






2 year old still babbles: 2-Year-Old Not Talking but Babbling: Should You Worry?
2-Year-Old Not Talking but Babbling: Should You Worry?
Toddlers are busy little beings. They walk, talk, and explore the world around them with fascinating curiosity.
You may notice that your child’s development goes at its own unique pace. And that’s OK — at least most of the time. Still, if you’re worried that your 2-year-old isn’t talking as much as their peers, or that they’re still babbling versus saying actual words, it’s a valid concern.
Understanding what’s developmentally appropriate at this age can help you know if your tot is on track. Here’s more about the milestones, what to watch for, and how you can seek help for potential issues.
Related: Language milestones at 1 to 2 years
By age 2, milestones for speech and language include having a vocabulary of 50 or more words, even if they aren’t pronounced perfectly or understood by strangers. Your tot may also call their favorite foods by their correct names and make various animal sounds — moo, baa, cluck, oink — when prompted.
Two-word phrases also emerge (e.g., “want food”), as well as the use of pronouns like “mine,” by your child’s second birthday.
Between the age of 2 and 3, your child may know between 200 and 1,000 words. That’s a big jump in vocabulary! They may begin to understand and speak about spatial concepts, such as “on” or “in.” They also demonstrate a better understanding of pronouns and know words to describe people, places, and things, including “happy” or “sad” and “big” or “small.”
Other milestones include:
- using two- to three-word sentences (e.g., “I want more” or “I see that”)
- speaking more clearly so that caregivers can understand
- answering simple questions
- using more pronouns, such as “I,” “you,” or “me”
- adding appropriate inflection to questions (e.g., “my turn?”)
- beginning to use plural words by adding “s” to everyday words, like “toys” or “shoes”
- beginning to use past tense for verbs, like “walked” or “jumped”
It’s important to note that children of this age still may leave the ends off of words. They may also not speak in a way that’s totally understood by strangers. When they’re 2, you or other caregivers may only understand around 50 percent of the words your child says.
They may also not speak in a way that’s totally understood by strangers. When they’re 2, you or other caregivers may only understand around 50 percent of the words your child says.
As your child gets closer to age 3, their speech may be understood fairly well by the people in your family or others who regularly care for them.
Related: Does my toddler have a speech delay?
You may have heard that speech delays are associated with autism. This is true, but delays can exist on their own as well. In general, children with isolated speech delays tend to meet their milestones in other areas of development — just not in speech or language.
For example, your child may have trouble speaking but does respond when their name is called or can use other ways to communicate, such as shaking their head yes or no, using sign language, or vocalizations. Your child may not have a large vocabulary, but they can follow age-appropriate directions or use age-appropriate social skills.
Children with autism spectrum disorder (ASD) may have speech delays, as well as difficulty with communicating in general. For example, you may notice your child doesn’t respond to their name or follow directions. Your tot may not point toward objects or use other gestures.
Other features of autism include:
- Additional communication issues. These include repeating certain words or phrases and losing words or phrases that were once in their vocabulary. You may also notice that when your child does speak, they do so in a robotic, sing-song, or other unusual tone of voice.
- Social challenges. In children with autism, these include things like limited eye contact and trouble reading cues, such as facial expressions or body language, among other challenges.
- Repetitive behaviors. Rocking or hand-flapping are other signs of autism. Your little one may be extremely focused on certain interests, play with their toys only in a specific way (e.
 g., lining up dolls or spinning crayons), or even seem interested in just one part of a specific toy, such as the buttons on a doll’s dress.
g., lining up dolls or spinning crayons), or even seem interested in just one part of a specific toy, such as the buttons on a doll’s dress.
 g., lining up dolls or spinning crayons), or even seem interested in just one part of a specific toy, such as the buttons on a doll’s dress.
g., lining up dolls or spinning crayons), or even seem interested in just one part of a specific toy, such as the buttons on a doll’s dress.Being extremely troubled with breaking a normal routine is yet another common characteristic of ASD.
Resist the urge to self-diagnose your child, and bring up any concerns with your child’s pediatrician. Some of the behaviors above may be part of your toddler’s personality or development. Experts say that a doctor’s diagnosis of autism at age 2 can be “very reliable” but note that it often takes longer for most kids to get a final diagnosis.
Related: How early can autism be detected?
Outside of ASD, there are a number of reasons your child may experience a speech or language delay. Primary causes are those that can’t be attributed to some other condition affecting your child.
Speech and language are two different things. Speech is the way your child forms words and sounds, while language is how your child applies meaning to those words and communicates. Children can have trouble saying words, putting them together, or other issues with speech and language.
Children can have trouble saying words, putting them together, or other issues with speech and language.
Some primary causes include:
- Developmental expressive language disorder (DELD). Children with this condition have trouble expressing themselves with speech, gestures, and writing (though trouble with writing won’t be noticeable with a toddler). The cause of this disorder is unknown.
- Receptive language disorder. On the flip side, children with receptive language disorder have trouble understanding and processing language they hear. These kids may hear the words around them but have trouble connecting the words to their meanings. As with expressive language disorder, the cause is generally unknown.
Other secondary conditions that may also cause delays in speech and language. This means the delay is caused by another condition that affects another part of your child’s body or brain. For example, the ears or soft palate of the mouth.
