Gestational sac and yolk sac but no baby at 7 weeks: What You Should See (and Why You May Not)
What You Should See (and Why You May Not)
Your first pregnancy ultrasound is usually an exciting event: You’re 12 or 13 weeks pregnant and looking forward to getting a glimpse of the baby that’s been growing for the last 3 months. You know they’re going to look like an alien, but still — they’ll be your little alien, and you can’t wait.
Sometimes, though, an earlier ultrasound is necessary, and we’ll be honest: It’s weird. Why? Because a ton of gestational development happens between 7 and 12 weeks, making an early ultrasound a completely different experience than the traditional one in your first trimester.
A 7-week ultrasound may not be the bonding experience you’re hoping for, since there’s a lot you may not see. But here’s what you can expect.
Although a 7-week ultrasound isn’t routinely performed, there are actually a bunch of reasons why your doctor might want you to have one — and not all of them fall into the “doom and gloom” category.
In fact, the most common reason doctors order ultrasounds before the 12- or 13-week point is to accurately date your pregnancy.
If your pregnancy symptoms don’t match up with your last menstrual period or there’s any confusion about how old your baby is — gestationally speaking — the measurements taken during an early ultrasound can tell your doctor exactly how far along you are in your pregnancy.
Other reasons for an early ultrasound include:
- Confirming twins or multiples. Especially if you’ve had fertility treatments, this might be something you want to confirm ASAP.
- Confirming fetal heartbeat. If you’ve had any concerning symptoms, like spotting or vaginal bleeding, your doctor will want to know if you’re experiencing a miscarriage or what the cause of any unexplained bleeding could be.
- Ruling out an ectopic pregnancy. When an embryo implants outside the uterus, you’ll often have pregnancy symptoms and a positive pregnancy test, even though the embryo isn’t viable. An ectopic pregnancy is a life threatening condition if it’s not treated, so it’s important to diagnose it.

- Checking your reproductive anatomy. Issues with your uterus, cervix, ovaries, or fallopian tubes can cause complications during pregnancy. So, if your doctor suspects you might have a problem — like uterine fibroids, for example — they may want to have that info right away.
Again, it isn’t cause for immediate panic if your doctor orders a 7-week ultrasound. Yes, it could be a worst-case scenario, but it could also just be one where you’re collecting as much info as possible so you can have a healthy pregnancy.
Pop culture has likely taught you that your first ultrasound is a beautiful experience where a technician waves a magic wand over your stomach and you get to stare at a computer screen and see the adorable shape of your baby floating peacefully in your uterus.
But that’s not what happens at a 7-week ultrasound, so let’s just blow that expectation out of the water now. (Sorry!) In most cases, your baby is too small to be seen clearly — or at all — on an external abdominal ultrasound. Instead, you’ll need a transvaginal ultrasound.
Instead, you’ll need a transvaginal ultrasound.
It sounds less than fun, we admit, and it is a less-than-fun procedure: A technician inserts an ultrasound wand, called a transducer, a few inches into your vagina until it reaches your cervix.
Then, the technician keeps it in place, adjusting the wand as much as needed to get a good look at the inside of your uterus. It’s not painful, though it may be uncomfortable.
You’ll feel about as much pressure as you do during your annual gynecology exam, for comparison. It does take longer, which can add to the overall unpleasantness, but the technicians are trained to make you comfortable — at least, as comfortable as you can be with an ultrasound wand inside in your vaginal canal.
The good news? There’s no risk to your baby from the procedure and there’s no radiation used. So, while it won’t go down in history as one of your favorite experiences, it can’t cause any harm.
Share on PinterestHave a nice day Photo/Shutterstock
A 7-week ultrasound showing crown rump length of baby, which helps figure out the age of the fetus. Surrounding the fetus is the gestational sac, which is filled with fluid.
Surrounding the fetus is the gestational sac, which is filled with fluid.
You’re not going to be counting fingers and toes at this ultrasound; the embryo is simply too tiny for clear images to be detected. You may see the general shape of your baby or be able to tell something is there, but it’s also normal to not see anything that looks very much like a baby at all.
One thing you will often see in a healthy pregnancy is your baby’s heartbeat. It could be going as fast as 110 beats per minute or more! If your baby is in a visible position on the ultrasound, you’ll probably see a little blinking or pulsing on the screen (and you should be able to hear it briefly, too).
You may see the following anatomical developments on a 7-week ultrasound:
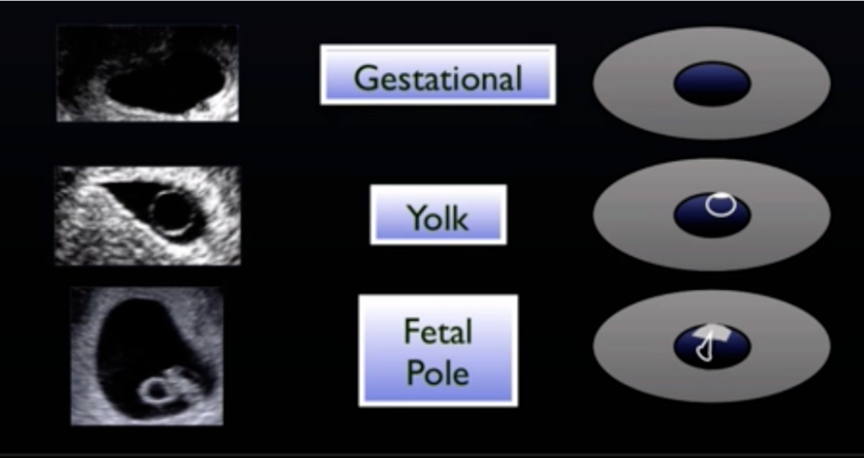
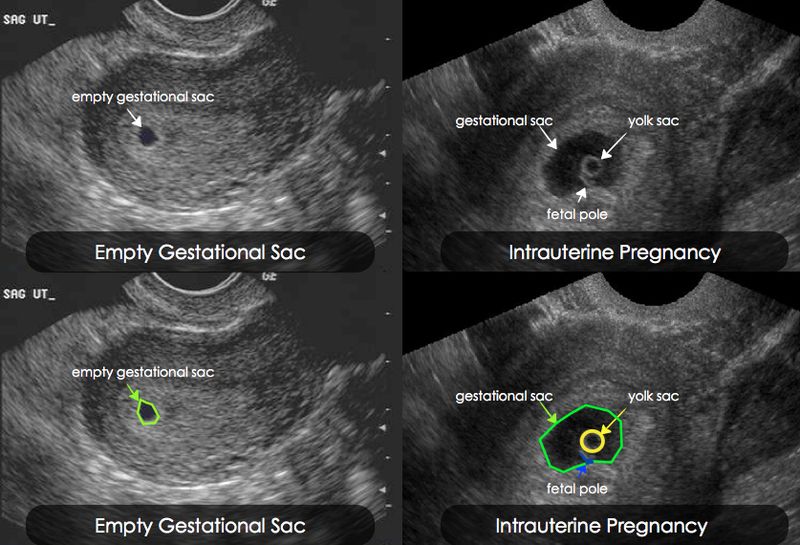
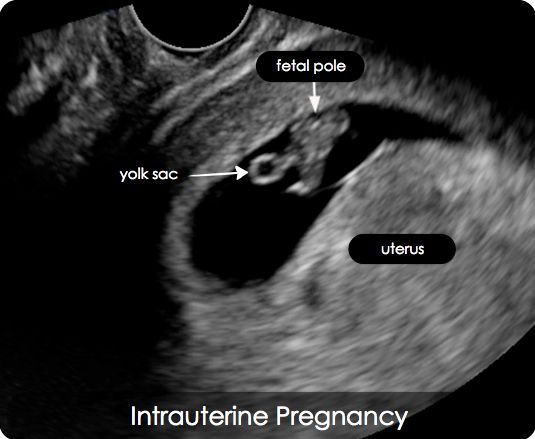
- Gestational sac. This is one of the earliest visible signs of a pregnancy, and it refers to the fluid-filled space surrounding the embryo. It’s usually formed by 5 weeks of gestation, and it can accurately confirm an intrauterine pregnancy the vast majority of the time it’s seen on an ultrasound. It will look like a clear, dark circular or oblong shape, sharply contrasted with the whitish, opaque appearance of the inside of your uterus.
