should a man start to worry and anti-age therapy CPS Medica 18+
Reproduction doctor’s appointment – we plan pregnancy correctly. Pisaroglo Maria Ivanovna. CPS Medica
Psychosomatics of infertility – all diseases are caused by nerves. Konon Ksenia Mikhailovna. CPS Medica 18+
Reproductologist Elena Tanchuk about indications for assisted reproductive technologies (ART)
PCOS (polycystic ovary syndrome). Danielyan Roza Martunovna. Reproduction Center Medica 18+
Danielyan Roza Martunovna. Reproduction Center Medica 18+
Testosterone and its effect on the human body. Kudryavtsev Artemy Alexandrovich. CPS Medica 18+
Ultrasound screening of pregnant women – why and how often. Ten Natalya Alekseevna. CPS Medica
Successful embryo implantation during natural pregnancy and after IVF. Konon Xenia Mikhailovna.18+
Endometriosis. Zakharova Oksana Vadimovna Center for Reproduction and Family Planning Medica 18+
The episode of the broadcast of the hysteroscopy operation in the ‘Center for Reproduction and Family Planning ‘Medica’
Erectile dysfunction – diagnosis, treatment, prevention. Sheikhov Magomedsadyk Gasanovich. 18+
Sheikhov Magomedsadyk Gasanovich. 18+
Popular questions
All questions in the direction
Hello. Everything was great with my first pregnancy, a healthy girl was born, but 2 months. ago I had a frozen pregnancy, how to avoid all this in the future? I just can’t stand another test like this. Advise how we should be, we really want a boy.
Dear Elena, first of all – in no case do not give up new attempts to get pregnant and give birth. Based on 19 years of experience in gynecology, I can judge that an undeveloped pregnancy, as a rule, is followed by a new one, which ends with the birth of a long-awaited baby. This is also proved by medical statistics – about 80% of patients after an undeveloped pregnancy safely bear and give birth to healthy children.
The main thing you need to do is to undergo an extended, thorough examination to find out the reason that caused your fetal growth to stop.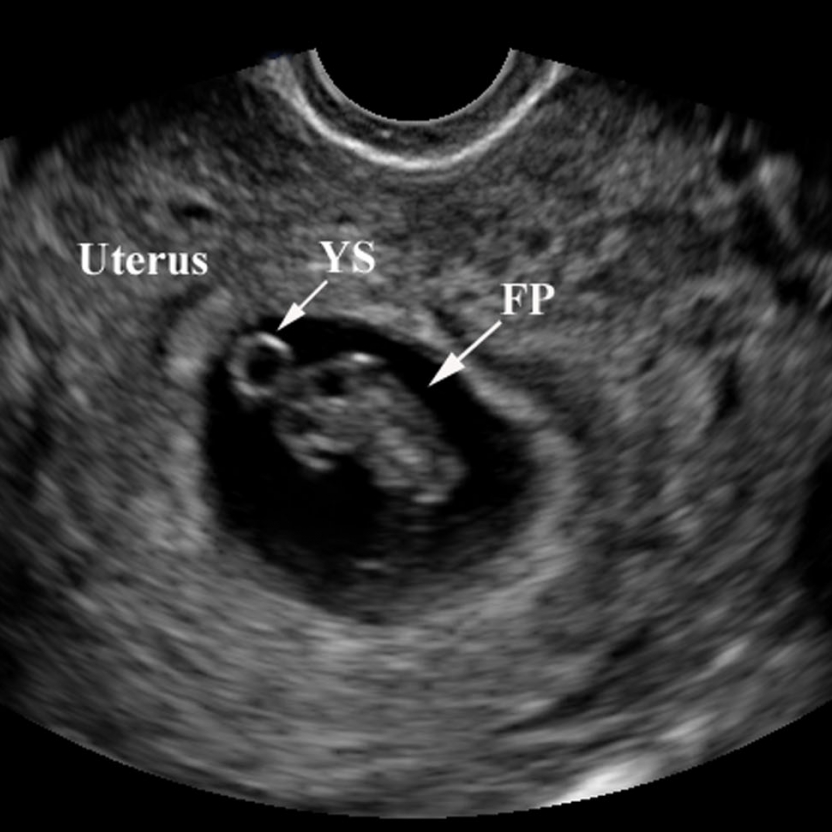 You and your husband need to be tested for infections, visit a gynecologist, urologist, endocrinologist. Our Center accepts all these specialists, and all of them are experienced doctors with high qualifications, “armed” with the latest diagnostic equipment and technologies. They will certainly help you not only to detect and eliminate the cause of fetal death, but also give recommendations on planning a new pregnancy.
You and your husband need to be tested for infections, visit a gynecologist, urologist, endocrinologist. Our Center accepts all these specialists, and all of them are experienced doctors with high qualifications, “armed” with the latest diagnostic equipment and technologies. They will certainly help you not only to detect and eliminate the cause of fetal death, but also give recommendations on planning a new pregnancy.
For those who take a responsible and serious approach to pregnancy planning, our Center has developed a special program “I want to become a mother!”, which includes consultations with an obstetrician-gynecologist, a wide range of tests and smears, ultrasound of the pelvic organs and mammary glands, colposcopy – one in a word, everything to assess the readiness of your body for such an important stage in the life of every woman. Please note that you can start planning a new pregnancy no earlier than 6 months after the termination of the previous one. Well, of course, I wish you that your dream comes true and that you give birth to a healthy boy!
-
Doctor:
Tanchuk Elena Valerievna
03/27/2021
The lifestyle of the father and his age affect the health of the child
American scientists have proven that age, addiction to alcohol and other bad habits of the father can cause congenital birth test test test test test test . ..
..
Read more
03/20/2021
Expertise on contraception
Portal “Medicine about me” and experts obstetricians and gynecologists – about contraception for young people. In developed countries, about 40% of adolescents aged 15-19 years…
Read more
02/15/2021
10 questions about IVF
In a couple of years, the world’s first “test-tube baby” – Lisa Brown – will turn 40 years old, and already in this, 2016, the first children conceived by me…
Read more
01/14/2021
Together against cancer
In “MEDICA” – the month of the fight against cancer. February 4th is World Cancer Day. Realizing the importance of this problem, the Med…
February 4th is World Cancer Day. Realizing the importance of this problem, the Med…
Read more
All articles
Address
Family Planning Center “MEDICA”
Address:
Torez Ave., 72 (hospital of the Russian Academy of Sciences, 2nd floor)
specific
lakes
Pl.