They include:
- cerebral palsy
- childhood apraxia of speech
- dysarthria
- hearing loss before or after speech is developed
- intellectual disability
- selective mutism
Related: Speech disorders
In the United States, children are eligible for a free federal program called “early intervention” until age 3. This program covers every area of a child’s development, from physical skills to emotional skills and beyond.
In regards to language and speech, audiologists and speech-language pathologists help children with communication skills, including listening, talking, gesturing, and overall understanding.
You may also get in touch with your state’s early intervention program directly. Simply call and say, “I have concerns about my child’s development, and I would like to have my child evaluated to find out whether they’re eligible for early intervention services.”
After your first contact, your child will be evaluated by a professional to discover their individual set of needs. If your little one is eligible, they may undergo more tests or observations so your child’s team can write up an Individualized Family Service Plan.
If your little one is eligible, they may undergo more tests or observations so your child’s team can write up an Individualized Family Service Plan.
As the name implies, each child’s plan will be catered to their needs and the corresponding potential treatments. As a caregiver, you help decide what’s part of your child’s plan.
Therapy activities for toddlers might involve:
- playing games
- reading books to interact through language
- practicing with sounds and syllables
Sessions may take place in your home or at a nearby school, day care center, or other public space.
You, as the parent, may also be able to help your child with speech therapy with proper training from a speech-language pathologist. Experts share that children exhibit a more varied response to learning from their parents, though, so be sure to work with professionals when coming up with your ultimate plan.
Discussing any concerns you may have with your child’s pediatrician is a good idea, too. They can help with the evaluation, as well as recommend and help coordinate any appropriate medical testing, such as a hearing test, and potential specialist referrals.
They can help with the evaluation, as well as recommend and help coordinate any appropriate medical testing, such as a hearing test, and potential specialist referrals.
What about after age 3?
Is your child almost 3? Before their birthday, your early intervention team will help write a transition plan for the next stage of therapy/support. Some states continue to offer early intervention after this age — your team can give you more information on the specifics. For others, services may be available through their local school district.
Related: What is speech therapy?
Keep in mind that every child is different, and every treatment plan is individual. Your little one may respond quickly to therapy (if needed) or, on the other hand, they may take some time to get the hang of things.
That said, in instances of an isolated speech and/or language delay that isn’t associated with another condition, early treatment can be helpful. Experts at the American Academy of Family Physicians share that children in this category typically have normal speech by the time they enter kindergarten.
One study followed late talkers from the time they were 20 to 34 months until they were in kindergarten and beyond. It found that 74 percent of the group had normal speech and language skills by the time they reached school.
A more recent study showed that late talkers may have more emotional or behavioral issues at age 2 due to not being able to adequately express themselves. However, over time these children didn’t show a significant difference in these areas when compared with their peers.
For speech and language delays caused by secondary issues, your child’s progress will likely depend on the cause and continued treatment therapies. Don’t lose hope. Continue to reach out to your child’s pediatrician or early intervention specialist for guidance and support.
There’s a lot you can do at home to promote good speech and language skills in the early years. Try reading to your toddler daily. You can also sing songs and talk out loud as you go about the day’s tasks to get your little one hearing more words and sentences.
If you still have concerns about your child not reaching speech or language milestones, consult your pediatrician. You don’t need a referral for early intervention services, but your child’s doctor may be able to point you in the right direction for help. The key is to identify potential issues and get support as soon as you can.
And don’t worry if you’re unsure about whether your family needs services. Leave that part up to the professionals and continue to advocate for your child.
First Words, Gestures, and More
Language Milestones 1 to 2 Years: First Words, Gestures, and More
By Dr. Anna Kaplan on June 12, 2018
Language milestones are successes that mark various stages of language development. They are both receptive (hearing and understanding) and expressive (speech). This means that in addition to being able to make sounds and words, your baby also needs to be able to hear and understand.
Most children speak their first word between 10 to 14 months of age.
By the time your baby is a year old, he or she is probably saying between one to three words. They will be simple, and not complete words, but you will know what they mean. They may say “ma-ma,” or “da-da,” or try a name for a sibling, pet, or toy. If they aren’t doing this at 12 months, you should not be worried, as long as they are producing lots of sounds, seem like they are trying to speak, and seem to understand you. They should be using gestures, responding to their name, and stopping activity when they hear “no.” They probably enjoy playing peek-a-boo.
While nothing quite matches the thrill of hearing the first word, or seeing the first step, the language development during this year can be a lot of fun. There are lots of games to be played as your baby learns words. You also will increasingly be able to understand your child, and this makes many things easier; they will also understand you better. Children are very proud of what they are learning during this time and enjoy announcing new words. Talking to your child often and reading to them starting no later than 6 months will go a long way towards helping with language development.
Talking to your child often and reading to them starting no later than 6 months will go a long way towards helping with language development.
- The first word – If your child hasn’t already spoken their first word, they will soon. Most children speak their first word between 10 to 14 months of age. More true words will follow the first one.
- Gestures – Your child may use a lot of gestures with words to try and get the meaning across to you. As time goes on, there will be more words than gestures.
- Parts of the body – By around 15 months, your child will be able to point to some parts of the body when you name them.
- Naming familiar objects – They will begin to be able to name some familiar objects between 12 and 18 months.
- Listening – During this time, they will enjoy being read to and listening to songs and rhymes. They will begin to be able to name familiar objects that you point to in a book.