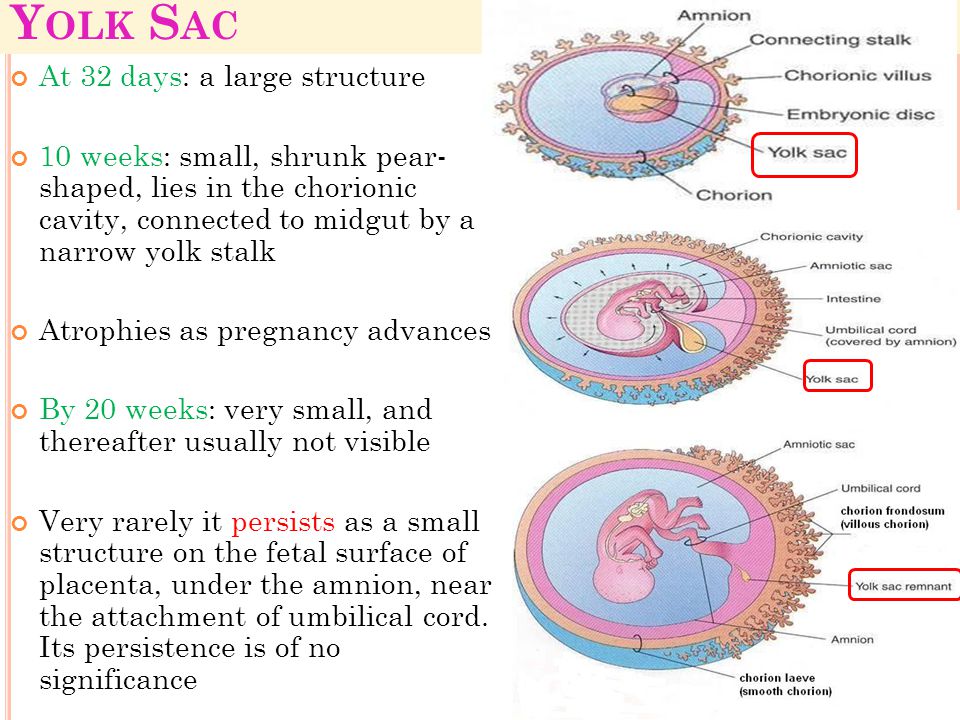
- Yolk sac. Even before you can see an embryo inside the gestational sac, you should spot the yolk sac. It’s the first thing to develop inside the gestational sac, and it provides your baby with nutrients and oxygen until the placenta develops. It’ll look like a small white ring or bubble inside the sac.
- Fetal pole. This is the first indication that your baby is forming inside the gestational sac. It will look like a thick, whitish shape attached to the yolk sac. Depending on how far along you are, it may be curved or oblong. It can usually be detected by 6 weeks of gestation on a transvaginal ultrasound. This is where you would see the baby’s heartbeat.
 It will look like a clear, dark circular or oblong shape, sharply contrasted with the whitish, opaque appearance of the inside of your uterus.
It will look like a clear, dark circular or oblong shape, sharply contrasted with the whitish, opaque appearance of the inside of your uterus.Aside from detecting a heartbeat, the point of a 7-week ultrasound is to take measurements of these fetal developments so your doctor has a better idea of where you are in your pregnancy.
That’s why this is often called a dating ultrasound: The measurements are a good indicator of gestational age.
The technician will measure the size of your gestational sac and also take a crown-to-rump measurement of the embryo, if it’s visible. At 7 weeks, your baby should be about 5 to 9 millimeters (mm) in size and the gestational sac will be about 18 to 24 mm.
At this point, fetal development is on a fast track and making large leaps in size from one week to the next.
A gestational sac measuring well below 18 mm will probably reduce your gestational age — that is, your doctor might tell you you’re only 5 or 6 weeks pregnant, not 7. The opposite is true for a sac that measures much larger than 24 mm.
Keep in mind that ultrasounds aren’t a perfect diagnostic tool, and things like the position of your baby can affect the accuracy of the measurements — or whether your technician is able to take them at all.
If the results are inconclusive, your doctor may ask you to schedule another ultrasound in 1 or 2 weeks to try again.
Considering that most people don’t realize they’re pregnant until they’re at least 3 or 4 weeks in — and the gestational sac is the very first thing to form in your uterus — it’s likely that by the time of your ultrasound, you’ll see at least this initial development with a healthy pregnancy.
But you may not be able to see a yolk sac, the fetal pole, the early shape of your baby, or your baby’s heartbeat yet. And if you don’t, try not to worry.
You could be earlier in your pregnancy than you’d first assumed, with a later ovulation window than you’d thought. You could also have a tilted uterus, which can make it harder to see your baby until they’re a little bigger.
That said, the 7-week ultrasound could also reveal a hard truth about the health of your pregnancy.
If there are no signs of pregnancy or inconsistent signs, like a large gestational sac without any yolk sac or fetal pole, it may mean you have a blighted ovum or are otherwise miscarrying. This is very common in the earliest weeks of pregnancy, when the risk is the highest.
If you’re still experiencing early pregnancy symptoms but no fetal growth at all can be found in your uterus, your technician will probably look for signs of an ectopic pregnancy. This may be done along with blood tests and a pelvic exam.
Yes, especially if they’re fraternal. Figuring out how many babies are growing in your uterus is one of the main reasons for having an early ultrasound.
If your twins are fraternal — meaning, two different eggs were fertilized — there will be a separate gestational sac for each baby. If you’re estimating your pregnancy accurately, multiple sacs should be pretty visible on a transvaginal ultrasound at 7 weeks.
If your twins are identical — meaning, one egg was fertilized but then split in two — there’ll only be one gestational sac; however, more than one yolk sac, fetal pole, and heartbeat may be visible.
Again, keep in mind that ultrasounds aren’t foolproof. You may not be far enough along in your pregnancy for all these things to be detected.
And remember that babies like to hide, especially when they have a sibling to hide behind! Multiple gestational sacs may not be visible until a later ultrasound.
Resist the temptation to be alarmed if your doctor orders a 7-week ultrasound; there are several good reasons this test is helpful in the early weeks of pregnancy.
It’s an uncomfortable but harmless procedure that offers important information, including whether your pregnancy is still viable and, if so, exactly how far along you are (and how many babies are growing).
What You Should See (and Why You May Not)
Your first pregnancy ultrasound is usually an exciting event: You’re 12 or 13 weeks pregnant and looking forward to getting a glimpse of the baby that’s been growing for the last 3 months. You know they’re going to look like an alien, but still — they’ll be your little alien, and you can’t wait.