- Vocabulary – By 18 months of age, most children have at least ten words. After 18 months, word acquisition increases dramatically. There may be a “word spurt” after a child has a vocabulary of 50 words. Some children then learn new words at a very rapid pace. Your child will be able to use and understand many words by 24 months of age.
- Name – By 24 months, your child should be referring to themselves by name.
- Directions – Your child will understand and follow simple directions between 12 and 15 months of age. By the age of two, they should be able to understand more complicated sentences.
- Two word “sentences” – By 24 months, they will also be putting two words together. This could be their name and a request, or your name and a request, or a question, like “mama car?”
 After 18 months, word acquisition increases dramatically. There may be a “word spurt” after a child has a vocabulary of 50 words. Some children then learn new words at a very rapid pace. Your child will be able to use and understand many words by 24 months of age.
After 18 months, word acquisition increases dramatically. There may be a “word spurt” after a child has a vocabulary of 50 words. Some children then learn new words at a very rapid pace. Your child will be able to use and understand many words by 24 months of age.Children master different language skills at different ages.
Words will still not be perfect. Your child will start using some of the harder consonants, first the d, n, and t, which are produced between the tongue and the roof of the mouth.
That will be followed by g, k, and ng, which are made farther back inside the mouth.
During this year, your child will use more consonants, although they may be mixed up, and they may drop the syllables at the end of words.
- Understanding simple words – You should be concerned if your child does not understand the words no, bye-bye, and bottle (if appropriate) by the age 15 months.
- Vocabulary – Your child should use single words by 15 to 16 months of age at the latest. They should have a 10-word vocabulary by 18 months of age.
- Following directions – They should be able to follow simple directions by the time they are 21 months old. An example would be “Come here.”
- Excessive jargon or babbling – A two year old should not be mainly babbling. They should be using more real words.
- Body parts – At two, your child should be able to point to a number of body parts.
- Two word phrases – A two-year-old should be putting two words together.
You will still have many visits to the pediatrician during this year. The doctor will still be evaluating your child’s development, including language development. You should share any concerns you have.
You should share any concerns you have.
It is still important to remember that every child is different and may master different language skills at different ages. You should be looking for evidence of increasing mastery of language and growth of vocabulary. Your child should be increasingly able to understand you. This should be easy for you to recognize as you read to and play with them.
- Parenthood
- Toddler
By Dr. Anna Kaplan on June 12, 2018
related stories
-
Language Milestones: 0 to 12 months
-
Developmental Expressive Language Disorder (DELD)
-
How to Teach Your Toddler to Talk
-
When Do Babies Know Their Name
-
Ages and Stages: How to Monitor Child Development
Read this next
-
Language Milestones: 0 to 12 months
Language milestones are successes that mark various stages of language development.
They are both receptive (hearing) and expressive (speech). This…READ MORE
-
Developmental Expressive Language Disorder (DELD)
Medically reviewed by Karen Gill, M.D.
If you have a child with developmental expressive language disorder (DELD), they might have difficulty remembering vocabulary words or using complex…
READ MORE
-
How to Teach Your Toddler to Talk
Medically reviewed by Karen Gill, M.D.
From the first word to sentences, questions, and more, language is an exciting developmental process. If you are wondering how to help your toddler…
READ MORE
-
When Do Babies Know Their Name
Medically reviewed by Karen Gill, M.D.
In the first year, a baby’s speech and language development takes off. Learn about development milestones between your baby recognizing their name and…
READ MORE
-
Ages and Stages: How to Monitor Child Development
Medically reviewed by Karen Gill, M.
D.Stages of child development are important measures of growth and maturity. There are many tools to measure development. Here’s a list of developmental…
READ MORE
-
Support for the Non-Birthing Partner after Stillbirth
Medically reviewed by Matthew Boland, PhD
The grief that accompanies stillbirth or infant loss isn’t reserved for the birthing parent — partners also feel this loss deeply.
READ MORE
-
How to Offer Support After Infant Loss or Miscarriage: A Guide
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
We spoke with parents who offered suggestions for how to support them after miscarriage, infant loss, and stillbirth.
READ MORE
-
Preeclampsia and Pregnancy: Blood Pressure Drug May Help in Severe Cases
Researchers say the medication nifedipine was effective in helping pregnant women with preeclampsia avoid dangerously high blood pressure
READ MORE
-
Unexplained Recurrent Pregnancy Loss: My Journey to Baby Number 2
Healthline writer Ashley Marcin shares her story of multiple fetal losses and how they affected her and her family.
READ MORE
-
Stillbirth vs. Miscarriage: How They’re Similar and How They’re Different
Stillbirth and miscarriage are two terms that describe a painful event: pregnancy loss. Learn how they are different and how they are similar.
READ MORE
 They are both receptive (hearing) and expressive (speech). This…
They are both receptive (hearing) and expressive (speech). This… D.
D.
Apraxia of Speech (AOS): Symptoms, Diagnosis, and Treatment
Apraxia of speech (AOS) is a speech disorder in which someone has trouble speaking. A person with AOS knows what they’d like to say but has difficulty getting their lips, jaw, or tongue to move in the proper way to say it.
In order to speak, your brain needs to send a message to your mouth. AOS affects the pathways of the brain that are involved in planning and coordinating the movements that are necessary for speech. Because of this, the messages from the brain don’t get through to the mouth correctly.