Sometimes, though, an earlier ultrasound is necessary, and we’ll be honest: It’s weird.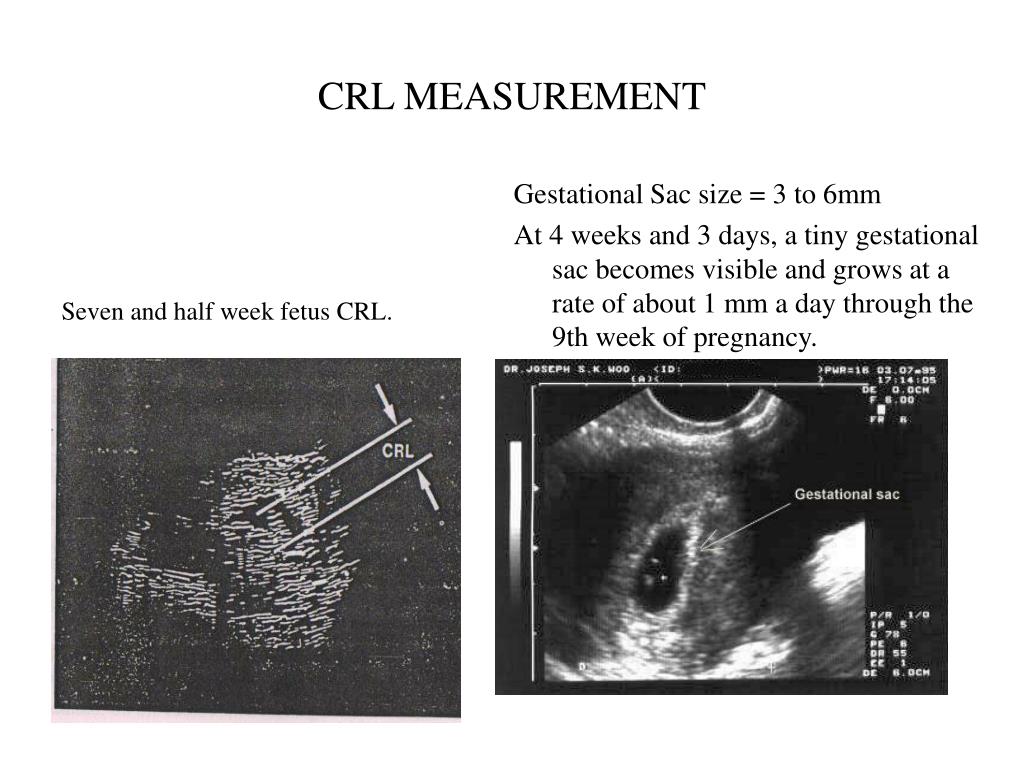 Why? Because a ton of gestational development happens between 7 and 12 weeks, making an early ultrasound a completely different experience than the traditional one in your first trimester.
Why? Because a ton of gestational development happens between 7 and 12 weeks, making an early ultrasound a completely different experience than the traditional one in your first trimester.
A 7-week ultrasound may not be the bonding experience you’re hoping for, since there’s a lot you may not see. But here’s what you can expect.
Although a 7-week ultrasound isn’t routinely performed, there are actually a bunch of reasons why your doctor might want you to have one — and not all of them fall into the “doom and gloom” category.
In fact, the most common reason doctors order ultrasounds before the 12- or 13-week point is to accurately date your pregnancy.
If your pregnancy symptoms don’t match up with your last menstrual period or there’s any confusion about how old your baby is — gestationally speaking — the measurements taken during an early ultrasound can tell your doctor exactly how far along you are in your pregnancy.
Other reasons for an early ultrasound include:
- Confirming twins or multiples. Especially if you’ve had fertility treatments, this might be something you want to confirm ASAP.
- Confirming fetal heartbeat. If you’ve had any concerning symptoms, like spotting or vaginal bleeding, your doctor will want to know if you’re experiencing a miscarriage or what the cause of any unexplained bleeding could be.
- Ruling out an ectopic pregnancy. When an embryo implants outside the uterus, you’ll often have pregnancy symptoms and a positive pregnancy test, even though the embryo isn’t viable. An ectopic pregnancy is a life threatening condition if it’s not treated, so it’s important to diagnose it.
- Checking your reproductive anatomy. Issues with your uterus, cervix, ovaries, or fallopian tubes can cause complications during pregnancy. So, if your doctor suspects you might have a problem — like uterine fibroids, for example — they may want to have that info right away.
 Especially if you’ve had fertility treatments, this might be something you want to confirm ASAP.
Especially if you’ve had fertility treatments, this might be something you want to confirm ASAP.Again, it isn’t cause for immediate panic if your doctor orders a 7-week ultrasound. Yes, it could be a worst-case scenario, but it could also just be one where you’re collecting as much info as possible so you can have a healthy pregnancy.
Yes, it could be a worst-case scenario, but it could also just be one where you’re collecting as much info as possible so you can have a healthy pregnancy.
Pop culture has likely taught you that your first ultrasound is a beautiful experience where a technician waves a magic wand over your stomach and you get to stare at a computer screen and see the adorable shape of your baby floating peacefully in your uterus.
But that’s not what happens at a 7-week ultrasound, so let’s just blow that expectation out of the water now. (Sorry!) In most cases, your baby is too small to be seen clearly — or at all — on an external abdominal ultrasound. Instead, you’ll need a transvaginal ultrasound.
It sounds less than fun, we admit, and it is a less-than-fun procedure: A technician inserts an ultrasound wand, called a transducer, a few inches into your vagina until it reaches your cervix.
Then, the technician keeps it in place, adjusting the wand as much as needed to get a good look at the inside of your uterus. It’s not painful, though it may be uncomfortable.
It’s not painful, though it may be uncomfortable.
You’ll feel about as much pressure as you do during your annual gynecology exam, for comparison. It does take longer, which can add to the overall unpleasantness, but the technicians are trained to make you comfortable — at least, as comfortable as you can be with an ultrasound wand inside in your vaginal canal.
The good news? There’s no risk to your baby from the procedure and there’s no radiation used. So, while it won’t go down in history as one of your favorite experiences, it can’t cause any harm.
Share on PinterestHave a nice day Photo/Shutterstock
A 7-week ultrasound showing crown rump length of baby, which helps figure out the age of the fetus. Surrounding the fetus is the gestational sac, which is filled with fluid.
You’re not going to be counting fingers and toes at this ultrasound; the embryo is simply too tiny for clear images to be detected. You may see the general shape of your baby or be able to tell something is there, but it’s also normal to not see anything that looks very much like a baby at all.
One thing you will often see in a healthy pregnancy is your baby’s heartbeat. It could be going as fast as 110 beats per minute or more! If your baby is in a visible position on the ultrasound, you’ll probably see a little blinking or pulsing on the screen (and you should be able to hear it briefly, too).
You may see the following anatomical developments on a 7-week ultrasound:
- Gestational sac. This is one of the earliest visible signs of a pregnancy, and it refers to the fluid-filled space surrounding the embryo. It’s usually formed by 5 weeks of gestation, and it can accurately confirm an intrauterine pregnancy the vast majority of the time it’s seen on an ultrasound. It will look like a clear, dark circular or oblong shape, sharply contrasted with the whitish, opaque appearance of the inside of your uterus.
- Yolk sac. Even before you can see an embryo inside the gestational sac, you should spot the yolk sac. It’s the first thing to develop inside the gestational sac, and it provides your baby with nutrients and oxygen until the placenta develops. It’ll look like a small white ring or bubble inside the sac.
- Fetal pole. This is the first indication that your baby is forming inside the gestational sac. It will look like a thick, whitish shape attached to the yolk sac. Depending on how far along you are, it may be curved or oblong. It can usually be detected by 6 weeks of gestation on a transvaginal ultrasound. This is where you would see the baby’s heartbeat.
 It’ll look like a small white ring or bubble inside the sac.
It’ll look like a small white ring or bubble inside the sac.Aside from detecting a heartbeat, the point of a 7-week ultrasound is to take measurements of these fetal developments so your doctor has a better idea of where you are in your pregnancy.
That’s why this is often called a dating ultrasound: The measurements are a good indicator of gestational age.
The technician will measure the size of your gestational sac and also take a crown-to-rump measurement of the embryo, if it’s visible. At 7 weeks, your baby should be about 5 to 9 millimeters (mm) in size and the gestational sac will be about 18 to 24 mm.
At this point, fetal development is on a fast track and making large leaps in size from one week to the next.
A gestational sac measuring well below 18 mm will probably reduce your gestational age — that is, your doctor might tell you you’re only 5 or 6 weeks pregnant, not 7. The opposite is true for a sac that measures much larger than 24 mm.
Keep in mind that ultrasounds aren’t a perfect diagnostic tool, and things like the position of your baby can affect the accuracy of the measurements — or whether your technician is able to take them at all.
If the results are inconclusive, your doctor may ask you to schedule another ultrasound in 1 or 2 weeks to try again.
Considering that most people don’t realize they’re pregnant until they’re at least 3 or 4 weeks in — and the gestational sac is the very first thing to form in your uterus — it’s likely that by the time of your ultrasound, you’ll see at least this initial development with a healthy pregnancy.
But you may not be able to see a yolk sac, the fetal pole, the early shape of your baby, or your baby’s heartbeat yet. And if you don’t, try not to worry.
And if you don’t, try not to worry.
You could be earlier in your pregnancy than you’d first assumed, with a later ovulation window than you’d thought. You could also have a tilted uterus, which can make it harder to see your baby until they’re a little bigger.
That said, the 7-week ultrasound could also reveal a hard truth about the health of your pregnancy.
If there are no signs of pregnancy or inconsistent signs, like a large gestational sac without any yolk sac or fetal pole, it may mean you have a blighted ovum or are otherwise miscarrying. This is very common in the earliest weeks of pregnancy, when the risk is the highest.
If you’re still experiencing early pregnancy symptoms but no fetal growth at all can be found in your uterus, your technician will probably look for signs of an ectopic pregnancy. This may be done along with blood tests and a pelvic exam.
Yes, especially if they’re fraternal. Figuring out how many babies are growing in your uterus is one of the main reasons for having an early ultrasound.
If your twins are fraternal — meaning, two different eggs were fertilized — there will be a separate gestational sac for each baby. If you’re estimating your pregnancy accurately, multiple sacs should be pretty visible on a transvaginal ultrasound at 7 weeks.
If your twins are identical — meaning, one egg was fertilized but then split in two — there’ll only be one gestational sac; however, more than one yolk sac, fetal pole, and heartbeat may be visible.
Again, keep in mind that ultrasounds aren’t foolproof. You may not be far enough along in your pregnancy for all these things to be detected.
And remember that babies like to hide, especially when they have a sibling to hide behind! Multiple gestational sacs may not be visible until a later ultrasound.
Resist the temptation to be alarmed if your doctor orders a 7-week ultrasound; there are several good reasons this test is helpful in the early weeks of pregnancy.
It’s an uncomfortable but harmless procedure that offers important information, including whether your pregnancy is still viable and, if so, exactly how far along you are (and how many babies are growing).
A modern view on the problem of non-developing pregnancy | Andreeva
Etiology and pathogenesis of non-developing pregnancy (NB)
NB is included in the structure of reproductive losses and is an urgent obstetric problem. The prevalence of spontaneous interruption of gestation in Russia is one fourth of all recorded pregnancies, while NB accounts for 45 to 88.6% [1][2]. The most relevant period for the study of NB is the first trimester of gestation, since most of the cases of NB (up to 80%) occur precisely in it [1].
Chromosomal aberrations play a special role in the etiology of HB [1][3]. Autosomal trisomy is responsible for more than half of pathological karyotypes. Monosomy is detected in 20–25% of cases [4]. Translocation (2-10%) can cause NB in cases where a married couple has repeated cases of NB or spontaneous miscarriage [4].
In 10-25% of women with recurrent miscarriage, examination reveals congenital anomalies in the structure of the uterus [1][5]. Acquired defects in the anatomical structure (isthmic-cervical insufficiency, myoma with submucous nodes, intrauterine synechia) play a more significant role in the development of NB [6][7].
Acquired defects in the anatomical structure (isthmic-cervical insufficiency, myoma with submucous nodes, intrauterine synechia) play a more significant role in the development of NB [6][7].
Since 2006, based on the resolution of the FIGO World Congress of Obstetricians and Gynecologists, every case of HB should be considered associated with chronic endometritis (CE). CE is a combination of morphological and functional changes in the endometrium of inflammatory origin, which are accompanied by changes in the physiological cyclic transformation and tissue receptivity [8]. In women with miscarriage, the diagnosis of CE was verified by histological examination in 61.0–73.1% of cases [9- 12]. In modern conditions, with XE, viral and bacterial pathogens are often verified, more often as part of a viral-bacterial mixed infection. The chronicity of the inflammatory process in the endometrium is also determined by the growth of microflora resistance to pharmacotherapy.
Numerous studies have shown that ChE acts as a modifier of local immunity.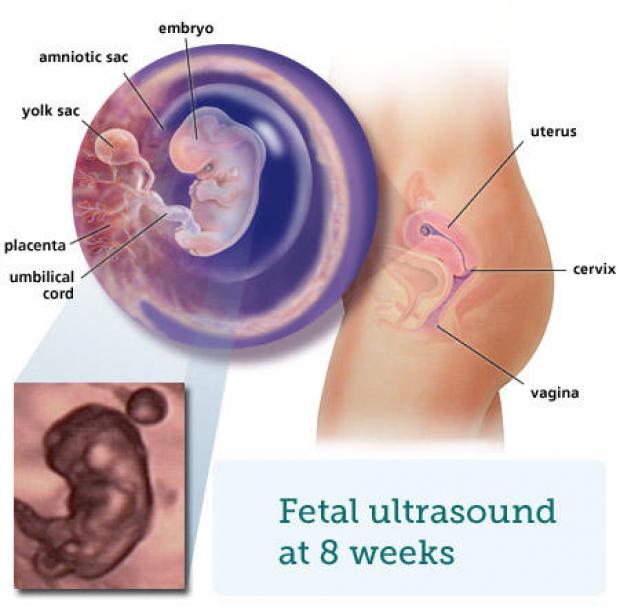 Specific antigens in the endometrial tissue induce the differentiation of T-helpers into two subpopulations: Th-1 and Th-2. Th-1 cells secrete interferon-γ, interleukin-2 (IL-2), and tumor necrosis factor-ß, while Th-2 cells secrete IL-4, IL-5, and IL-10. Both subpopulations are responsible for the production of tumor necrosis factor-α with the predominant influence of Th2 [10][9][13]. The physiological course of pregnancy is provided by humoral immune responses of the Th3 type. In turn, the cellular link of Th2-type immunity can have an abortive effect.
Specific antigens in the endometrial tissue induce the differentiation of T-helpers into two subpopulations: Th-1 and Th-2. Th-1 cells secrete interferon-γ, interleukin-2 (IL-2), and tumor necrosis factor-ß, while Th-2 cells secrete IL-4, IL-5, and IL-10. Both subpopulations are responsible for the production of tumor necrosis factor-α with the predominant influence of Th2 [10][9][13]. The physiological course of pregnancy is provided by humoral immune responses of the Th3 type. In turn, the cellular link of Th2-type immunity can have an abortive effect.
Abnormal activation of NK cells and macrophages contributes to fetal loss. NK cells are directly involved in the dissolution of the trophoblast. Increased production and secretion of cytokines caused by macrophage activation affects NK cells [9][12]. Proteins involved in the inflammatory response, proliferation and apoptosis in the endometrium during the “implantation window” are determined by the expression of 25 genes. It has been shown that in patients with CE, the activity of genes directly encoding pro-inflammatory cytokines, growth factors, and apoptosis processes is significantly altered. Thus, the expression of IGFBR1, BCL2, and BAX increased, while the expression of IL-11, CC 14, IGF-1, and CASP8 decreased [3]. Modification of gene activity in the endometrium in CE causes a decrease in its receptivity, which can be a likely cause of HB.
Thus, the expression of IGFBR1, BCL2, and BAX increased, while the expression of IL-11, CC 14, IGF-1, and CASP8 decreased [3]. Modification of gene activity in the endometrium in CE causes a decrease in its receptivity, which can be a likely cause of HB.