There are two main types of apraxia of speech:
- Childhood AOS. Present from birth, this type of AOS is diagnosed during childhood. Genetics may play a role in the speech disorder, and it appears to affect boys more often than girls.
- Acquired AOS. This type of AOS can affect anyone, but it most commonly occurs in adults. It’s caused by damage to the brain by something such as a stroke, traumatic brain injury, or brain tumor.
 Present from birth, this type of AOS is diagnosed during childhood. Genetics may play a role in the speech disorder, and it appears to affect boys more often than girls.
Present from birth, this type of AOS is diagnosed during childhood. Genetics may play a role in the speech disorder, and it appears to affect boys more often than girls.It’s important to remember that AOS is a complex condition, and the severity and symptoms can vary from person to person.
In some people, it may be very mild, with the person only having difficulties with a few sounds or words. In more severe cases, someone may experience great difficulty speaking at all.
Additionally, some people may only have very few symptoms of AOS, while other people may have many symptoms.
Childhood AOS symptoms
These are some childhood AOS symptoms:
- delayed first words
- only being able to produce a few different types of sounds
- syllables or sounds that aren’t put together in the right order
- saying the same word in different ways
- lengthy pauses between sounds or difficulty moving between sounds and syllables
- putting stress on the incorrect syllable of a word or using equal emphasis for all syllables
- putting stress on the incorrect syllable of a word or using equal emphasis for all syllables
- having more trouble with longer words
- having difficulties imitating what another person is saying
- having to move the lips, jaw, or tongue several times in order to make a sound
- appearing to understand spoken language better than they can speak it
Acquired AOS symptoms
Many of the symptoms of acquired AOS are similar to those of childhood AOS.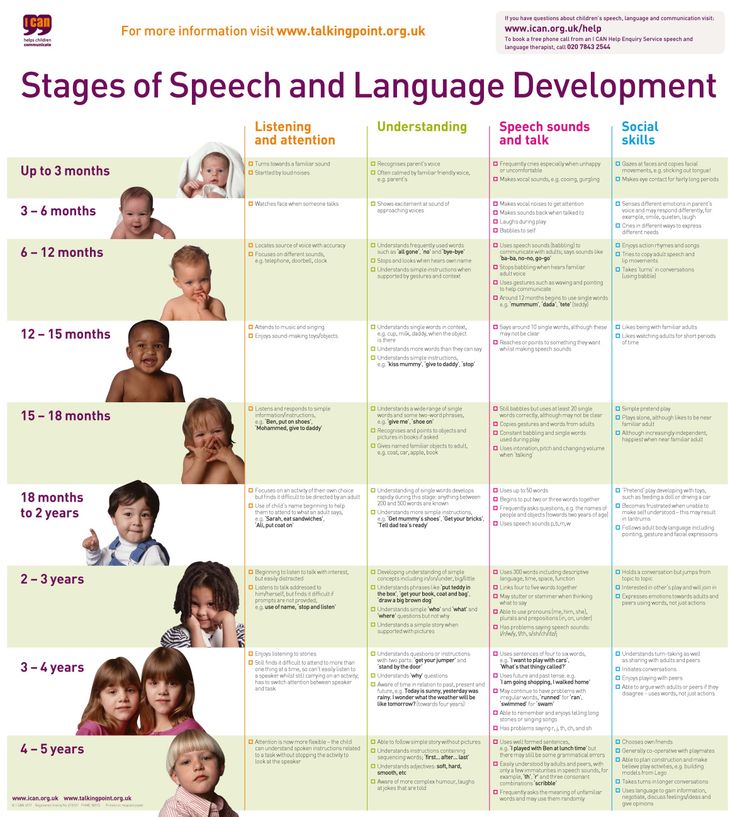 Some of these symptoms can include:
Some of these symptoms can include:
- a slower rate of speech
- distortions of sounds, which can also include sound additions or substitutions
- long pauses between syllables
- placing an equal amount of stress on all syllables in a word
- having to move the lips, jaw, or tongue a few times before speaking
Childhood AOS causes
Researchers do not fully understand what causes childhood apraxia of speech. They think it may be genetic and could be related to overall language development or an issue with the brain’s signals to muscles used for speech.
In some cases, the condition may occur as part of a larger, more complex disorder, such as:
- autism spectrum disorder
- epilepsy
- cerebral palsy
- galactosemia
- a neuromuscular disorder
Childhood AOS may run in families. Many children diagnosed with the condition have a family member with a communication disorder or learning disability. It appears to affect boys more often than girls.
Acquired AOS causes
Acquired AOS can affect anyone, but it occurs most commonly in adults. It is usually caused by an injury that damages the parts of the brain responsible for planning and programming muscle movements necessary for speech.
Here are the most common causes:
- stroke
- traumatic head injury
- tumor or surgical trauma
- neurodegenerative diseases
The condition may present together with other conditions, such as dysarthria (slurred speech) and aphasia, which also causes communication difficulties.
In both children and adults, a professional speech-language pathologist (SLP) works to diagnose and treat AOS. Since the symptoms of AOS may vary from person to person, diagnosis can be difficult.
In addition to taking the person’s medical history, the SLP will look for the presence of groups of symptoms that can be indicative of AOS. They’ll also work to rule out other conditions like:
- aphasia
- muscle weakness
- hearing disorders
Childhood AOS diagnosis
The SLP can use various methods to assess if your child has childhood AOS. Your child’s SLP may:
Your child’s SLP may:
- ask your child to repeat the same word or syllable several times
- request that your child read from a list of increasingly long words
- assess how your child makes specific vowel or consonant sounds
- listen to your child’s flow of speech to see how they stress different syllables and words or move from one syllable or word to another
- see how well your child’s speech can be understood by others
- give hearing tests to rule out issues with hearing that could be contributing to your child’s speech problem
- assess your child’s lips, tongue, and jaw for any structural issues or muscle weakness
Sometimes in order to make a diagnosis of childhood AOS, the SLP will need to evaluate your child’s speech over a period of time as opposed to in just one session.
Acquired AOS diagnosis
Adults who’ve had a stroke or other type of brain injury may be evaluated for AOS. Similar to the diagnostic process for childhood AOS, the SLP can use a variety of assessments to help them make a diagnosis.
Your SLP may:
- ask you to report any language or communication difficulties you’ve been having
- listen to how you pronounce and apply emphasis to syllables or words
- compare speech you come up with yourself versus speech you’re asked to imitate
- assess the rate at which you communicate verbally
- evaluate how well something you’ve said can be understood
- check your lips, tongue, or jaw for any muscle weakness that may be contributing to your condition
- listen to how your voice sounds — for example, is it harsh, breathy, or weak?
In addition to evaluating your verbal communication skills, the SLP may also ask you to perform tasks that include reading, writing, and nonspeech movements as part of the diagnostic process.
A child with childhood AOS will require treatment, as the condition typically doesn’t improve on its own. However, some cases of acquired AOS may actually improve on their own, which is called spontaneous recovery.
For both children and adults, the treatment for AOS involves speech-language therapy. The specific approach is customized to the individual and takes into account the severity of their condition and the specific difficulties they have with speech.
- asking for the same word or phrase to be repeated multiple times
- practicing saying specific syllables or words to help you learn to move from one sound to another
- having you carefully observe how the therapist’s mouth moves when they say words or phrases
- using visual cues, such as practicing speech in front of a mirror, to remind yourself how to move your mouth to say specific words or phrases
Speech therapy sessions for AOS are typically one-on-one and occur often. As improvement occurs, they may occur less often. Additionally, practice at home with family members is also encouraged.
In more severe cases of AOS, alternative forms of communication may be taught as part of your treatment. This can include things like hand gestures or sign language that you can use to help you communicate with others.
This can include things like hand gestures or sign language that you can use to help you communicate with others.
Childhood AOS
In identifying any type of speech or language disorder, it may be helpful to compare the way your child speaks and communicates with the typical milestones for these skills. The American Speech-Language-Hearing Association (ASHA) provides detailed guidelines by age.
Since identifying and treating childhood AOS early can help lower the risk of long-term speech problems, you should be sure to see a doctor if you notice that your child is having problems speaking.
Acquired AOS
If you’re an adult and find that you’re having trouble speaking, be sure to see a doctor. It’s very important that you’re assessed to determine the cause of your condition and to make sure that it doesn’t get worse.
Apraxia of speech is a speech disorder in which you know what you want to say, but you have trouble moving your mouth properly to say it. This isn’t due to muscle weakness or atrophy but instead happens because the signal from your brain to your mouth is disrupted in some way.
This isn’t due to muscle weakness or atrophy but instead happens because the signal from your brain to your mouth is disrupted in some way.
There are two types of apraxia of speech — childhood and acquired. Both can be diagnosed and treated by a speech-language pathologist. If you find that you or your child is having trouble speaking, you should be sure to see the doctor to find out the cause of your condition.
The child understands everything, but does not speak. What is the reason?
The problem of the timely formation of speech always worries parents. Even if the grandmother tries to console, they say, nothing, dad spoke late, and yours is all right. Sometimes, indeed, the child simply develops at his own pace and over time begins to chat no worse than his peers.
However, speech delay problems can be much deeper and it is very important to pay attention to them in time. After all, the sooner the correction begins, the greater results can be achieved.
Expressive speech disorder
“Understands everything but does not speak” is one of the biggest traps. Parents are sincerely perplexed why their child lags behind in the development of speech, because he clearly understands well the speech addressed to him and is quite developed intellectually. Sometimes this fact does not allow you to notice obvious problems with speech.
Absence or impairment of speech with full understanding of the phrases addressed to the child is called a disorder of expressive speech. As a rule, parents begin to pay attention and sound the alarm when, by the age of three, their child has not spoken.
What characterizes this condition :
- the child does not speak at all;
- in speech there are babbling words, syllabic forms of words, onomatopoeia;
- after the age of three, the child does not build sentences from words, limiting himself to a small vocabulary. Perhaps the child has dysarthria.

At the same time, it is very important to note other important features:
- The child’s intelligence is completely preserved. He understands words and requests well, fulfills them without difficulty.
- Both physiological and mental development is normal.
- The child is able to maintain contact, he does not have signs of autism.
- Available active gestural communication, adequate facial expressions, etc.
- No hearing problems.
Why doesn’t he speak?
So why is it that a child who absolutely understands everything that is spoken to him lags behind in speech development? If the process is not “slowed down” by either the intellectual or the mental component, what is the matter?
Experts identify two types of reasons that can cause problems in expressive (inverted) speech:
- Social.
- Physiological.