The concept of endometrial receptivity is directly associated with the formation of pinopodium in it and an increase in the level of progesterone, LIF, leukemia inhibitory factor receptor (LIFR), and integrin αVβ3 [13]. Inhibition of the HOXA 10 genes leads to a sharp decrease in the number of pinopodiums [13]. They also regulate endometrial stromal cell proliferation and epithelial cell morphogenesis. At the point of pinopodium formation, the embryo and endometrium carry out signaling interaction [11, 13]. Interleukin-6, LIF, which are important components of blastocyst development and implantation, are expressed on pinopodium [3]. The implementation of the effects of LIF is achieved through receptors consisting of LIFR and gp130 (transmembrane proteins).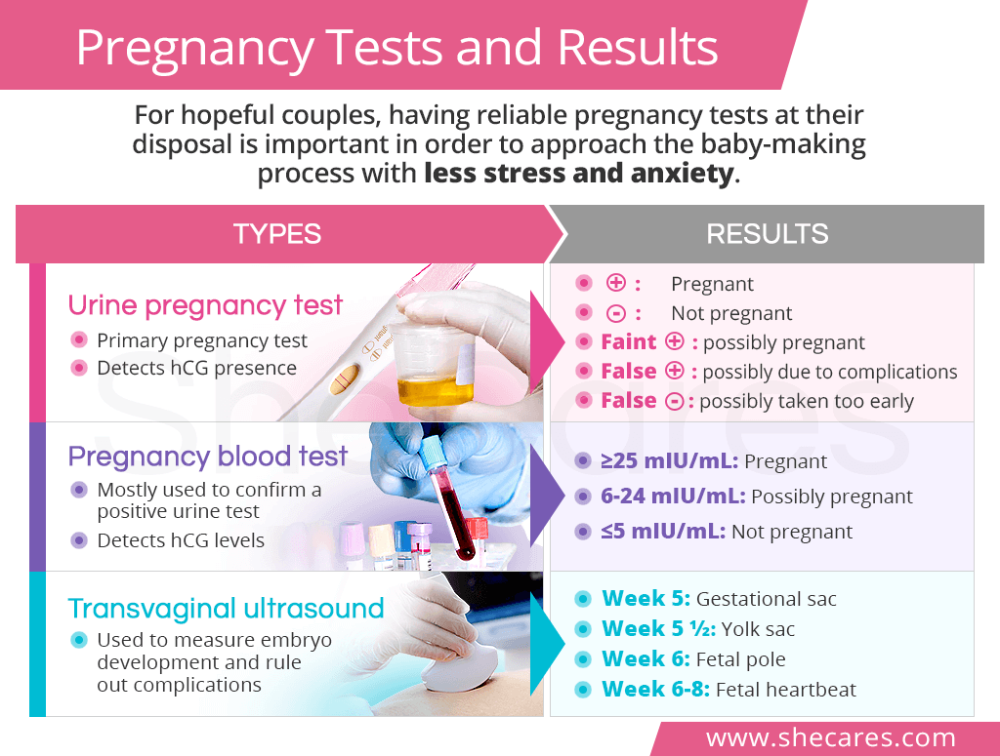 LIF is responsible for the activation of JAK/STAT, MAPK, and PIPK signaling pathways in various cell types [3]. Thus, in the endometrium of mice homozygous for the defective LIF gene, blastocyst implantation did not occur, which confirms the effect of LIF on implantation in general [3].
LIF is responsible for the activation of JAK/STAT, MAPK, and PIPK signaling pathways in various cell types [3]. Thus, in the endometrium of mice homozygous for the defective LIF gene, blastocyst implantation did not occur, which confirms the effect of LIF on implantation in general [3].
In CE, the sensitivity of the endometrium to progesterone decreases, which is a possible mechanism for the violation of its generative function [14]. Degradation of estrogen and activation of growth factors (EGF, TGFα, β, VEGF) in a long-term inflammatory process causes a local increase in estrogen concentration, leading to excessive proliferation of the endometrium [14][15]. The latter is not capable of adequate secretory transformation due to a decrease in the number of progesterone receptors in the cells of the endometrial glands, stroma, and also on regulatory Th-lymphocytes [14][15].
In a number of literary sources, convincing data have been obtained on the significant role of endometrial proteins in implantation processes, the most significant of which is a-2-fertility microglobulin (AMGF).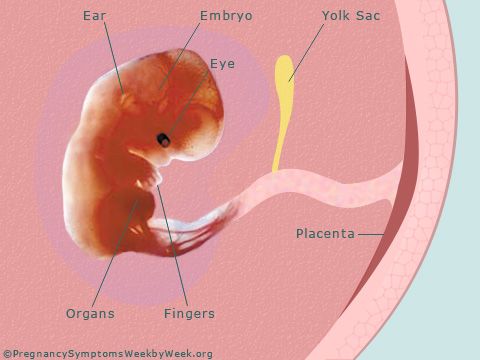 AMHF is an indicator of the activity of the uterine glands, and placental α1-microglobulin (PAMG) is an indicator of endometrial decidualization [1][2]. In CE, endometrial production of proteins with immunosuppressive action (AMHF, PAMG) is reduced [16].
AMHF is an indicator of the activity of the uterine glands, and placental α1-microglobulin (PAMG) is an indicator of endometrial decidualization [1][2]. In CE, endometrial production of proteins with immunosuppressive action (AMHF, PAMG) is reduced [16].
NB ultrasound
Currently, ultrasound (ultrasound) is the most informative method for diagnosing non-developing uterine pregnancy. When performing a sonographic study, it is necessary to differentiate frozen from progressive gestation and exclude ectopic pregnancy. In the early stages, preference is given to transvaginal ultrasound, if it is impossible, sonography is performed transabdominally.
In terms of ultrasound, there are two variants of NB: – anembryony and early death of the embryo (fetus). On fig. 1 shows the state of anembryony.
Figure 1. Transvaginal ultrasound. Pregnancy 7 weeks and 5 days. The diameter of the fetal egg is 25 mm. Anembryony.
Figure 1 .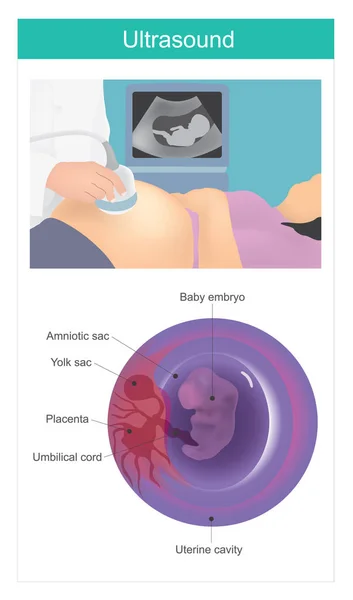 Transvaginal ultrasound examination. Pregnancy 7 weeks and 5 days. The diameter of the ovum is 25 mm. Anembryony.
Transvaginal ultrasound examination. Pregnancy 7 weeks and 5 days. The diameter of the ovum is 25 mm. Anembryony.
When performing an ultrasound examination, it is necessary to differentiate frozen from progressive gestation and exclude ectopic localization. Figure 2 shows an example of an undeveloped pregnancy at 6 weeks and 4 days.
Figure 2. Transvaginal ultrasound. Pregnancy 6 weeks and 4 days. There is no heartbeat. Non-developing pregnancy.
Figure 2 . Transvaginal ultrasound examination. Pregnancy 6 weeks and 4 days. There is no heartbeat. Non-developing pregnancy
In the early stages, preference is given to transvaginal ultrasound, if it is impossible, sonography is performed transabdominally.
Ultrasound data allow us to differentiate between two types of anembryony [1]. Type I anembryony is characterized by the absence of an embryo, the fetal egg is up to 20-25 mm, the uterus corresponds to 5-7 weeks of pregnancy. At the same time, the parameters of the uterus and the fetal egg do not correspond to the gestational age, and dynamic observation does not change the characteristics. The growth rate of the fetal egg in type II anembryonia is normal, but the embryo is absent or its remains can be fixed in the form of a thin hyperechoic line (“vertebral fold”). At a period of 10-11 weeks of pregnancy, the fetal egg reaches 45-55 mm in diameter, but already from the 8th week it is not possible to verify the laying of the villous chorion. On fig. 3 shows the early death of the embryo.