External causes:
- Lack of motivation in the child. It may sound strange, but excessive care and attention does not stimulate in children the desire to express their needs through speech. If absolutely all desires are anticipated, and the gestural “alphabet” is grasped by loving relatives on the fly, then why bother?
- Missing example. Children in socially disadvantaged families often have problems with the development of speech, since communication and activities with the child are minimized there. However, quite “positive” parents sometimes believe that the baby needs only care and provision of physiological requirements. All experts are sounding the alarm – children are sometimes surrounded only by voices sounding from the TV and modern gadgets.
- Bilingualism. If a family speaks two languages at the same time, it is difficult for a child to isolate the lexemes of one of them. For this reason, bilingual children begin to speak later than their peers growing up in a monolingual family. At the same time, they can understand the speech of their parents well.
- Excessive demands. The child may refuse to speak if the parents are too insistent on this from him. The situation when the baby, having barely tried a word, is constantly subjected to requests to say it again and again, is quite common. It will be better if the family tries to create motivation for communication, and not pressure on the child.
 It may sound strange, but excessive care and attention does not stimulate in children the desire to express their needs through speech. If absolutely all desires are anticipated, and the gestural “alphabet” is grasped by loving relatives on the fly, then why bother?
It may sound strange, but excessive care and attention does not stimulate in children the desire to express their needs through speech. If absolutely all desires are anticipated, and the gestural “alphabet” is grasped by loving relatives on the fly, then why bother? Note to parents: The process of language formation in children is based on the child’s natural ability to learn from the environment. That is why regular communication with even the smallest child is so important. However, moms and dads should take note that speech from TV and other sources cannot teach a baby to speak, perceived as noise, until he masters his native language.
Internal causes:
- Heredity. A genetic factor cannot be ruled out. If one of the parents spoke later than the deadline, then it may very well be that the child will repeat his story. However, experts advise in this case to be on the alert.
The fact is that with each subsequent generation the situation can become more complicated.
- Neurological problems. Quite often, speech delay is based on damage to the speech areas of the cerebral cortex. The trigger mechanism can be intrauterine hypoxia, difficult childbirth, injuries and serious illnesses suffered by a child at an early age.
- Disorders of the organs of articulation. Short frenulum of the tongue, reduced tone of the muscles of the face and articulatory organs, etc. lead to the inability to pronounce sounds, and therefore delay the development of speech.
If the child does not speak, the Tomatis method helps a lot
What to do if the child understands everything but does not speak?
First of all, parents should definitely pay attention to this. Do not relax and wait until the child enters into a conversation on his own. Speech delay can lead to other problems, including a lag in mental and intellectual development.
The fact that a child perceives the speech of others well and fulfills all requests can dull his vigilance – thank God, he is intellectually developed enough! However, if problems occur after reaching the age of three, it is necessary to take action.
Contact:
- Start with your pediatrician. He will direct you to the right specialist.
- Visit a neurologist. If the reason for the delay in speech is a violation related to his competence, the doctor will prescribe an appropriate treatment.
- Do not put off a visit to a speech pathologist. Timely measures taken and regular classes will help the child catch up with peers and successfully prepare for the future.
Publication date: 02/08/2017. Last modified: 08/02/2022.
Early Childhood Speech Development Calendar
Early childhood is considered a very important period in a child’s life.
This is the time of the most rapid and rapid changes in the mental and physical development of the baby, the child takes the first steps, learns to speak, begins to use gestures and other means of communication.
3 weeks – 1 month – there is a cry indicating emotional discomfort, pain or hunger. With physical stress, the child groans, making the sounds “a”, “e”.
2 – 3 months : the child has a cooing, he pronounces simple sounds – “ a”, “y”, “s ”, sometimes in combination with “ g ”. This is an important stage in the development of speech in young children.
4 – 6 months – emits high melodious sounds, sounds of exclamation, reacts with joyful sounds to the faces of loved ones.
6 – 9 months – babbles, he repeats the same syllables (“ma-ma-ma”, “ba-ba-ba”, “dya-dya-dya”, “gu-gu-gu”).
9 – 11 months – the baby begins to imitate the sounds of adult speech.
11 – 14 months – the first meaningful words “mom”, “dad”, “woman”, “uncle” appear, from 8 to 14 words. Correlates a word with an object
By the age of 2 years there are 100-200 words in the baby’s vocabulary. He is already building a sentence of 2-3 words.
He is already building a sentence of 2-3 words.
By the age of 3 the volume of the dictionary increases to 1000 words by enriching the child’s life experience. Simple prepositions appear: in, on, under, for, with, at. The child remembers poems, children’s songs.
By the end of 3 years , most children are able to construct a sentence grammatically correctly, conduct dialogues, tell what, what they saw and heard.
Important to know:
Do not listen to advice from other parents whose children began to say after 3 years that the child will speak on his own. He will speak, the only question is what kind of speech it will be, its quality.
How can I tell if my child has speech problems?
By the end of 1 month the child does not cry before feeding
By the end of 4 months does not smile when his mother talks to him, does not coo.
By the end of the 5th month does not listen to sounds and music
By the end of the 7th month does not react to the intonation of the voice, does not recognize the mother’s voice with a “revitalization complex”
By the end of the 9th month there is no babbling, the child does not repeat sound combinations and syllables after the adult
By the end of 1 year the child does not wave his head when saying goodbye as a sign of denial. He does not utter a single word and does not follow simple instructions: “give”, “on”, “take”.