At the same time, the parameters of the uterus and the fetal egg do not correspond to the gestational age, and dynamic observation does not change the characteristics. The growth rate of the fetal egg in type II anembryonia is normal, but the embryo is absent or its remains can be fixed in the form of a thin hyperechoic line (“vertebral fold”). At a period of 10-11 weeks of pregnancy, the fetal egg reaches 45-55 mm in diameter, but already from the 8th week it is not possible to verify the laying of the villous chorion. On fig. 3 shows the early death of the embryo.
Fig.3. Transvaginal ultrasound. Pregnancy 8 weeks and 2 days. Non-developing pregnancy (early death of the embryo).
3. Transvaginal ultrasound examination. Pregnancy 8 weeks and 2 days. Non-developing pregnancy (early death of the embryo).
The following ultrasound diagnostic criteria for non-developing pregnancy are defined: 1) the fetal heartbeat with its coccyx-parietal size (CTE) of 7 mm or more is not recorded; 2) there is no embryo with an average diameter of the fetal egg of 25 mm or more [17][18].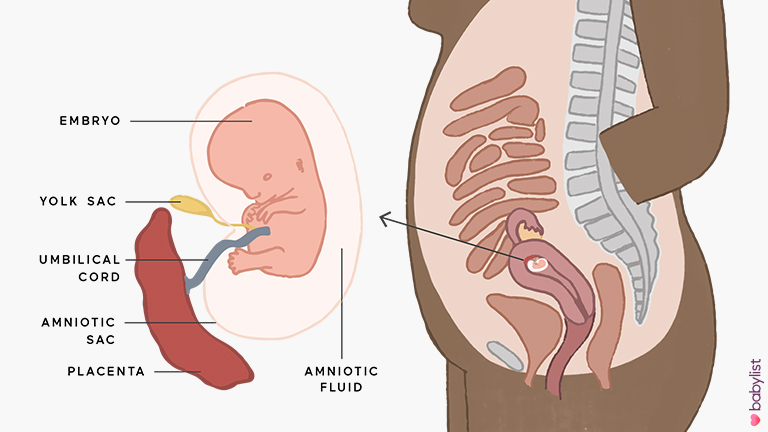 Without fail, the diameter of the fetal egg is measured in three projections, and then its average value is calculated. If at least one of the above criteria is present, the diagnosis of NB is made [18], but confirmation by a second ultrasound specialist is required 1 . The working group of the National Institute for Health and Care Excellence (NICE) is also considering the possibility of re-examination of the patient after 7–14 days for a final conclusion [18].
Without fail, the diameter of the fetal egg is measured in three projections, and then its average value is calculated. If at least one of the above criteria is present, the diagnosis of NB is made [18], but confirmation by a second ultrasound specialist is required 1 . The working group of the National Institute for Health and Care Excellence (NICE) is also considering the possibility of re-examination of the patient after 7–14 days for a final conclusion [18].
Ultrasound criteria for NB during repeated studies: 1) absence of an embryo with a heartbeat 2 weeks or more after the discovery of a gestational sac without a yolk sac; 2) the absence of an embryo with a heartbeat 11 days or more after the discovery of a fetal egg with a yolk sac [17][18][19].
There are also prognostic ultrasound criteria for NB: 1) absence of fetal heartbeat with CTE less than 7 mm; 2) the absence of an embryo with an average diameter of the fetal sac of 16–24 mm; 3) the absence of an embryo with a heartbeat 7–13 days after the detection of a fetal egg without a yolk sac; 4) the absence of an embryo with a heartbeat 7–10 days after the discovery of a fetal egg with a yolk sac; 5) the absence of an embryo after 6 weeks. from the beginning of the last menstruation; 6) the size of the yolk sac is more than 7 mm; 7) discrepancy between the size of the fetal sac and the size of the embryo (the difference between the average diameter of the fetal sac and the CTE of the fetus is less than 5 mm) [1][17][19].
from the beginning of the last menstruation; 6) the size of the yolk sac is more than 7 mm; 7) discrepancy between the size of the fetal sac and the size of the embryo (the difference between the average diameter of the fetal sac and the CTE of the fetus is less than 5 mm) [1][17][19].
These signs only suggest NB, and dynamic ultrasonography is needed to confirm or rule it out. Some researchers point out that it is inappropriate to use the calculation of the difference between the diameter of the fetal egg and CTE as a prognostic criterion [20], and the phenomenon of “yolk stalk sign” has additional value [21][22]. The yolk stalk is a tubular structure that connects the yolk sac and the body of the embryo. In the early stages of gestation, they are located close to each other, so the yolk stalk cannot normally be visualized. If the embryo without a heartbeat begins to separate from the yolk sac, before reaching CTE values of 5 mm or more, then in this situation they speak of the phenomenon of the “yolk stalk”. The results of studies confirm the correlation of this symptom with missed pregnancy in the dynamic observation of patients [21][22].
The results of studies confirm the correlation of this symptom with missed pregnancy in the dynamic observation of patients [21][22].
Therapeutic tactics in NB
The traditional tactic in NB is the surgical removal of the dead fetal egg, while the endometrial repair process takes longer than after artificial abortion [2]. Therefore, an important direction in the study of the problem of HB is the search and development of new approaches to the management of patients after emptying the uterine cavity in order to reduce the frequency of infectious complications and prevent chronic inflammation. In this regard, attention is drawn to the possibility of using quantum therapy (CT) in the postoperative period in patients with NB [23][24].
The CT method based on magnetic infrared laser therapy contributes to the normalization of all parts of the regulation of the adrenal glands, reproductive, immune and other systems [23][24]. Under the influence of low-intensity pulsed laser radiation, a total reaction of organs and tissues is generated, which causes an analgesic and anti-inflammatory effect. The functionality of the microvasculature improves, the repair processes are accelerated. The activity of specific and non-specific links of immunity is stimulated. The excitability of the vegetative centers is reduced. The trophism of damaged tissues improves against the background of an increase in the general level of adaptation of the organism [23][24]. At the level of individual organs and tissues, including the uterus, receptor sensitivity increases, the duration of the phase of inflammation and interstitial tissue edema decreases, etc. [23][24]
The functionality of the microvasculature improves, the repair processes are accelerated. The activity of specific and non-specific links of immunity is stimulated. The excitability of the vegetative centers is reduced. The trophism of damaged tissues improves against the background of an increase in the general level of adaptation of the organism [23][24]. At the level of individual organs and tissues, including the uterus, receptor sensitivity increases, the duration of the phase of inflammation and interstitial tissue edema decreases, etc. [23][24]
The above effects of CT, the positive experience of using it for the treatment of wound infection and chronic inflammatory processes [23][24] of other localization determine the scientific and practical interest in knowing the possibilities of using CT in patients after NB interruption in order to prevent chronic inflammation and its recurrence .
1. Letter of the Russian Ministry of Health of 06/07/2016 No. 15-4/10/2-3482 “Miscarriage in the early stages of pregnancy: diagnosis and management tactics”.
1. Non-progressive pregnancy: MARS (Interdisciplinary Association of Reproductive Medicine) Guidelines. Aut.-stat. V.E. Radzinsky et al. – M .: Editorial staff of Status Praesens, 2015.
2. Radzinsky V.E., Dimitrova V.I., Maiskova I.Yu. Non-developing pregnancy. – M.: GEOTAR-Media; 2009.
3. Di Pietro C., Cicinelli E., Guglielmino M.R., Ragusa M., Farina M., et al. Altered transcriptional regulation of cytokines, growth factors, and apoptotic proteins in the endometrium of infertile women with chronic endometritis. // Am J Reprod Immunol. – 2013. – V.69, No. 5. – P.509–517. https://doi.org/10.1111/aji.12076
4. Sugiura-Ogasawara M., Ozaki Y., Katano K., Suzumori N., Kitaori T., Mizutani E. Abnormal Embryonic Karyotype is the Most Frequent Cause of Recurrent Miscarriage. // Hum reproduction. – 2012. – V.27, No. 8. – P.2297–2302. https://doi.org/10.1093/humrep/des179
5. Tabolova V.K., Korneeva I.E. Influence of chronic endometritis on the outcomes of assisted reproductive technology programs: morpho-functional and molecular genetic features. // Obstetrics and gynecology. – 2013. – No. 10. – P.17-22. eLIBRARY ID: 20841398
// Obstetrics and gynecology. – 2013. – No. 10. – P.17-22. eLIBRARY ID: 20841398
6. Obstetrics. National leadership. Under. ed. E.K. Ailamazyan, V.I. Kulakova, V.E. Radzinsky, G.M. Savelyeva. – M.: GEOTAR-Media; 2009.
7. Puscheck E.E., Scott Lucidi R. FACOG Early Pregnancy Loss Workup / Updated: Jun 08, 2018. – URL: https://reference.medscape.com/article/266317-workup
8. Kogan E .A., Demura T.A., Vodyanoy V.Ya., Shurshalina A.V. Molecular and morphological aspects of endometrial receptivity disorders in chronic endometritis. // Archive of pathology. – 2012. – No. 3. – P.15–17. eLIBRARY ID: 22288730
9. Andreeva M.V., Neklyudova A.V. Ways to overcome infectious complications in obstetrics. // Vestnik VolgGMU. – 2019. – No. 4 (72). – P.21-25. DOI: 10.19163/1994-9480-2019-4(72)-21-25
10. Early pregnancy. From preconception preparation to healthy gestation. Ed. Radzinsky V.E., Orazmuradova A.A. – Media Bureau “Status Presence”; 2018.
11. Plyasunova M.P., Khlybova S.V. Chronic endometritis as one of the urgent problems in modern gynecology. // Vyatka Medical Bulletin. – 2013. – No. 1 – C.44–53. eLIBRARY ID: 19114243
Plyasunova M.P., Khlybova S.V. Chronic endometritis as one of the urgent problems in modern gynecology. // Vyatka Medical Bulletin. – 2013. – No. 1 – C.44–53. eLIBRARY ID: 19114243
12. Sukhikh G.T., Shurshalina A.V. Chronic endometritis. Management. – M.: GEOTAR-Media; 2013.
13. Dimitriadis E., Nie G., Hannan P., Paiva P., Salamonsen LA. Local regulation of implantation at the human fetal-maternal interface. // Int J Dev Biol. – 2010. – V.54. – P.313–322. DOI: 10.1387/ijdb.082772ed
14. Mote P.A., Balleine R.L., McGowan E.M., Clarke C.L. Colocalization of progesterone receptors A and B by dual immunofl uorescent histochemistry in human endometrium during the menstrual cycle. // J Clin Endoc Metab.- 1999. – V.84, No. 8. – P.2963-2971. DOI: 10.1210/jcem.84.8.5928
15. Sivko T.S., Andreeva M.V., Gadzhieva A.Kh. Non-developing pregnancy as a cause of reproductive losses. // Almanac-2019: collection of articles. – 2019. – P.228-230.
16. Kitaya K., Yasuo T. Immunohistochemistrical and clinicopathological characterization of chronic endometritis. // Am J Reprod Immunol. – 2011. – V.66, No. 5. – P.410–415. DOI: 10.1111/j.1600-0897.2011.01051.x
Immunohistochemistrical and clinicopathological characterization of chronic endometritis. // Am J Reprod Immunol. – 2011. – V.66, No. 5. – P.410–415. DOI: 10.1111/j.1600-0897.2011.01051.x
17. Murugan VA, Murphy BO, Dupuis C, Goldstein A, Kim YH. Role of ultrasound in the evaluation of fi rst-trimester pregnancies in the acute setting. // ultrasonography. – 2020. – V.39, №2. – P.178-189. DOI: 10.14366/usg.19043
18. NICE guideline [NG126]. Ectopic pregnancy and miscarriage: diagnosis and initial management. Published date: 17 April 2019. Accessed at: https://www.nice.org.uk/guidance/ng126.
19. Preisler J., Kopeika J., Ismail L., Vathanan V., Farren J., et al. Defining safe criteria to diagnose miscarriage: prospective observational multicentre study. // BMJ. – 2015. – V.351. – P.4579. DOI: 10.1136/bmj.h5579.
20. Kapfh amer J.D., Palaniappan S., Summers K., Kassel K., Mancuso A.C., et al. Diff erence between mean gestational sac diameter and crown-rump length as a marker of fi rsttrimester pregnancy loss aft er in vitro fertilization.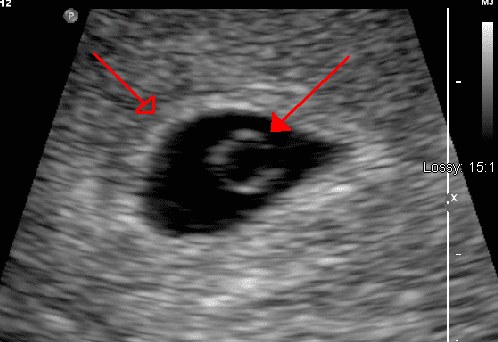 // Fertil Steril. – 2018. – V.109,№1. – P.130-136. DOI: 10.1016/j.fertnstert.2017.09.031
// Fertil Steril. – 2018. – V.109,№1. – P.130-136. DOI: 10.1016/j.fertnstert.2017.09.031
21. Filly M.R., Callen P.W., Yegul N.T., Filly R.A. Th e yolk stalk sign: evidence of death in small embryos without heartbeats. J Ultrasound Med. – 2010. – V.29, No. 2. – P.237-41. DOI: 10.7863/jum.2010.29.2.237
22. Acuña J., Rukh S., Adhikari S. Point-of-care ultrasound identification of yolk stalk sign in a case of failed fi rst trimester pregnancy. World J Emerge Med. – 2018. – V.9, No. 2. – P.149-151. DOI: 10.5847/wjem.j.1920-8642.2018.02.012
23. Melkozerova O.A., Bashmakova N.V., Pogorelko D.V., Chistyakov M.A. The energy of low-frequency ultrasound in the restoration of the receptor field of the endometrium after an undeveloped pregnancy. // Obstetrics and gynecology. – 2014. – No. 7. – P.61-67. eLIBRARY ID: 21801006
24. Zubarev PN, Risman BV. [Ultrasonic cavitation and ozonization in treatment of patients with pyo-necrotic complications of diabetic foot syndrome]. Vestn Khir Im I I Grek. 2011;170(1):48-53. (In Russ.). PMID: 21506355.
Vestn Khir Im I I Grek. 2011;170(1):48-53. (In Russ.). PMID: 21506355.
Non-developing early pregnancy. / News / RDC
The main unresolved problems in obstetrics and gynecology to date, making a significant negative contribution to reproductive losses, are the lack of a decrease in the number of preterm births (termination of pregnancy after 22 weeks) and an increase in the frequency of spontaneous miscarriages (up to 22 weeks).
Currently, non-developing pregnancy is usually considered as a polyetiological complication of pregnancy, which is based on a pathological symptom complex: lack of vital activity of the embryo, endometrial dysfunction and disturbances in the hemostasis system of a pregnant woman. Back at 19In 1995 Professor Stuart Campbell stated that: “Early death of the embryo should be given the same importance as late fetal death.” Unfortunately, at the present time, this phrase has acquired a special meaning, since we live in an era of an “epidemic” of non-developing pregnancies. Their frequency among cases of spontaneous miscarriages in the early stages has increased over the past 30 years from 10-20% in the late 90s of the last century to 45-88.6% in recent years. Therefore, the issues of the earliest and most accurate diagnosis of an undeveloped pregnancy become extremely relevant.
Their frequency among cases of spontaneous miscarriages in the early stages has increased over the past 30 years from 10-20% in the late 90s of the last century to 45-88.6% in recent years. Therefore, the issues of the earliest and most accurate diagnosis of an undeveloped pregnancy become extremely relevant.