By the age of 1.5, does not show or name mom and dad, does not build a tower of blocks, does not differentiate sounding toys, does not use a pointing gesture.
By 2 years does not show parts of the body, does not show mom and dad in the photo, does not follow the two-step instruction (go to the kitchen and put the plate on the table)
By the age of 2. 5, does not distinguish between “big and small”, does not communicate with children.
5, does not distinguish between “big and small”, does not communicate with children.
By the age of 3, cannot give his first and last name, tell a simple poem and a fairy tale.
If this does not happen, there is a reason to contact specialists.
Possible causes of speech disorders
- Viral and endocrine diseases of the mother, the threat of miscarriage, trauma, toxicosis, low hemoglobin levels.
- Genetic anomalies, hereditary predisposition.
- Unfavorable delivery.
- Diseases suffered by a child in the first years of life
- Babies with low Apgar scores at birth
The exact cause of the disorders is determined by the doctor, and the type of speech disorder is determined by the speech therapist.
So what can parents do to improve language development?
Speech is the highest mental function, so the period of intrauterine development of a child is very important. Parents need to take care of the development of speech even before his birth. It is important that the expectant mother receives only positive emotions i.
Parents need to take care of the development of speech even before his birth. It is important that the expectant mother receives only positive emotions i.
Communicate more with your baby! Goodwill, a soft and calm voice, grammatically correct speech is another important factor in the development of speech.
Children often get what they want with just a pointing gesture. Teach your child to express his desires as fully as possible, say new words, sentences.
Do not scold your child for mispronounced words. This can provoke neurotic reactions. He will shut up, stop speaking and learning new words.
Develop your baby’s ability to listen and pay attention. Play games with him that help him develop his ability to listen and hear: “Listen, what’s ticking there? And what’s that noise?” Let the baby learn to distinguish between speech and non-speech sounds (environmental sounds).
Teach your child fairy tales, poems, because memorizing them and repeating, he learns new words, trains memory and attention.
Important to know:
Speech disorders can be corrected – it is important not to waste time!
Author-compiler: Mikhnovich O.F speech pathologist
when to panic and where to seek help • 02/08/2020 • Reading • Sibdepo
The specialist begins talking about the causes of speech disorders with the story of his son. The guy is diagnosed with autism.
The first story. Personal experience.
“Vladimir is now 15, and all these years we have been fighting for his life. The desired first child, a little large, and before the birth, the question arose of the possibility of a caesarean section. It must be said that I have always been far from miniature, and, probably, this is how the cards fell or the doctor strongly believed in me, but in the end I was allowed to give birth on my own. Then something went wrong. As a result, everything ended with the already forced caesarean section and fetal asphyxia.
 And, consequently, affected brain cells and unpredictable consequences that we have been solving for 15 years. That would be a caesarean immediately, there would be chances to give birth to a healthy child.
And, consequently, affected brain cells and unpredictable consequences that we have been solving for 15 years. That would be a caesarean immediately, there would be chances to give birth to a healthy child. By the way, Maria entered the profession after the birth of her special son. And not only for practical purposes, but also for educational purposes. She is sure that the availability of information kills the stereotypes of the perception of disability.
The second story. Vaccination.
“In front of me is just a child, she was barely 18. Her fragile childish shoulders shudder from internal sobs and inability to comprehend the information received from me. “Will he walk? Will he speak? Will he go to a regular school? They look at me like a magician and God rolled into one. The kid (he is about two years old) quietly sits on the floor, sorting through his tar-colored curls, looking at one point during this action.
 “We were vaccinated at a year and three, and in a week he fell silent, and this is how he sits all day.”
“We were vaccinated at a year and three, and in a week he fell silent, and this is how he sits all day.” During her ten years of practice, Maria Krasnopolskaya encountered similar stories many times. In the language of specialists, this is called “disintegration” – when the already formed skills are lost by the child due to certain circumstances at the age of about 1.5 years.
“In this example, the child was born already with the preconditions for the disease, and the vaccination became only a trigger factor for the onset of the development of the disease, it kind of started the mechanism, pressed the “on” button,” the defectologist comments.
Discussions about the benefits or harms of vaccination are very heated today. There are parents who deliberately write refusals of all vaccinations, protest noisily on the Internet, citing many quite sound arguments about the dangers of vaccination. According to the interlocutor, the baby could live well with this predisposition. But, most likely, vaccination took place after the illness, when the child’s immunity was not ready to fight foreign antibodies, and there was a “surrender”, “rollback”.
But, most likely, vaccination took place after the illness, when the child’s immunity was not ready to fight foreign antibodies, and there was a “surrender”, “rollback”.
“Unfortunately, no one canceled the human factor, and if our polyclinics did not pursue compliance with the vaccination schedule, but were more attentive to the health of young patients, statistics that 1 out of 1000 children (and these are only those who proved!) suffers from the consequences of negligent vaccination, it would not be. I emphasize: I am not against vaccinations, I am for reasonable vaccination.”
The third story. Motivating.
“When they first came to the reception, Masha was 9months. Mom had a blue-eyed miracle in her arms, and the red fluff on her head was funny bristling in different directions, and even a bright blue headband with violets did not save the situation. A family of doctors, my mother was checked for everything during pregnancy.