Based on clinical signs, it is very difficult to make this diagnosis in the early stages, since its symptoms are not specific. So, for example, slight spotting from the genital tract may appear after a certain interval after the cessation of its development, or may be absent altogether. Not in every case there are pains in the lower abdomen. General malaise, weakness, dizziness, fever are observed only in 10% of women with a delay of a dead fetus in the uterus for more than 3-4 weeks. The most characteristic and long-known subjective signs of the death of the fetal egg in the first trimester of pregnancy are the disappearance of nausea, vomiting, salivation. However, all of the above cannot be considered reliable symptoms of a missed pregnancy. The use of biochemical tests, such as serum β-hCG levels, is an aid to differential diagnosis in early pregnancy between conditions such as normal developing uterine pregnancy, non-progressing uterine pregnancy, pregnancy of “unclear localization” and ectopic pregnancy. However, to date, it is recommended to determine the serum level of β-hCG only in the case of “pregnancy of unclear localization”. There is no indication for taking serum β-hCG if the gestational sac is clearly visible in the uterine cavity and we need to confirm the diagnosis of an arrested pregnancy. That is why the priority today is given to ultrasound, which allows you to detect non-developing pregnancy long before the onset of clinical symptoms.
The use of biochemical tests, such as serum β-hCG levels, is an aid to differential diagnosis in early pregnancy between conditions such as normal developing uterine pregnancy, non-progressing uterine pregnancy, pregnancy of “unclear localization” and ectopic pregnancy. However, to date, it is recommended to determine the serum level of β-hCG only in the case of “pregnancy of unclear localization”. There is no indication for taking serum β-hCG if the gestational sac is clearly visible in the uterine cavity and we need to confirm the diagnosis of an arrested pregnancy. That is why the priority today is given to ultrasound, which allows you to detect non-developing pregnancy long before the onset of clinical symptoms.
Diagnostic criteria for non-developing pregnancy in the early stages:
- absence of a heart rhythm in the coccyx-parietal size of the embryo 7 mm or more;
- lack of embryonic structure with an average diameter (arithmetic mean of 3 diameters) of the ovum greater than or equal to 25 mm.

If at least one of the indicated signs is present, the diagnosis is considered final. In this case, repeated ultrasound examinations are not required. The probability that in the period of 12 weeks. fetus will be viable is zero.
There are several more criteria that allow diagnosing a non-developing pregnancy:
- the embryo does not have a heartbeat 14 days after the ultrasound examination revealed a fetal egg without a yolk sac at the initial admission;
- , the embryo has no heartbeat 11 days after the ultrasound revealed a gestational sac with a yolk sac at the initial intake.
Other signs that are described in the medical literature are prognostic. They do not give a 100% guarantee, but only allow you to suspect a missed pregnancy. In this case, additional ultrasound examinations are required to confirm or refute the diagnosis of non-developing pregnancy.
Prognostic criteria for non-developing pregnancy include:
- Embryo CTE < 7 mm, no heartbeat;
- the average diameter of the fetal egg (arithmetic mean of 3 diameters) is 16-24 mm, the embryo is absent;
- Absence of an embryo with a heartbeat 7-10 days after an ultrasound examination revealed a gestational sac without a yolk sac;
- absence of an embryo with a heartbeat 7-10 days after the discovery of a fetal egg with a yolk sac;
- no embryo after 6 weeks. after the first day of the last menstruation;
- abnormal structure of the yolk sac (irregular shape, hyperechoic structure), dimensions more than 7 mm or less than 3 mm;
- small fetal egg relative to the size of the embryo (the difference in size between the above structures is less than 5 mm), the so-called oligohydramnios of the first trimester;
- abnormal contours of the ovum;
- the appearance of the yolk stalk without registration of cardiac activity in the embryo;
- modified amniotic cavity;
- increase in CTE less than 0.2 mm/day;
- fetal bradycardia (M-mode heart rate less than 80-90 beats/min.
 after the first day of the last menstruation;
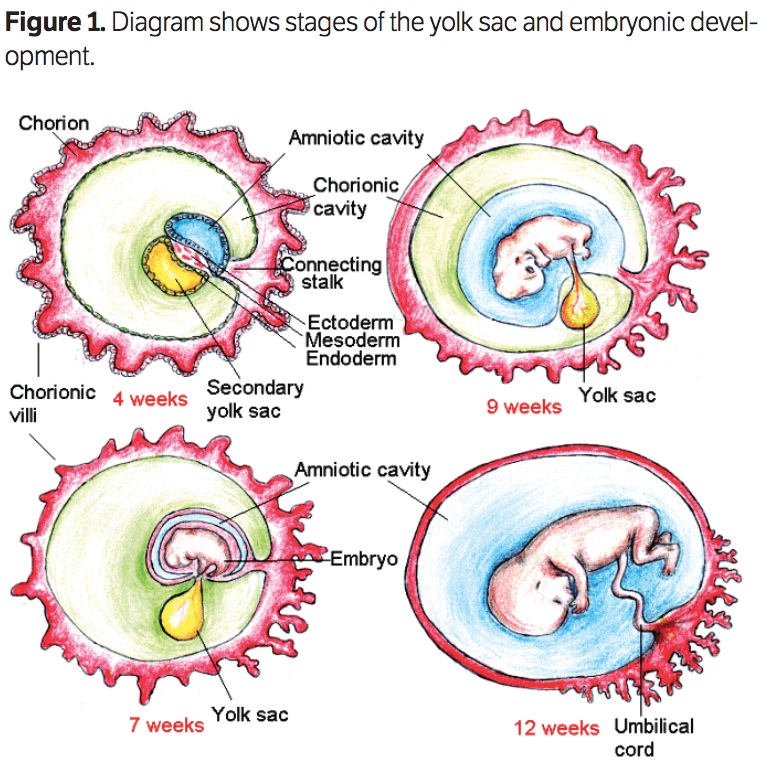
after the first day of the last menstruation; Early ultrasound examinations require both clear methodological approaches and examination safety principles. It is necessary to evaluate the following structures: gestational sac, amniotic cavity, yolk sac and embryo with real-time (B-mode) or M-mode cardiac activity. Up to 10 weeks gestation should not use color Doppler mapping (CDM) to record cardiac activity, as this increases the heat index (TI) to 2. 5-4.2, and according to the ALARA principles governing the safety of ultrasound, scan early in pregnancy not recommended for TI greater than the threshold value of 3.0.
5-4.2, and according to the ALARA principles governing the safety of ultrasound, scan early in pregnancy not recommended for TI greater than the threshold value of 3.0.
An important issue in the ultrasound diagnosis of non-developing pregnancy is the issue of repeated ultrasound examinations. It is necessary to choose the optimal interval for repeating the study, since unreasonable studies in case of suspected non-developing pregnancy increase the burden on the ultrasound diagnostic rooms and the obstetrician-gynecologist and lead to excessive neuroticism of patients who are faced with this problem. It is wise to adhere to the following recommendations.
- If an embryo smaller than 7 mm is visualized during the first ultrasound examination and there is no heartbeat, then a second examination is prescribed no earlier than after 7 days. If during the re-examination cardiac activity is not recorded, then the doctor is authorized to make a diagnosis of “non-developing pregnancy”.
- If the first ultrasound shows an empty gestational sac or a gestational sac with a yolk sac and is > 12 mm, repeat the examination no sooner than 7 days later. If during the re-examination the echographic picture does not change, then it is competent to make a diagnosis of “non-developing pregnancy”.
- If the first ultrasound shows an empty gestational sac or a gestational sac with a yolk sac and is <12 mm, repeat the examination no sooner than 14 days later. If the situation does not change during the re-examination, then the doctor is authorized to make a diagnosis of “non-developing pregnancy”.

If the mean ovum diameter (arithmetic mean of 3 diameters) is > 16 mm and no embryo is visualized, there is a 10% chance that we are dealing with a normal developing uterine pregnancy. If an empty gestational sac is detected on the first transvaginal ultrasound, and a yolk sac appears on the second examination, then there is a 27% chance of a developing pregnancy.