 In the end, everything was fine, except for one extra chromosome and the “sunny child” syndrome. There were tears, the option of a boarding school was considered, but the mind won out. In the medical record there were a bunch of diagnoses in addition to the main one. But the red-haired miracle smiled, and the rest was already unimportant. And then years of work. Now Masha is ten, she studies well and dances oriental dances, she has friends. A lot has been passed, but there is still more to go and, most importantly, on this road – not to lose hope, and to be able to enjoy every passing day.
In the end, everything was fine, except for one extra chromosome and the “sunny child” syndrome. There were tears, the option of a boarding school was considered, but the mind won out. In the medical record there were a bunch of diagnoses in addition to the main one. But the red-haired miracle smiled, and the rest was already unimportant. And then years of work. Now Masha is ten, she studies well and dances oriental dances, she has friends. A lot has been passed, but there is still more to go and, most importantly, on this road – not to lose hope, and to be able to enjoy every passing day. There are a great many reasons for delayed speech development, each case has its own. According to Maria Krasnopolskaya, the main thing here is to ask yourself the right questions. And find the answer in your heart. “For what? Why did this happen? “What can you give to this world, how to help?”.
“And rejoice in spite of everything and in spite of everything.
 Hope, she does not die in a mother’s heart.
Hope, she does not die in a mother’s heart. Worry or not?
The quality of corrective diagnostics has seriously advanced over ten years, but it is still very far from perfection, and every year there are more questions than answers, notes the interlocutor. More and more children start talking rather late.
“The child is almost three years old, and he still does not speak, and the parents begin to sound the alarm. Doctors diagnose the baby with speech development delay (SRR), because normally, by the age of three, he should already have good phrasal speech. Then everything develops according to several scenarios: someone “spits” on this diagnosis and waits for the child to speak; someone begins to worry a lot and take various measures; the rest are derivatives of the first two.
When should one focus on one or another scenario of behavior?
Scenario one, when you shouldn’t be especially worried
We look at the child and see:
- He is less than three years old, he is healthy, agile, developed according to the schedule and did not get sick in the first year of life.
- He loves running bikes, scooters and bicycles, loves swinging.
- Understands well the speech addressed to him, can fulfill a two-level request (“go there, bring that” or “take not blue”).
- He is trying to say something himself, and he has his own language: “Chu cha” – “I want tea.”
- Looks at and shows pictures in a book.
- The main thing is that he communicates actively and with pleasure. At least with my parents. Communication is not necessarily verbal, gestures are also speech. The main thing is that the child should have a desire to communicate and he should have something to say.
All these points are very important in terms of diagnosing the child’s speech development. If at least some of this is not available, with the possible exception of a balance bike and a scooter with a bicycle, you should contact a specialist.
“There are many reasons for the delay in speech development, and believe me, the situation will not change if certain measures are not taken in time.
 The delay in speech development later also inhibits mental development.
The delay in speech development later also inhibits mental development. The second scenario, when you should worry
You should be very worried if your mother was sick in the first trimester of pregnancy, and the child is unsociable, does not look into your eyes and generally does not seem to notice you. He is quite “independent”, and it seems that he does not need you at all. If the child behaves this way, you need to run to the specialists, even if the mother was not sick at the beginning of pregnancy and did not take medicine: this can signal serious problems in the development of the child, and the sooner you start doing something, the easier the consequences.
Recall how a child developed in its first year. Did he react to your voice, did he babble, was there babble (“agu-uh-hu”, “ta-ta”, “ba-ba” and the like, what happens), did he try to catch the movements of the lips and imitate them, saying what something similar to the syllables “pa-pa-pa”, “ma-ma-ma”, “tya-tya-tya”, whether he caught the intonation.
If something is wrong, you have cause for concern. These are the stages of speech development that every child must go through before pronouncing their first children’s words. You need to start with doctors, check your hearing and vision.
Next, you need to pay attention to motor awkwardness. Perhaps the child is clumsy, walks on tiptoe, often falls, or simply his “arms by themselves, legs by themselves.” Speech muscles are also muscles, and it may be difficult for a child to coordinate not only the work of the legs and arms, but also the lips, cheeks and tongue. This can be tracked by a neurologist.
“If a child seems to be active and sociable, but does not speak at all, even simple words (“mom”, “dad”, “give”, “bi-bi”), especially if he is already more than two years old, or his speech is more like soft babble, and the neurologist has already diagnosed ZRR, you need to look not for a speech therapist, but for a defectologist, or a neuropsychologist.
 It is possible that the child is simply maturing more slowly than his peers. It would be good to be sure of this and not start problems that are better solved as early as possible.
It is possible that the child is simply maturing more slowly than his peers. It would be good to be sure of this and not start problems that are better solved as early as possible. Here are the main points when you should turn to specialists – neurologists, defectologists, speech therapists, neuropsychologists. And this must be done up to three years, urges Maria Krasnopolskaya.
- A child older than 3 months – does not come to life when he hears the speech of an adult, does not show an emotional reaction to the voice.
- Older than 8 months – does not babble.
- Over 1.5 years old – does not pronounce simple words like “mom” or “give”, cannot point to objects in the picture in response to a parent’s question.
- Older than 2 years old – does not have a vocabulary of just a few words and does not expand it, and is also unable to follow the instructions of adults (“Pick up the doll and give it to me”).
- Over 2.5 years old – does not form a two-word phrase.
